






Abstract
Reductions in human immunodeficiency virus (HIV) incidence with pre-exposure prophylaxis (PrEP) for men who have sex with men (MSM) will require significant coverage of those at risk. We propose a simplified framework, similar to the HIV care continuum, to achieve protection with PrEP as follows: 1. At-risk MSM; 2. Awareness of and willingness to take PrEP; 3. Access to healthcare; 4. Receiving a prescription; and 5. Adhering to effective PrEP. We evaluated the PrEP care continuum on an Atlanta cohort of MSM and projected how many MSM might achieve protection from HIV. Even with optimistic estimates, few Atlanta MSM (15%) are projected to achieve protection from HIV with PrEP given the significant barriers described. Each continuum step represents an important point for intervention that could substantially increase the overall effectiveness of PrEP. In addition, novel strategies for PrEP delivery are needed to achieve the necessary effectiveness for Atlanta MSM at risk of HIV.
Men who have sex with men (MSM) continue to be at highest risk for human immunodeficiency virus (HIV) infection in the United States, accounting for 63% of new infections in 2010 [1]. Atlanta, Georgia, had the 5th highest city-specific rate of new HIV diagnoses in 2013 [2] and 2nd highest city-specific number of new HIV diagnoses among MSM in the United States in 2011 [3]. As in other large municipalities, black MSM are disproportionately affected, comprising about 60% of HIV-infected MSM, whereas blacks represent only about 30% of the overall Atlanta population [4]. We recently concluded a longitudinal cohort study of MSM in Atlanta (InvolveMENt) where we documented large HIV disparities between black and white MSM and alarmingly high rates of HIV incidence, particularly among young black MSM [5, 6]. HIV prevalence was 43% among black MSM compared to 13% among white MSM, and black MSM aged 18–25 years had an annualized HIV incidence of 11%. This public health crisis calls for urgent attention and action.
Pre-exposure prophylaxis (PrEP) has been heralded as a potential “game-changer” for HIV prevention efforts. The first successful PrEP clinical trial (iPrex) was conducted among MSM and transgender women and showed efficacy of 44% for daily tenofovir/emtricitabine (TDF/FTC) for prevention of HIV [7, 8]. Although PrEP is an expensive intervention driven largely by drug costs, cost-effectiveness analyses support targeted use in high incidence populations such as MSM [9]. The Centers for Disease Control and Prevention (CDC) released clinical practice guidelines in 2014 for use of PrEP in populations at high risk of HIV infection [10].
Realizing effectiveness of PrEP in reducing HIV incidence will require significant coverage of an at-risk population. Over 10 years, population coverage of 40% of at-risk HIV-negative MSM with PrEP is estimated to prevent approximately 25% of new HIV infections; increasing coverage to 80% results in prevention of approximately 40% of new infections [11]. However, multiple barriers exist to achieving effectiveness of PrEP at individual and population levels, and actual PrEP usage has remained low [12, 13].
Here, we introduce the PrEP care continuum, which conceptualizes these barriers analogously to the HIV care continuum, originally formalized by Gardner et al to depict the necessary steps to achieving viral suppression in HIV-infected individuals, and further refines the HIV prevention continuum proposed by McNairy and El-Sadr [14, 15]. To achieve protection from HIV with PrEP, we propose that the at-risk population must be defined, an at-risk individual must be aware of and willing to take PrEP, must have access to healthcare, must receive a PrEP prescription from a healthcare provider, and must adhere to PrEP. We then apply this PrEP care continuum to a cohort of black and white MSM in Atlanta to estimate how many might achieve protection from HIV with PrEP.
THEORETICAL MODEL FOR THE PREP CARE CONTINUUM
In Figure 1, we propose a theoretical model for the PrEP care continuum. For each step of the continuum, we list factors relevant to PrEP uptake and potential interventions to enhance uptake. This model is not exhaustive but rather is intended to facilitate categorization of interventions and conceptualization of systems-based approaches to enhance PrEP uptake. In the model, each “factor” has the potential to constrain PrEP effectiveness, and each “intervention” has the potential to ameliorate a constraint. In order to prioritize the wide range of interventions that may be needed to bring PrEP to scale in the United States, it is necessary to measure and understand the factors that serve to constrain PrEP scale-up and effectiveness. Below, we explore in more detail each step in the PrEP care continuum.
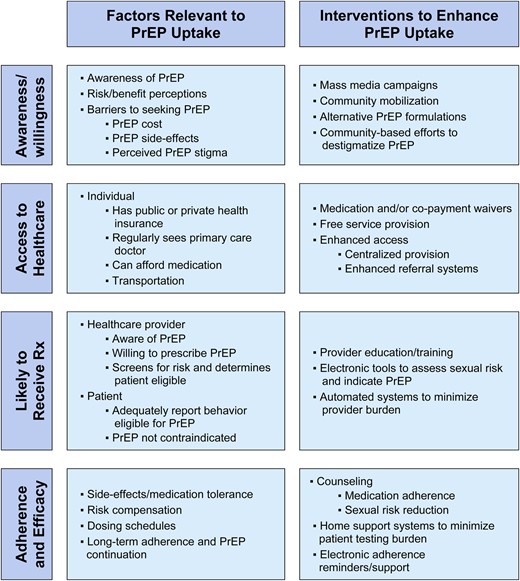
Theorectical model of the PrEP care continuum, factors relevant to uptake, and areas for intervention. Abbreviation: PrEP, pre-exposure prophylaxis.
AWARENESS OF AND WILLINGNESS TO TAKE PREP
Awareness of PrEP and subsequent willingness to initiate PrEP among those at highest risk for HIV infection is the necessary first step to PrEP uptake. Knowledge of PrEP among MSM has increased in the last 5 years, particularly since the release of PrEP efficacy trial results [16]. However, awareness of PrEP among MSM remains varied and limited, and PrEP messaging may not be reaching those at highest risk [16, 17]. A September 2014 Kaiser Family Foundation survey found less than half of gay and bisexual men were aware of PrEP, and only 5% had ever used PrEP [13]. Among MSM at highest risk of HIV infection, including black MSM, knowledge of PrEP may be lower or inconsistent [18].
Among MSM aware of PrEP, interest has been relatively high, and studies show most are in support of PrEP for HIV prevention, including black and young MSM [19]. Willingness of MSM to use PrEP is associated with cost of medication, stigma, concerns regarding disclosing PrEP use to partners, and perception of HIV risk [12, 17]. Additionally, studies among US MSM have shown concerns about daily pill taking, adverse effects, and whether PrEP provides sufficient protection from HIV infection [12, 20]. Barriers limiting willingness to use PrEP may be greater in the highest risk populations, including nonwhite and younger MSM [16, 20]. Increasing awareness, inculcating more positive norms surrounding use, and enhancing motivation to sustain adherence, could increase willingness to use PrEP.
ACCESS TO HEALTHCARE
Obtaining a prescription for PrEP requires healthcare provider access, in terms of both regular attendance and affordability of provider visits. The venues where PrEP is prescribed are widely varying: sexually transmitted infection (STI) clinics, HIV/AIDS community-based organizations, health maintenance organizations, research and PrEP demonstration studies, and clinician offices [21]. Additionally, a range of providers prescribes PrEP, including HIV specialists, advanced-practice practitioners, and primary care physicians. Monitoring services, associated physician visits and TDF/FTC prescription may result in significant out-of-pocket costs, in the form of co-pays and deductibles for those with health insurance. Costs of these services are likely unaffordable for those without health insurance. Although there is manufacturer assistance for obtaining TDF/FTC at reduced cost for those without insurance or who face high drug-copays, in most parts of the United States there is not a similar system to subsidize monitoring costs of laboratory testing and provider visits. The Affordable Care Act (ACA) has resulted in significant declines in the percentage of Americans without health insurance; from its peak at 18% in 2013, the uninsured rate has declined to 11.9% in Q1 2015 [22]. The ACA also expanded Medicaid coverage to 138% of the federal poverty level (FPL) for most low-income adults. However, more than 20 states have opted not to expand Medicaid programs, and many of these states, including Georgia, have high rates of HIV transmission [23]. As poverty is a significant risk factor for HIV, the lack of Medicaid expansion is likely to leave many who are at risk for HIV without access to biomedical prevention services [24].
LIKELY TO RECEIVE A PRESCRIPTION FOR PREP
Once a patient has reached an appropriate provider, he or she must be screened for behavioral eligibility and, if eligible, offered a PrEP prescription. Lack of disclosure of same-sex attraction is common, with 56% of MSM in one study not disclosing to their providers [25]. Provider willingness to prescribe PrEP may also be limited by concerns such as drug toxicity, medication adherence, cost, and risk compensation [26]. CDC guidance provides several options to screen for PrEP behavioral eligibility [10]. One method indicates as behaviorally eligible male patients with a male sex partner in the past 6 months, not in a monogamous relationship with a recently tested HIV-negative man, AND any anal sex without condoms (past 6 months), any STI (past 6 months), or in an ongoing relationship with an HIV-positive partner. Another method recommended by CDC is a Risk Index that assesses six domains and provides PrEP eligibility score. Although this index was developed based on datasets from national trials [27], we recently demonstrated its low predictive value for 2-year HIV seroconversion among MSM in Atlanta [6]. Algorithms that take into account local epidemiological profiles could enhance the ability to appropriately target PrEP prescriptions, although any such system would need to be in a format amenable to provider adoption.
ADHERENCE AND EFFICACY
Clinical efficacy of PrEP is dependent on adherence. In clinical trials of MSM, heterosexual men and women, and intravenous drug users, efficacy estimates for PrEP ranged from 44% to 84% [7, 28–30]. However, 2 trials of heterosexual women in Africa were stopped early due to lack of efficacy, and low levels of adherence to study product contributed greatly [31, 32]. Later evidence showed that efficacy of PrEP was greater than 90% when detectable blood levels of study product were present [33, 34]. Current recommendations are for daily dosing of TDF/FTC during periods of high-risk behavior, although results recently presented in abstract form (discussed below) could support intermittent dosing in the future [35, 36]. In addition, dose ranging studies and the open-label cohort study of MSM who previously participated in PrEP trials suggest that high levels of efficacy can be achieved with greater than 2 or 3 doses/week [8, 33].
The iPrEx study team conducted an open-label, cohort extension study of men and transgender women who were previously enrolled in PrEP clinical trials, which may represent the best available estimate of combined PrEP adherence and efficacy in real world settings for MSM [8]. In this study, adherence and efficacy resulted in a 51% decline in HIV incidence, relative to the placebo arm of the prior iPrEx trial. Higher levels of PrEP adherence were seen among those who reported condomless receptive anal intercourse, suggesting that those engaged in high-risk behavior may be more likely to adhere to PrEP. However, younger men did not adhere as well to PrEP as older men, so special consideration to adherence is critical in this group. Of note, the PROUD, a PrEP implementation study conducted in England, and IPERGAY, an intermittent PrEP study conducted in France and Canada, results were recently reported in abstract form. Both reported exceptionally high efficacy (>85%) in MSM who reported very high levels of sexual risk behavior suggesting high levels of adherence to the study regimen [36, 37]. Intermittent dosing schedules could improve PrEP adherence, however it remains to be seen whether these levels of efficacy can be achieved in US MSM.
PREP CONTINUUM APPLIED TO A COHORT OF MSM IN ATLANTA
By synthesizing data from the Emory-based InvolveMENt cohort and literature, we applied the proposed PrEP care continuum to illustrate the proportion of at-risk MSM in the Atlanta cohort who might theoretically have achieved protection from HIV infection with PrEP, given the sequential barriers outlined above. Descriptions of the characteristics and HIV/STI incidence in InvolveMENt have been published [5, 6, 38]. Briefly, between 2010 and 2012, MSM aged 18 years and above were recruited, regardless of HIV status, from the Atlanta community. Eligible participants self-identified as black and white MSM who reported sex with another man in the previous 3 months and who were not in a mutually monogamous relationship, could complete survey instruments in English, and lived in the Atlanta metropolitan area. Men who self-identified as Hispanic or of other/mixed race were not enrolled. All men were tested for HIV and completed a detailed computer-assisted self-interview questionnaire to evaluate demographic, individual, dyadic, and community-level HIV risk. Men who were HIV negative at baseline were prospectively followed for up to 24 months and underwent HIV testing at 3–6 month intervals. Thirty-two HIV seroconversions were observed, yielding estimated annual incidence rates of 3.8% overall, 6.5% among black MSM, and 1.7% among white MSM [6].
We projected the PrEP care continuum for the entire cohort, black MSM only, white MSM only, and seroconverters, by serial multiplication of estimates for each step. Based on study inclusion criteria, we included all HIV-negative MSM in the cohort in step 1 of the continuum: at-risk MSM. We estimated step 2, awareness of and willingness to take PrEP, at 50% based on data from our cohort, where approximately half of MSM reported awareness/willingness, and the literature, where estimates ranged from 17% to 94% [13, 16, 17, 20]. It is important to note that estimates of awareness and willingness to take PrEP for MSM are rapidly changing and current, accurate estimates in any given subpopulation and/or geographic location are difficult to determine. Therefore, we chose to use 50% for awareness/willingness, as an optimistic assessment for demonstrative purposes. Step 3, access to healthcare, was conceptualized as insurance access, and estimated based on InvolveMENt survey responses (Figure 2). We included all men who reported having health insurance (eg, private insurance, Medicare, Medicaid, etc.) and men who reported earning >138% of the FPL as they would be eligible to purchase health insurance on ACA insurance exchanges. The state of Georgia has not expanded Medicaid; therefore, men earning less than 138% of FPL without current health insurance are not expected to have insurance access. Step 4, likely to receive a PrEP prescription, was determined based on InvolveMENt survey responses. Per CDC guidelines, all men that reported sex without condoms (last 6 months), or an STI diagnosis (last 6 months), or an HIV-positive partner on the baseline InvolveMENt survey were categorized as likely to receive a prescription. Finally, we used the iPrEx open label extension adherence/efficacy estimate of 51% (95% confidence interval [CI]: 23%–69%) for step 5 [8]. These continuum-step-wise estimates were multiplied to yield the cumulative proportion achieving each step and, ultimately, theoretical PrEP protection. Because the proportion achieving theoretical PrEP protection was derived from multiple samples, to estimate its 95% CI, we combined the standard errors for each individual step's proportions, using Monte Carlo simulations of independent normal distributions. As an optimistic, best-case scenario for the impact of future interventions to improve the PrEP care continuum, we considered the effects of absolute 20% increases at all steps on cumulative HIV protection, to a maximum of 100% for any single step.
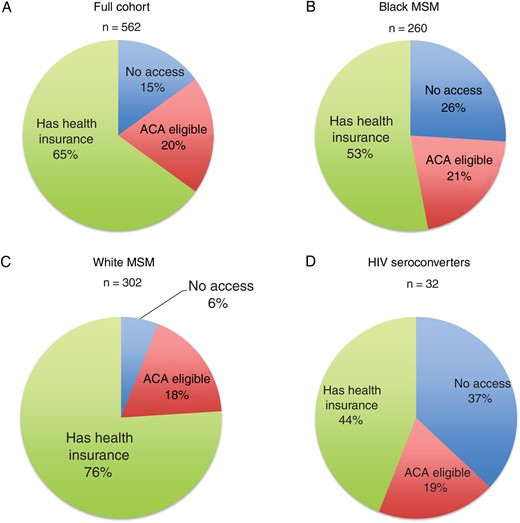
Distribution of health insurance status and Affordable Care Act (ACA) eligibility for (A) the total InvolveMENt cohort, (B) black MSM, (C) white MSM, and d) HIV seroconverters in the InvolveMENt cohort. *P < .001 for difference between white MSM, black MSM, and HIV serocoveters by chi-square test. Abbreviations: HIV, human immunodeficiency virus; MSM, men who have sex with men.
Figure 3 presents the estimated PrEP care continuum for the entire cohort (n = 562), stratified by race (n = 302 white MSM; n = 260 black MSM), and for HIV seroconverters (n = 32). Per Figure 3A, 86.1% of all MSM were estimated to have healthcare access, and 69.1% were likely to receive a prescription. Combined with awareness/willingness and efficacy estimates, PrEP protection would be achieved by 15.2% (95% CI, 6.7%, 23.8%) of the total cohort. Per Figure 3B and 3C, black MSM were estimated as less likely than white MSM to have access to healthcare and to receive a prescription, resulting in 12.3% (95% CI, 5.5%, 19.7%) of black and 17.8% (95% CI, 7.9%, 28.2%) of white MSM projected to achieve theoretical protection with PrEP. Among the 32 HIV seroconverters, the likelihood to receive a prescription was slightly higher than the full cohort at 75.0%, yet projected PrEP protection was 12.3% (95% CI, 4.7%, 22.9%) (Figure 3D). Interventions of 20% increases in all continuum steps yielded protection from HIV with PrEP of 44.3% for the whole cohort, 39.9% for black MSM, 46.6% for white MSM, and 39.9% for seroconverters.
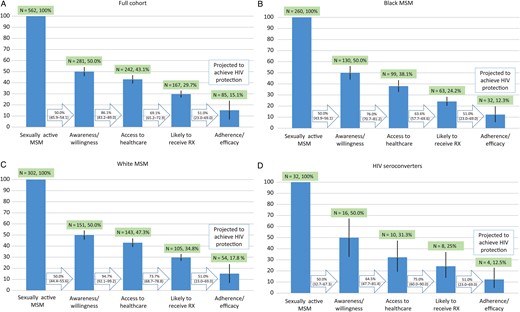
The PrEP care continuum for (A) the total InvolveMENt cohort, (B) black MSM (C) white MSM and (D) HIV seroconverters in the InvolveMENt cohort. Abbreviations: HIV, human immunodeficiency virus; MSM, men who have sex with men; PrEP, pre-exposure prophylaxis.
LIMITATIONS
The proposed PrEP care continuum has several limitations. The continuum begins with defining an at-risk population, which is inherently difficult given numerous possible understandings of what constitutes risk and the hidden nature of the population. Participants in our cohort also had access to frequent HIV testing, which can serve to facilitate PrEP education and access, or as a barrier where these services are not available. The continuum imposes a specific sequence for achieving protection from HIV with PrEP that may not be true for all individuals. In addition, each step of the continuum was parameterized with a single, necessary aspect (eg, health insurance) when multiple competing aspects (eg, healthcare seeking behavior, transportation, comfort with healthcare provider) likely contribute. These multiple, competing aspects to each step are likely to be greater for MSM with comorbid conditions such as substance abuse or mental illness and other challenges such as unstable housing and will contribute substantially to the likelihood to achieve protection from HIV with PrEP. Finally, our projections are limited to black and white MSM, and it is unclear how results might differ for other at-risk populations (eg, Latino MSM or women) or demographic groups (eg, adolescents).
CONCLUSION
We have illustrated that even with generous, optimistic estimates, few Atlanta MSM will achieve protection from HIV with PrEP given significant barriers currently in place. With substantial 20% increases at all steps, the potential for increasing overall coverage was improved to 44%, which has been projected to avert nearly 25% of new infections over 10 years [11]. Given the current state of the PrEP care continuum, large, sustained changes are needed to achieve levels of HIV protection that might alter the course of the epidemic. It is also notable that black MSM are less likely to have access to healthcare, to screen as eligible for a PrEP prescription, and to ultimately be protected by PrEP, despite facing HIV incidence rates nearly triple that of white MSM in Atlanta [6]. Therefore, disparities in achieving HIV protection with PrEP, although not statistically significant in our theoretic projections, have the potential to worsen racial disparities in HIV unless concerted effort is taken to enhance access for those most at-risk.
Each step of the proposed continuum represents a critical intervention point that demands immediate attention, particularly in geographic areas that have a large burden of HIV and have been slow to implement PrEP, such as Atlanta. The likelihood to seek PrEP could be fundamentally changed through mass national awareness campaigns. Access to PrEP could entirely shift with changes in policy to make PrEP free for those who are uninsured. The likelihood of appropriately receiving a PrEP prescription could change based on concerted provider training efforts and development of custom algorithms tailored to local epidemics. Last, adherence and efficacy may shift given development and scale-up of new adherence technology, or shifts in PrEP formulations such as a long-acting, injectable PrEP [39].
However, given the immediate need for intervention in high incidence settings such as among Atlanta MSM, novel strategies for PrEP delivery that circumvent the barriers presented in the PrEP care continuum are needed to achieve the necessary effectiveness for MSM most at risk of HIV. In our opinion, this should include free or low-cost open access PrEP programs targeted to those at highest risk. An important first step would be ensuring that PrEP is freely available where at-risk MSM are currently accessing services including STI screening and treatment centers, HIV testing services, and/or other HIV prevention services.
Notes
Financial support. This work was supported by the National Institutes of Health: KL2TR000455 (to C. F. K.), K23AI108335 (to C. F. K.), R01MH085600 (to P. S. S.), The Atlanta Clinical and Translational Science Institute UL1TR000454, and the Emory Center for AIDS Research P30 AI050409.
Potential conflicts of interest. All authors: No potential conflicts of interest.
All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.


{kind=link}
{kind=link}
{kind=link}