





Abstract
Thrombotic microangiopathy (TMA) are a heterogeneous group of diseases characterized by mechanical hemolytic anemia, peripheral thrombocytopenia, and organ failure of variable severity. In patients with cancer, TMAs are frequently induced by antineoplastic drugs but may be related to the malignant disease itself. Small series have reported poor prognosis. Only chemotherapy succeeded in lengthening life expectancy, even if few reports have described efficacy of therapeutic plasma exchange (TPE) or Eculizumab. Complement regulation was not studied in these publications, as the pathophysiology was rarely explored. In this study, we investigated retrospectively 59 cases of cancer-associated TMAs, to describe characteristics at diagnosis and efficacy of treatment.
We conducted a retrospective multicentric observational study including all patients with a diagnosis of cancer-associated TMA, hospitalized in nephrological intensive care units (members of the French Intensive Care Network), between 2008 and 2019. We excluded patients receiving chemotherapy known to cause TMAs. We analyzed clinical and biological characteristics at diagnosis. We reported complement analysis when available. We defined four distinct treatment groups: No treatment (N), Plasmapheresis (P), Chemotherapy with or without chemotherapy (C+P), Eculizumab with or without Chemotherapy or Plasmapheresis (E+C+P). Renal remission and global survival were compared according to treatment group.
We included 59 patients admitted to intensive care units for cancer-associated TMA. Twenty patients had a past history of cancer. Fifty percent was female, and mean age was 62.8 years. The primary cancer was breast (23.7%), lung (18.6%), stomach (10.2%), and prostate (10.2%). Adenocarcinoma was the most frequent histologic subtype (47.5%). The cancer was metastatic in almost cases (89.8%). At presentation, TMA manifestations were pulmonary (57.6%), neurologic (49.2%), bone pain (30.5%), and disseminated intravascular coagulopathy (DIVC) (55.9%). Forty-one patients had a bone marrow aspiration and/or biopsy. Among them, medullar metastases were found in 20 patients (48.7%). We observed low C3 in 14.7% of cases suggesting an activation of the alternative pathway. No genetic analysis was performed. Only one patient had an undetectable ADAMTS13 <5% without inhibitory ADAMTS13 antibodies. Renal failure was seen in 28 patients whom 63.7% had severe grade 3 acute kidney injury. Renal biopsy was performed in 6 patients with severe arteriolar TMA lesions. Seventeen patients had no treatment (N), fifteen patients were treated with TPE (P), twenty patients received chemotherapy with TPE (C+P), and seven patients received Eculizumab with TPE (E). Hematological and renal remission was not significantly different between treatment groups (p=0.74 and p=0.10 respectively). Mortality was high, 52.5% at one month, 90% after one year of follow-up. The median duration of survival was 27 days [8.5;95.5] in patients who received treatment. Survival was improved in (C+P) and (E+C+P) groups, significantly (p<0.0001).
We report the largest series of cancer-associated TMAS since the advent of Eculizumab for the treatment of HUS. Typical presentation included old age, bone pain, dyspnea, and DIVC. These symptoms, when associated with TMA, should therefore suggest a diagnosis of cancer. Bone marrow aspiration or biopsy led to diagnosis of cancer in half of cases, and should be systematically performed to rapidly confirm diagnosis. The overall prognosis remained dramatically poor, with a mortality rate of 90% in the first year. Chemotherapy is probably the most efficient therapy to delay the death. C3 serum level was decreased in only 7 patients, suggesting that the pathophysiology of cancer-associated TMA is not linked to complement activation. As a result, neither TPE nor Eculizumab improved survival rate.

Comparison of survival probability according to treatment
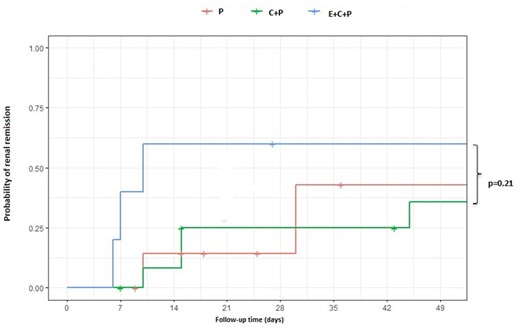
Comparison of renal remission according to treatment


{kind=link}
Comments