





In September 2020, an 87-year-old Japanese man presented with a 5-day history of high fever and generalized rash. He had been receiving carbamazepine for trigeminal neuralgia. He had engaged in forestry for some time. His body temperature was 40.3°C, while other vital signs were normal. Physical examination revealed a non-pruritic maculopapular rash on his trunk and extremities, including his palms and soles. No eschar was detected. Laboratory data showed a low platelet count (8.3 × 104/μL), elevated aspartate aminotransferase (91 U/L), lactate dehydrogenase (426 U/L) and C-reactive protein (26.8 mg/dL). Serological tests revealed no elevation of anti-Orientia tsutsugamushi IgM. Carbamazepine was discontinued due to suspected drug hypersensitivity syndrome, but the fever persisted.
Three days later, a 78-year-old Japanese woman, the above patient’s wife, presented with a 4-day history of fever and skin rash. Her body temperature was 39.5°C, while other vital signs were normal. Physical examination further revealed a non-pruritic maculopapular rash on her trunk and extremities, including her palms and soles (Figure 1a). An eschar was located on her right earlobe, which indicated the site of an infected chigger bite (Figure 1b). Laboratory data showed a low platelet count (7.7 × 104/μL), elevated aspartate aminotransferase (77 U/L), lactate dehydrogenase (303 U/L) and C-reactive protein (6.0 mg/dL). There was also no elevation of anti-Orientia tsutsugamushi IgM, but increased antibody titer for Rickettsia japonica was observed in paired sera using an indirect fluorescent antibody. Family cluster of Japanese spotted fever was diagnosed. After treatment with minocycline (200 mg/day for 14 days), the patients’ symptoms resolved completely.
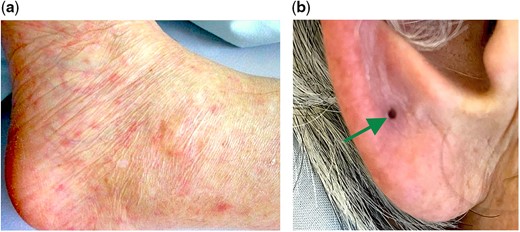
(a) Non-pruritic maculopapular rash on her left sole. (b) An eschar was located on her right earlobe, which indicated the site of an infected chigger bite (arrow).
Japanese spotted fever, a tick-borne disease caused by R. japonica, is an endemic disease in Japan.1,2 The common presentation involves fever (99%), skin rash (94%) and eschar (66%).1 In our case, the male patient had no evidence of eschar. Although eschar is one of the key clinical symptoms in the diagnosis of Japanese spotted fever, it may disappear in a few days.3 The main laboratory findings include thrombocytopenia, elevated C-reactive protein and elevated liver enzymes.4 The diagnosis is confirmed when there is a 4-fold or greater increase in IgG in the paired sera of the acute and convalescent phases or positive polymerase chain reactions for R. japonica. The risk of infection is associated with forestry, agricultural activities and leisure.2 The female patient had no history of risky exposure to Japanese spotted fever. Rickettsiosis, including Japanese spotted fever, is considered as a sporadic disease; however, family clusters and geographical hyperendemicity have been reported.5
Authorship: All authors had access to the data and a role in writing the manuscript.
Conflict of interest. None declared.

{kind=link}