





Abstract
We report the case of a 29-year-old male in whom COVID-19 concerns led to a delayed diagnosis of falciparum malaria. The patient developed symptoms of cerebral malaria with cytotoxic lesions of the corpus callosum in magnetic resonance imaging.
Case Report
A 29-year-old man was admitted to our ward due to muscle weakness, fatigue, nausea, vomiting and recurrent febrile episodes. The patient arrived from Zanzibar 3 weeks earlier, where he visited his family. He did not seek pre-travel advice or took any malaria prophylaxis. His symptoms started 2 weeks after arrival in Vienna, but he remained at home for another week as he was afraid of the ongoing coronavirus pandemic. The patient was born in Zanzibar but has stayed in Austria for the last 10 years.
Clinical examination at admission revealed diffuse abdominal pain, scleral icterus as well as a subtle impairment of consciousness. A dark discoloration of the urine was noticeable. Laboratory analysis demonstrated thrombocytopenia (31 G/l; normal range, 150–350 G/l), anaemia (haemoglobin, 9.9 g/dl; normal range, 13.5–18 g/dl), acute kidney injury (creatinine, 1.5 mg/dl; normal range, 0.70–1.20 mg/dl), elevated bilirubin (4.2 mg/dl; normal range < 1.2 mg/dl), lactate dehydrogenase (892 U/l, normal range < 250 U/l) and elevated C-reactive protein (16.1 mg/dl; normal range < 0.5 mg/dl). Thick and thin blood smears revealed Plasmodium falciparum infection with high parasitemia (Figure 1). Intravenous treatment with artesunate 240 mg (b.i.d.) and clindamycin 900 mg (b.i.d.) was initiated. Shortly after admission, the patient became hypotensive (blood pressure, 80/50 mmHg) and consciousness continued to deteriorate. He was transferred to an intensive care unit (ICU). Neurological examination showed a bulbar dysarthria and sixth nerve palsy. Magnetic resonance imaging (MRI) demonstrated a well-defined FLAIR- and T2-hyperintense, non-enhancing lesion in the splenium of the corpus callosum (CLOCC). The lesion showed restricted diffusion, which is consistent with the cytotoxic lesion of the CLOCC (Figure 2a–c). Under treatment, the clinical condition and neurological symptoms of the patient improved quickly and he was discharged from the ICU 2 days later. Artesunate treatment was continued for a total of 3 days, clindamycin was ended after 7 days. On follow-up MRI, performed 25 days after discharge, a complete resolution of the CLOCC was noted (Figure 2d–f).
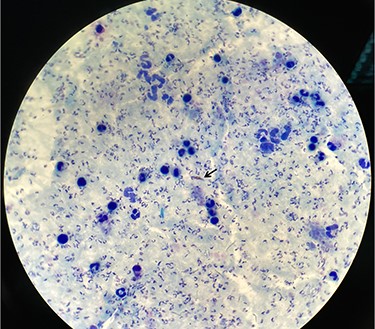
Thick blood smear demonstrates P. falciparum infection with high parasitemia; the black arrow shows a gametocyte of P. falciparum
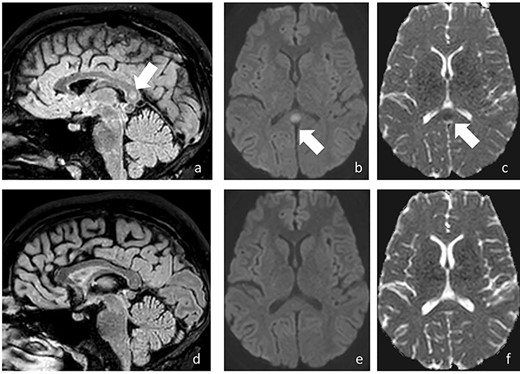
On sagittal FLAIR (a) a well-defined hyperintense lesion is detected in the splenium of the CLOCC; diffusion-weighted MR images (DWI) shows high signal on DWI (b) with corresponding low ADC (c), indicating diffusion restriction (arrow); the abnormality was consistent with cytotoxic lesion of the CLOCC; follow-up MRI 3 weeks later shows complete resolution of the abnormality (d–f)
Discussion
Today, around 5500 cases of malaria are imported to EU countries per year of which 10% progress to severe malaria.1 Zanzibar reported 5146 cases of malaria in 2018.2 Hence, malaria prophylaxis is recommended for travellers to Zanzibar. The reported patient did not seek pre-travel advice or took malaria prophylaxis, which is a frequently reported problem in travellers visiting friend and relatives (VFR).3 An increase of severe malaria cases associated with a delay of diagnosis and treatment during the COVID-19 pandemic was recently reported at France.4 The increased time between the onset of symptoms and malaria diagnosis in our patient was clearly attributable to his concerns about COVID-19, resulting in progression to cerebral malaria with development of CLOCC in MRI imaging.
CLOCC are secondary lesions reported in a wide range of cerebral infections.5 In a series of children with cerebral malaria from Malawi, CLOCC was the second most common finding of white matter diffusion restriction in MRI, however, similar lesions were also shown to be present in uncomplicated cases of imported malaria.6 Thus, whether CLOCC clearly represents cerebral involvement or even precedes clinical deterioration in malaria remains to be elucidated. In all, this case demonstrates that access and provision of pre-travel health care for travellers VFR still has to be improved and that the awareness of classic tropical diseases remains essential in times of a pandemic.7
Authors’ statement
Authors’ contributions
K.M., S.T. and SW were responsible for patient care; L.S. and S.W. wrote the manuscript; M.M.T. was responsible for the preparation of MRI images and all authors have seen and approved the manuscript.
Funding
This case report did not receive any specific grant from funding agencies in the public, commercial or not-for-profit sectors.
Conflict of Interest: None declared.
References
Starkey J, Konayashi N, Numaguchi, Y, Moritani T.

{kind=link}
{kind=link}