





Summary
Single coronary arteries (SCA) are seldom encountered in catheterization laboratory. We describe an unusual combination of triple anomaly of origin of SCA from ascending aorta, acute take of right coronary artery (RCA) from SCA and anomalous inter-arterial course. Emergent percutaneous coronary intervention (PCI) was done in anomalous RCA arising from SCA that was arising from ascending aorta.
Case description
A 58-year-old male patient presented with acute onset chest pain for 3 h. His electrocardiogram (ECG) showed ST elevation in inferior leads suggestive of acute inferior wall myocardial infarction. Troponin T test was positive. Selective coronary angiogram showed no vessels arising from right coronary sinus. Angiogram done with Amplatz 2 (AL-2) guide catheter showed single coronary trunk arising from ascending aorta. Right coronary artery was arising at an unusual vertical angle and showed critical stenosis in mid-segment (Figure 1, Supplementary material online, Video S1). RCA was engaged with an extra back up guide (EBU), and PCI was completed with implantation of an 2.75 × 28 mm everolimus-eluting stent (Figure1, Supplementary material online, Video S2). The left ventricle (LV) ejection fraction of the patient at discharge was 45%. Coronary computed tomography (CT) angiography done later confirmed anomalously originating SCA from ascending aorta (Figure 2). The RCA coursed between aorta and pulmonary artery (Figure2).
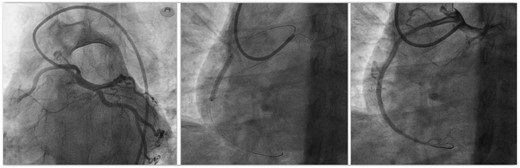
Coronary angiogram of single coronary artery engaged with Amplatz left guide catheter showing normal left anterior descending artery and left circumflex artery and occluded right coronary artery (RCA) arising at an acute angle from the common trunk. It also shows implantation of a drug eluting stent with good result in the anomalous RCA.
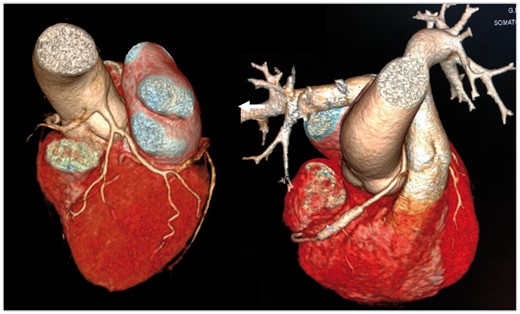
Computed tomography coronary angiography showing origin of single coronary trunk above the left sinus from ascending aorta and normal left coronary system. The right coronary artery (RCA) is coursing between aorta and pulmonary artery. It shows a well deployed stent in mid-RCA.
Incidence of SCA in general population is 0.024%.1 When present, they mostly arise from one of the coronary sinuses. Such solitary coronary ostia is classified into three types.2 Origin of SCA from ascending aorta is extremely rare. Anomalous RCA in such cases rarely traverses can traverse anterior to right ventricle, between the pulmonary artery and aorta (as in present case), in crista supraventricular or dorsal to aorta.2 The present case was a rare coronary anomaly which will be classified as type IB2 as per the Roberts and Shirani classification.2 Such an inter-arterial path is rarely associated with syncope, chest pain, and rarely sudden cardiac death.3 This is due to lateral compression of the artery with phasic and exercise induced worsening of deformity (scissor-like mechanism). If such a course is diagnosed in a non-emergent situation, then surgical intervention may be considered for such patients. Emergent PCI was performed in the present situation as a bail out procedure. PCI in this situation has several technical considerations like choice of guide catheter, its careful manipulation, choice of wire, and use of flexible stent.
The present case describes lifesaving PCI in an anomalously originating, anomalously coursing occluded RCA in an emergent situation.
Consent: The author/s confirm that written consent for submission and publication of this case report including images and associated text has been obtained from the patient in line with COPE guidance.
Conflict of interest: none declared.

{kind=link}
{kind=link}
Comments