





Abstract
Neonate hyperbilirubinemia usually resolves within 3–5 days without complications however, severe neonatal jaundice (SNJ) is associated with long-term neurocognitive impairment, cerebral palsy, auditory neuropathy, deafness, or death. Globally, at least 481,000 term/near-term neonates are affected by SNJ annually, with 114,000 neonates dying and an additional 63,000 neonates surviving with kernicterus [1,2]. Phototherapy and exchange transfusions prevent/treat SNJ, but these modalities are scarce in some low and lower-middle income countries, where SNJ prevalence is increased due to higher prevalence of glucose-6-phosphate dehydrogenase deficiency, blood group incompatibilities, late referrals, and delayed diagnosis. We aimed to explore a model for allo-hemodialysis (alloHD), a novel potential modality to treat SNJ rapidly and effectively in neonates, possibly avoiding exchange transfusions.
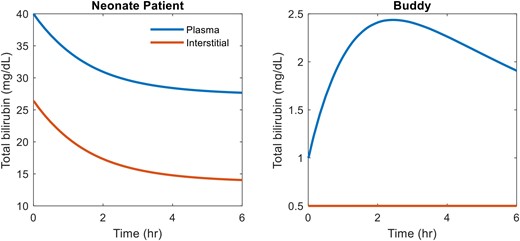
With alloHD, the neonate's blood flows through hollow fibers of a 0.075 m2 miniature low flux hemodialyzer (pore size 1.2 to 2.2 nm), while the blood of a healthy adult (“buddy”) flows counter-currently through the dialyzer, thus serving as the “dialysate”. Our mathematical model simulates the bilirubin kinetics in alloHD, with neonate and buddy blood flow rates at 15 and 30 mL/min, respectively. In the neonate model, bilirubin conjugation was assumed to be zero, resulting in excess unconjugated bilirubin that binds to albumin and causes SNJ. Bilirubin production rate in neonate and buddy were set to 6 and 3 mg/kg/day, respectively [3]. Buddy bilirubin conjugation rate was calculated to obtain normal steady state bilirubin levels. We only simulated unconjugated bilirubin because the conjugated form is easily excreted. Simulations are performed with neonate and buddy albumin levels of 31 g/L and 43 g/L, respectively.
Model simulations suggest that 3- to 6-hour alloHD session can reduce neonatal bilirubin levels by >30% (Fig. 1, left panel). Due to the high bilirubin conjugation capacity of an adult's healthy liver, the buddy's bilirubin level increases only transiently during the alloHD session (Fig. 1, right panel).
Our modeling suggests that a single alloHD session can lower neonatal bilirubin levels effectively. In principle, this bilirubin reduction should lower the risks associated with SNJ, especially kernicterus and possibly avoiding exchange transfusions. Future modeling scenarios will incorporate the improved neonatal liver function over time and additional alloHD schedules.


{kind=link}
Comments