





Clinically significant mitral stenosis in industrialized countries is more often degenerative calcific than rheumatic, and therefore, not suitable for percutaneous mitral commisurotomy.
Cardiac surgery is performed less in older patients with calcific mitral stenosis (MS), respectively mitral annular calcification because of a higher perioperative risk.
Degenerative calcified MS and mitral annulus calcification can form bizarre formations.
A 79-year-old woman was admitted to our hospital because of progressive dyspnoea [New York Heart Association (NYHA) III]. She had a history of diabetes, arterial hypertension, polymyalgia rheumatic, and kidney transplantation 25 years ago. One year earlier a moderate mitral stenosis (MS) with secondary pulmonary hypertension was diagnosed in an ambulatory transthoracic echocardiogram (TTE). Optimal medical treatment including diuretics and a beta-blocker was initiated.
After admission TTE showed a heavy calcified high-grade MS (Figure 1). Systolic left ventricular function was normal. Right heart catheterization confirmed the diagnosis: mitral valve area was calculated 1.0 cm2 by the Gorlin equation. A mean gradient of 15 mmHg and a mean pulmonary pressure of 58 mmHg were measured. Coronary angiogram revealed a high-grade stenosis in LAD and CX. Three-dimensional transoesophageal echocardiogram (3D-TOE) showed that calcified MS formed a bridge from anterior to posterior mitral leaflet with two remaining orifices mimicking a MitraClip® (Figure 2, see Supplementary material online, Videos).

Transthoracic echocardiogram showing a massive calcified mitral stenosis.
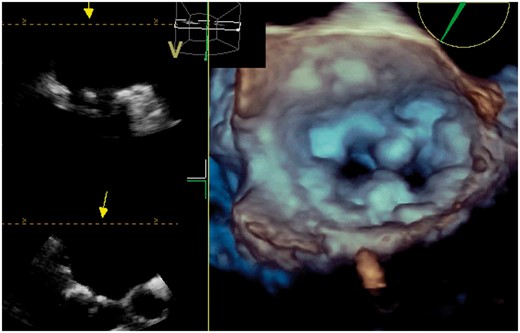
Calcified mitral stenosis imitates a MitraClip® in three-dimensional transoesophageal echocardiogram.
Because of heavy calcification percutaneous mitral commisurotomy (PMC) was no option. The patient refused heart surgery due to high perioperative risk according to the immunosuppressive therapy and other comorbidities. She even declined coronary interventions in absence of angina.
While the incidence of rheumatic MS has decreased in industrialized countries, degenerative calcific stenosis is now encountered mainly in older patients often accompanied by other diseases.1 PMC is the first choice of treatment in clinically significant MS. The degenerative calcific stenosis is often not suitable for this intervention. Cardiac surgery in these patients, however, is associated with higher perioperative risk, especially in older patients with comorbidities.2
Calcification of the mitral valve and the mitral annular calcification are frequently seen in older patients. They are associated with a higher morbidity and mortality and are a strong independent risk factor for stroke.3,4 In some cases the calcifications can form bizarre formations.5 This is the first case documenting that a calcified MS can imitate a MitraClip® in 3D-TOE.
Consent: The author/s confirm that written consent for submission and publication of this case report including image(s) and associated text has been obtained from the patient in line with COPE guidance.
Conflict of interest: none declared.

{kind=link}
{kind=link}
Comments