





Abstract
Chronic kidney disease (CKD) accelerates both atherosclerosis and arterial calcification. The aim of the present study was to explore whether maximal carotid plaque thickness (cPT max) was increased in patients with CKD stage 3 compared to controls and associated with cardiovascular disease and severity of calcification in the carotid and coronary arteries.
The study group consisted of 200 patients with CKD stage 3 from the Copenhagen CKD Cohort and 121 age- and sex-matched controls. cPT max was assessed by ultrasound and arterial calcification by computed tomography scanning.
Carotid plaques were present in 58% of patients (n=115) compared with 40% of controls (n=48), P=0.002. Among participants with plaques, cPT max (median, interquartile range) was significantly higher in patients compared with controls (1.9 (1.4-2.3) versus 1.5 (1.2-1.8) mm, P=0.001. Cardiovascular disease was present in 9.4% of patients without plaques (n=85), 23.2% of patients with cPT max 1.0-1.9 mm (n=69) and 34.8% of patients with cPT max >1.9 mm (n=46), P=0.001.
Carotid and coronary calcium scores >400 were present in 0.0% and 4.0%, respectively, of patients with no carotid plaques, in 19.1% and 24.2% of patients with cPT max 1.0-1.9 mm, and in 47.5% and 52.6% of patients with cPT max >1.9 mm, P<0.001.
This is the first study showing that cPT max is increased in patients with CKD stage 3 compared to controls and closely associated with prevalent cardiovascular disease and severity of calcification in both the carotid and coronary arteries.
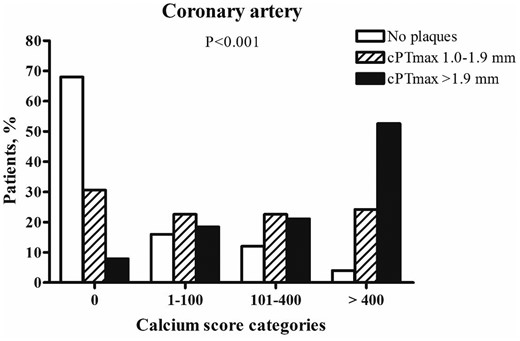
Association between maximal carotid plaque thickness (cPT max) and coronary artery calcium score.
According to carotid ultrasound findings, patients were divided into 3 groups: No carotid plaques, cPT max 1.0-1.9 mm, cPT max >1.9 mm. Based on the distribution of calcium scores from noncontrast CT scanning of the coronary arteries, patients were divided into calcium score categories of 0, 1-100, 101-400 and >400.


{kind=link}
Comments