





Abstract
We sought to systematically review the effect of gender-affirming hormone therapy on psychological outcomes among transgender people. We searched PubMed, Embase, and PsycINFO through June 10, 2020 for studies evaluating quality of life (QOL), depression, anxiety, and death by suicide in the context of gender-affirming hormone therapy among transgender people of any age. We excluded case studies and studies reporting on less than 3 months of follow-up. We included 20 studies reported in 22 publications. Fifteen were trials or prospective cohorts, one was a retrospective cohort, and 4 were cross-sectional. Seven assessed QOL, 12 assessed depression, 8 assessed anxiety, and 1 assessed death by suicide. Three studies included trans-feminine people only; 7 included trans-masculine people only, and 10 included both. Three studies focused on adolescents. Hormone therapy was associated with increased QOL, decreased depression, and decreased anxiety. Associations were similar across gender identity and age. Certainty in this conclusion is limited by high risk of bias in study designs, small sample sizes, and confounding with other interventions. We could not draw any conclusions about death by suicide. Future studies should investigate the psychological benefits of hormone therapy among larger and more diverse groups of transgender people using study designs that more effectively isolate the effects of hormone treatment.
Transgender people are those whose gender identity is different from the sex they were assigned at birth. Estimates of the size of the transgender population vary depending on how the data are collected [1]. In studies that rely on clinical records, estimates range between 1 and 30 people per 100 000 (0.001% to 0.03%) [2]. Studies that focus instead on self-report among nonclinical populations find estimates that range between 0.1% and 2% [2].
Many transgender people seek medical services to affirm their gender identity. According to the Standards of Care for Transsexual, Transgender, and Gender Non-Conforming People maintained by the World Professional Association for Transgender Health (WPATH), gender-affirming medical care is different for each individual and may include a variety of services and procedures, such as psychological support, hormone therapy, and surgeries [3]. Hormone therapy, which typically involves estrogens and anti-androgens for transgender women and other trans-feminine people and testosterone for transgender men and other trans-masculine people, is a common component of medical gender affirmation [4]. Because hormone treatment can have a powerful effect on physical appearance, it is often a priority for transgender people seeking medical gender affirmation [5]. Gender-affirming hormone therapy can be managed for most patients by primary care providers, as it typically involves long-term maintenance on doses similar to those used for cisgender patients with conditions such as hypogonadism [6, 7]. Some clinicians require a minimum period of psychological counseling before hormone therapy can be initiated, while others provide hormone therapy on the basis of informed consent [8].
The need for gender-affirming care is often characterized using psychiatric diagnoses such as gender dysphoria, which replaced gender identity disorder in the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) [9]. The 11th International Classification of Diseases (ICD-11) replaces these terms with a diagnosis called gender incongruence (codes: HA60, HA61, HA6Z), which is located in a new chapter on sexual health. These changes clarify that the target of gender-affirming medical interventions is not the person’s gender identity itself but rather the clinically significant distress that can accompany a misalignment between gender identity and sex assigned at birth [10]. Some countries have further underscored that transgender identity is not a pathology by recognizing gender affirmation as fundamental to the human right to self-definition and removing requirements that transgender people seeking gender-affirming medical care present with a diagnosis such as gender dysphoria [11].
Several previous reviews have indicated that gender-affirming hormone therapy is associated with psychological benefits that include reductions in depression and anxiety and improvements in quality of life (QOL) among transgender people [12-17]. Most of these reviews did not require a minimum duration of hormone therapy [14-17]. One review that did impose a minimum follow-up requirement is 10 years old [12]. The other that required a minimum of 3 months of therapy included only uncontrolled prospective cohorts, which resulted in a sample of only 3 studies [13]. A comprehensive review without a minimum follow-up period assessed gender-affirming hormone therapy and surgeries only in adolescents [17]. By requiring a minimum duration of hormone treatment but considering all ages and a variety of study designs, we sought to update and more completely summarize the growing evidence base regarding the relationship between gender-affirming hormone therapy and psychological outcomes in transgender people.
Search Strategy and Selection Criteria
This review is one of a series of systematic reviews on gender-affirming care conducted for WPATH to inform the eighth revision of the Standards of Care. The protocol is registered on PROSPERO (CRD42018115379) [18], and we followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines in reporting our findings [19].
We searched PubMed, Embase, and PyscINFO from inception to October 2018 and updated the search through June 10, 2020, for studies assessing QOL, depression, anxiety, and death by suicide among transgender participants of any age in the context of gender-affirming hormone therapy [20]. We also reviewed the reference lists of previous reviews and hand-searched the International Journal of Transgenderism. Using DistillerSR [21], 2 reviewers independently screened titles, abstracts, and full-text articles. Differences were resolved through consensus adjudication.
We included studies that evaluated the psychological effects of any testosterone, estrogen, or anti-androgen formulation used for gender affirmation. We also considered gonadotropin-releasing hormone (GnRH) analogues used as anti-androgens or for puberty delay. Study participants must have been on hormone therapy for at least 3 months in order to reflect a minimum time for expected onset of effects [3]. Health care provider supervision was not required. We excluded studies that did not state therapy type and duration, including the range for cross-sectional studies. We included studies regardless of language (the search terms were in English) and country of origin, and we accepted any study design except case reports.
We created standardized forms for data extraction using the Systematic Review Data Repository system. The data extracted included participant demographics; study design and methods; hormone therapy type, dose, and duration; potential confounders such as gender-affirming surgery status; outcome scales [20]; and psychological outcomes. From studies that used the Short Form-36 Health Survey (SF-36) to measure QOL, we extracted scores in all domains [22]. For studies that used measures with depression or anxiety subscales, we extracted only the subscale scores corresponding to the psychological outcomes of interest (eg, the depression subscale of the Minnesota Multiphasic Personality Inventory [MMPI]). We extracted comparisons with cisgender controls or general population norms only when longitudinal findings in a transgender population or comparisons with an untreated transgender control group were not reported. We used WebPlotDigitizer to extract data reported only in figures [23].
Two reviewers independently assessed risk of bias [20]. For randomized controlled trials (RCTs), we used the revised Cochrane tool [24]. For non-randomized studies, we used the Cochrane Risk of Bias Assessment Tool for Non-Randomized Studies of Interventions (ROBINS-I) [25]. One reviewer graded strength of evidence for each outcome using the Agency for Healthcare Research and Quality Methods Guide for Conducting Comparative Effectiveness Reviews [26]. We considered the directionality and magnitude of effects reported in cross-sectional studies as additional context for our evaluation of evidence from trials and prospective and retrospective cohorts. Each strength of evidence assessment was confirmed by a second reviewer.
WPATH provided the research question and reviewed the protocol, evidence tables, and report. WPATH had no role in study design, data collection, analysis, interpretation, or drafting. The corresponding author had full access to all the data and had final responsibility for the decision to submit for publication. The authors are responsible for all content, and statements in this report do not necessarily reflect the official views of or imply endorsement by WPATH.
Results
We retrieved 1753 nonduplicate studies for the broader systematic review project of which this review was a part (Fig. 1). After screening and full-text review for the specific research question on the psychological effects of gender-affirming hormone therapy, 20 studies reported in 22 publications were included (Table 1): 1 RCT [27], 2 before-after trials [28, 29], 12 prospective cohorts reported in 13 publications [30-42], 1 retrospective cohort reported in 2 publications [43, 44], and 4 cross-sectional studies [45-48]. De Vries (2014) [35] reported on a subset of the participants in de Vries (2011) [34] who continued in care. We counted these publications as a single study but extracted and reported data separately because the characteristics of the study’s adolescent population changed substantially in the period between the 2 publications. Similarly, Asscheman (2011) [44] reported on an extension of Asscheman (1989) [43]; we counted these as a single study but extracted data separately. In Table 1 and in the subsequent tables for each outcome, studies are ordered first by study design (RCTs, before-after trials, prospective cohorts, retrospective cohorts, and cross-sectional studies); within these categories, studies are presented in the following order according to how the study results were reported: adult transgender women only, adult transgender men only, adult transgender women and transgender men together, and transgender adolescents (no study reported separate results by gender identity for transgender youth). Where multiple studies shared the same study design and population, they are additionally ordered chronologically.
Studies Reporting Effects of Gender-Affirming Hormone Therapy on Psychological Outcomes Among Transgender People
| Author, year Location Study name | Study design | Start year | Transgender population | Overall N | Age in years | Baseline HT status | Outcomes | GAS status | Risk of bias |
|---|---|---|---|---|---|---|---|---|---|
| Pelusi, 2014 [27] Italy | Randomized controlled triala | NR | Men | 45 | Mean: 29.5 | No previous HT | QOL | No GAS before or during study | High |
| Gava, 2016 [28] Italy | Before-after trial | NR | Women | 40 | Mean: 3.2 (range, 19–55) | No previous HT | QOL, Depression | No GAS before or during study | Low |
| Gava, 2018 [29] Italy | Before-after triala | NR | Men | 50 | Mean: 30.1 (range, 21–42) | No previous HT | QOL | 72% (n = 36) had gonadectomy during study | Serious |
| Fuss, 2015 [37] Belgium ENIGI (NCT01072825) | Prospective cohort | 2010 | Women | 20 | Mean: 33.9 (range, 17–48) | No previous HT | Anxiety | NR | Serious |
| Costantino, 2013 [32] Italy | Prospective cohort | 2001 | Men | 50 | Mean: 29.8 | No previous HT | Depression | No GAS before or during study | Serious |
| Motta, 2018 [41] Italy | Prospective cohort | 2013 | Men | 52 | Mean: 28.3 | No previous HT | Anxiety | NR | Moderate |
| Turan, 2018 [42] Turkey | Prospective cohortb | NR | Men | 37 | Mean: 24.6 | No previous HT | Depression, Anxiety | No GAS before or during study | Moderate |
| Metzger, 2019 [40] Switzerland, Germany | Prospective cohortb | 2013 | Men | 23 | Mean: 27.2 (range, 18–51) | No previous HT | Depression | No GAS before or during study | Moderate |
| Colizzi, 2014 [31] Italy | Prospective cohort | 2008 | Women and men | 107 | Mean: 29.2 | No previous HT | Depression, Anxiety | No GAS before or during study | Low |
| Manieri, 2014 [39] Italy | Prospective cohort | NR | Women and men | 83 | Mean: 32.7 (women), 30.2 (men) | No previous HT | QOL | No GAS before or during study | Moderate |
| Fisher, 2016 [36] Italy | Prospective cohort | 2012 | Women and men | 54 | Mean: 32.5 (women), 26.3 (men) | No previous HT | Depression | No GAS before or during study | Low |
| Defreyne, 2018 [33] UK | Prospective cohort | 2012 | Women and men | 155 | Median: 27 (range, 18–52) | No previous HT | Depression, Anxiety | Some had GAS during study; % and type NR | Serious |
| Asscheman, 1989 [43] Netherlands | Retrospective cohortb,d | 1972 | Women and men | 425 | Median: 32 (women, range, 16–67); 25.4 (men, range, 16–54) | Previous HT for at least 6 months | Death by suicide | 78% (n = 235) of transgender women had GAS during study; data NR for transgender men | Serious |
| Asscheman, 2011 [44] Netherlands | Retrospective cohortb,d | 1975 | Women and men | 1331 | Mean: 31.4 (women, range, 16–76); 26.1 (men, range, 16–57) | Previous HT for at least 1 year | Death by suicide | 87% (n = 834) of transgender women and 94% (n = 343) of transgender men had GAS during study | Serious |
| Leavitt, 1980 [47] US | Cross-sectional | 1976 | Women | 41 | Range, 18–35 | 54% (n = 22) on HT | Depression | No previous GAS | Serious |
| Wierckx, 2011 [48] Belgium | Cross-sectionalb | 2009 | Men | 47 | Mean: 37 (range, 22–54) | 100% on HT | QOL | 100% had GAS, but not within previous year | Serious |
| Gómez-Gil, 2012 [45] Spain | Cross-sectional | NR | Women and men | 187 | Mean: 29.9 (range, 15–61) | 64% (n = 120) on HT | Depression, Anxiety | 42% (n = 79) of all participants and 64% (n = 77) of participants on HT had previous GAS | Serious |
| Gorin-Lazard, 2012 [46] France | Cross-sectionalb | NR | Women and men | 61 | Mean: 34.7 | 72% (n = 44) on HT | QOL | No previous GAS | Serious |
| de Vries, 2011 [34] Netherlands | Prospective cohort | 2000 | Girls and boys | 70 | Mean: 14.8 (range, 11.3–18.6) | No previous HT | Depression, Anxiety | No GAS before or during study | Moderate |
| de Vries, 2014 [35] Netherlands | Prospective cohortb,c | 2000 | Girls and boys | 55 | Mean: 14.8 (range, 11.5–18.5) | No previous HT | Depression, Anxiety | 100% had GAS during study | Serious |
| Achille, 2020 [30] US | Prospective cohort | 2013 | Girls and boys | 50 | Mean: 16.2 | No previous HT | QOL, Depression | No GAS before or during study | Moderate |
| López de Lara, 2020 [38] Spain | Prospective cohortb | 2018 | Girls and boys | 23 | Mean: 16 (range, 14-18) | No previous HT | Depression, Anxiety | No GAS before or during study | Moderate |
| Author, year Location Study name | Study design | Start year | Transgender population | Overall N | Age in years | Baseline HT status | Outcomes | GAS status | Risk of bias |
|---|---|---|---|---|---|---|---|---|---|
| Pelusi, 2014 [27] Italy | Randomized controlled triala | NR | Men | 45 | Mean: 29.5 | No previous HT | QOL | No GAS before or during study | High |
| Gava, 2016 [28] Italy | Before-after trial | NR | Women | 40 | Mean: 3.2 (range, 19–55) | No previous HT | QOL, Depression | No GAS before or during study | Low |
| Gava, 2018 [29] Italy | Before-after triala | NR | Men | 50 | Mean: 30.1 (range, 21–42) | No previous HT | QOL | 72% (n = 36) had gonadectomy during study | Serious |
| Fuss, 2015 [37] Belgium ENIGI (NCT01072825) | Prospective cohort | 2010 | Women | 20 | Mean: 33.9 (range, 17–48) | No previous HT | Anxiety | NR | Serious |
| Costantino, 2013 [32] Italy | Prospective cohort | 2001 | Men | 50 | Mean: 29.8 | No previous HT | Depression | No GAS before or during study | Serious |
| Motta, 2018 [41] Italy | Prospective cohort | 2013 | Men | 52 | Mean: 28.3 | No previous HT | Anxiety | NR | Moderate |
| Turan, 2018 [42] Turkey | Prospective cohortb | NR | Men | 37 | Mean: 24.6 | No previous HT | Depression, Anxiety | No GAS before or during study | Moderate |
| Metzger, 2019 [40] Switzerland, Germany | Prospective cohortb | 2013 | Men | 23 | Mean: 27.2 (range, 18–51) | No previous HT | Depression | No GAS before or during study | Moderate |
| Colizzi, 2014 [31] Italy | Prospective cohort | 2008 | Women and men | 107 | Mean: 29.2 | No previous HT | Depression, Anxiety | No GAS before or during study | Low |
| Manieri, 2014 [39] Italy | Prospective cohort | NR | Women and men | 83 | Mean: 32.7 (women), 30.2 (men) | No previous HT | QOL | No GAS before or during study | Moderate |
| Fisher, 2016 [36] Italy | Prospective cohort | 2012 | Women and men | 54 | Mean: 32.5 (women), 26.3 (men) | No previous HT | Depression | No GAS before or during study | Low |
| Defreyne, 2018 [33] UK | Prospective cohort | 2012 | Women and men | 155 | Median: 27 (range, 18–52) | No previous HT | Depression, Anxiety | Some had GAS during study; % and type NR | Serious |
| Asscheman, 1989 [43] Netherlands | Retrospective cohortb,d | 1972 | Women and men | 425 | Median: 32 (women, range, 16–67); 25.4 (men, range, 16–54) | Previous HT for at least 6 months | Death by suicide | 78% (n = 235) of transgender women had GAS during study; data NR for transgender men | Serious |
| Asscheman, 2011 [44] Netherlands | Retrospective cohortb,d | 1975 | Women and men | 1331 | Mean: 31.4 (women, range, 16–76); 26.1 (men, range, 16–57) | Previous HT for at least 1 year | Death by suicide | 87% (n = 834) of transgender women and 94% (n = 343) of transgender men had GAS during study | Serious |
| Leavitt, 1980 [47] US | Cross-sectional | 1976 | Women | 41 | Range, 18–35 | 54% (n = 22) on HT | Depression | No previous GAS | Serious |
| Wierckx, 2011 [48] Belgium | Cross-sectionalb | 2009 | Men | 47 | Mean: 37 (range, 22–54) | 100% on HT | QOL | 100% had GAS, but not within previous year | Serious |
| Gómez-Gil, 2012 [45] Spain | Cross-sectional | NR | Women and men | 187 | Mean: 29.9 (range, 15–61) | 64% (n = 120) on HT | Depression, Anxiety | 42% (n = 79) of all participants and 64% (n = 77) of participants on HT had previous GAS | Serious |
| Gorin-Lazard, 2012 [46] France | Cross-sectionalb | NR | Women and men | 61 | Mean: 34.7 | 72% (n = 44) on HT | QOL | No previous GAS | Serious |
| de Vries, 2011 [34] Netherlands | Prospective cohort | 2000 | Girls and boys | 70 | Mean: 14.8 (range, 11.3–18.6) | No previous HT | Depression, Anxiety | No GAS before or during study | Moderate |
| de Vries, 2014 [35] Netherlands | Prospective cohortb,c | 2000 | Girls and boys | 55 | Mean: 14.8 (range, 11.5–18.5) | No previous HT | Depression, Anxiety | 100% had GAS during study | Serious |
| Achille, 2020 [30] US | Prospective cohort | 2013 | Girls and boys | 50 | Mean: 16.2 | No previous HT | QOL, Depression | No GAS before or during study | Moderate |
| López de Lara, 2020 [38] Spain | Prospective cohortb | 2018 | Girls and boys | 23 | Mean: 16 (range, 14-18) | No previous HT | Depression, Anxiety | No GAS before or during study | Moderate |
Abbreviations: ENIGI, European Network for the Investigation of Gender Incongruence; GAS, gender-affirming surgery; HT, hormone therapy; NR, not reported; QOL, quality of life.
bIncluded a cisgender control group or a comparison to general population norms
cAll participants were also included in de Vries (2011) [34]
Studies Reporting Effects of Gender-Affirming Hormone Therapy on Psychological Outcomes Among Transgender People
| Author, year Location Study name | Study design | Start year | Transgender population | Overall N | Age in years | Baseline HT status | Outcomes | GAS status | Risk of bias |
|---|---|---|---|---|---|---|---|---|---|
| Pelusi, 2014 [27] Italy | Randomized controlled triala | NR | Men | 45 | Mean: 29.5 | No previous HT | QOL | No GAS before or during study | High |
| Gava, 2016 [28] Italy | Before-after trial | NR | Women | 40 | Mean: 3.2 (range, 19–55) | No previous HT | QOL, Depression | No GAS before or during study | Low |
| Gava, 2018 [29] Italy | Before-after triala | NR | Men | 50 | Mean: 30.1 (range, 21–42) | No previous HT | QOL | 72% (n = 36) had gonadectomy during study | Serious |
| Fuss, 2015 [37] Belgium ENIGI (NCT01072825) | Prospective cohort | 2010 | Women | 20 | Mean: 33.9 (range, 17–48) | No previous HT | Anxiety | NR | Serious |
| Costantino, 2013 [32] Italy | Prospective cohort | 2001 | Men | 50 | Mean: 29.8 | No previous HT | Depression | No GAS before or during study | Serious |
| Motta, 2018 [41] Italy | Prospective cohort | 2013 | Men | 52 | Mean: 28.3 | No previous HT | Anxiety | NR | Moderate |
| Turan, 2018 [42] Turkey | Prospective cohortb | NR | Men | 37 | Mean: 24.6 | No previous HT | Depression, Anxiety | No GAS before or during study | Moderate |
| Metzger, 2019 [40] Switzerland, Germany | Prospective cohortb | 2013 | Men | 23 | Mean: 27.2 (range, 18–51) | No previous HT | Depression | No GAS before or during study | Moderate |
| Colizzi, 2014 [31] Italy | Prospective cohort | 2008 | Women and men | 107 | Mean: 29.2 | No previous HT | Depression, Anxiety | No GAS before or during study | Low |
| Manieri, 2014 [39] Italy | Prospective cohort | NR | Women and men | 83 | Mean: 32.7 (women), 30.2 (men) | No previous HT | QOL | No GAS before or during study | Moderate |
| Fisher, 2016 [36] Italy | Prospective cohort | 2012 | Women and men | 54 | Mean: 32.5 (women), 26.3 (men) | No previous HT | Depression | No GAS before or during study | Low |
| Defreyne, 2018 [33] UK | Prospective cohort | 2012 | Women and men | 155 | Median: 27 (range, 18–52) | No previous HT | Depression, Anxiety | Some had GAS during study; % and type NR | Serious |
| Asscheman, 1989 [43] Netherlands | Retrospective cohortb,d | 1972 | Women and men | 425 | Median: 32 (women, range, 16–67); 25.4 (men, range, 16–54) | Previous HT for at least 6 months | Death by suicide | 78% (n = 235) of transgender women had GAS during study; data NR for transgender men | Serious |
| Asscheman, 2011 [44] Netherlands | Retrospective cohortb,d | 1975 | Women and men | 1331 | Mean: 31.4 (women, range, 16–76); 26.1 (men, range, 16–57) | Previous HT for at least 1 year | Death by suicide | 87% (n = 834) of transgender women and 94% (n = 343) of transgender men had GAS during study | Serious |
| Leavitt, 1980 [47] US | Cross-sectional | 1976 | Women | 41 | Range, 18–35 | 54% (n = 22) on HT | Depression | No previous GAS | Serious |
| Wierckx, 2011 [48] Belgium | Cross-sectionalb | 2009 | Men | 47 | Mean: 37 (range, 22–54) | 100% on HT | QOL | 100% had GAS, but not within previous year | Serious |
| Gómez-Gil, 2012 [45] Spain | Cross-sectional | NR | Women and men | 187 | Mean: 29.9 (range, 15–61) | 64% (n = 120) on HT | Depression, Anxiety | 42% (n = 79) of all participants and 64% (n = 77) of participants on HT had previous GAS | Serious |
| Gorin-Lazard, 2012 [46] France | Cross-sectionalb | NR | Women and men | 61 | Mean: 34.7 | 72% (n = 44) on HT | QOL | No previous GAS | Serious |
| de Vries, 2011 [34] Netherlands | Prospective cohort | 2000 | Girls and boys | 70 | Mean: 14.8 (range, 11.3–18.6) | No previous HT | Depression, Anxiety | No GAS before or during study | Moderate |
| de Vries, 2014 [35] Netherlands | Prospective cohortb,c | 2000 | Girls and boys | 55 | Mean: 14.8 (range, 11.5–18.5) | No previous HT | Depression, Anxiety | 100% had GAS during study | Serious |
| Achille, 2020 [30] US | Prospective cohort | 2013 | Girls and boys | 50 | Mean: 16.2 | No previous HT | QOL, Depression | No GAS before or during study | Moderate |
| López de Lara, 2020 [38] Spain | Prospective cohortb | 2018 | Girls and boys | 23 | Mean: 16 (range, 14-18) | No previous HT | Depression, Anxiety | No GAS before or during study | Moderate |
| Author, year Location Study name | Study design | Start year | Transgender population | Overall N | Age in years | Baseline HT status | Outcomes | GAS status | Risk of bias |
|---|---|---|---|---|---|---|---|---|---|
| Pelusi, 2014 [27] Italy | Randomized controlled triala | NR | Men | 45 | Mean: 29.5 | No previous HT | QOL | No GAS before or during study | High |
| Gava, 2016 [28] Italy | Before-after trial | NR | Women | 40 | Mean: 3.2 (range, 19–55) | No previous HT | QOL, Depression | No GAS before or during study | Low |
| Gava, 2018 [29] Italy | Before-after triala | NR | Men | 50 | Mean: 30.1 (range, 21–42) | No previous HT | QOL | 72% (n = 36) had gonadectomy during study | Serious |
| Fuss, 2015 [37] Belgium ENIGI (NCT01072825) | Prospective cohort | 2010 | Women | 20 | Mean: 33.9 (range, 17–48) | No previous HT | Anxiety | NR | Serious |
| Costantino, 2013 [32] Italy | Prospective cohort | 2001 | Men | 50 | Mean: 29.8 | No previous HT | Depression | No GAS before or during study | Serious |
| Motta, 2018 [41] Italy | Prospective cohort | 2013 | Men | 52 | Mean: 28.3 | No previous HT | Anxiety | NR | Moderate |
| Turan, 2018 [42] Turkey | Prospective cohortb | NR | Men | 37 | Mean: 24.6 | No previous HT | Depression, Anxiety | No GAS before or during study | Moderate |
| Metzger, 2019 [40] Switzerland, Germany | Prospective cohortb | 2013 | Men | 23 | Mean: 27.2 (range, 18–51) | No previous HT | Depression | No GAS before or during study | Moderate |
| Colizzi, 2014 [31] Italy | Prospective cohort | 2008 | Women and men | 107 | Mean: 29.2 | No previous HT | Depression, Anxiety | No GAS before or during study | Low |
| Manieri, 2014 [39] Italy | Prospective cohort | NR | Women and men | 83 | Mean: 32.7 (women), 30.2 (men) | No previous HT | QOL | No GAS before or during study | Moderate |
| Fisher, 2016 [36] Italy | Prospective cohort | 2012 | Women and men | 54 | Mean: 32.5 (women), 26.3 (men) | No previous HT | Depression | No GAS before or during study | Low |
| Defreyne, 2018 [33] UK | Prospective cohort | 2012 | Women and men | 155 | Median: 27 (range, 18–52) | No previous HT | Depression, Anxiety | Some had GAS during study; % and type NR | Serious |
| Asscheman, 1989 [43] Netherlands | Retrospective cohortb,d | 1972 | Women and men | 425 | Median: 32 (women, range, 16–67); 25.4 (men, range, 16–54) | Previous HT for at least 6 months | Death by suicide | 78% (n = 235) of transgender women had GAS during study; data NR for transgender men | Serious |
| Asscheman, 2011 [44] Netherlands | Retrospective cohortb,d | 1975 | Women and men | 1331 | Mean: 31.4 (women, range, 16–76); 26.1 (men, range, 16–57) | Previous HT for at least 1 year | Death by suicide | 87% (n = 834) of transgender women and 94% (n = 343) of transgender men had GAS during study | Serious |
| Leavitt, 1980 [47] US | Cross-sectional | 1976 | Women | 41 | Range, 18–35 | 54% (n = 22) on HT | Depression | No previous GAS | Serious |
| Wierckx, 2011 [48] Belgium | Cross-sectionalb | 2009 | Men | 47 | Mean: 37 (range, 22–54) | 100% on HT | QOL | 100% had GAS, but not within previous year | Serious |
| Gómez-Gil, 2012 [45] Spain | Cross-sectional | NR | Women and men | 187 | Mean: 29.9 (range, 15–61) | 64% (n = 120) on HT | Depression, Anxiety | 42% (n = 79) of all participants and 64% (n = 77) of participants on HT had previous GAS | Serious |
| Gorin-Lazard, 2012 [46] France | Cross-sectionalb | NR | Women and men | 61 | Mean: 34.7 | 72% (n = 44) on HT | QOL | No previous GAS | Serious |
| de Vries, 2011 [34] Netherlands | Prospective cohort | 2000 | Girls and boys | 70 | Mean: 14.8 (range, 11.3–18.6) | No previous HT | Depression, Anxiety | No GAS before or during study | Moderate |
| de Vries, 2014 [35] Netherlands | Prospective cohortb,c | 2000 | Girls and boys | 55 | Mean: 14.8 (range, 11.5–18.5) | No previous HT | Depression, Anxiety | 100% had GAS during study | Serious |
| Achille, 2020 [30] US | Prospective cohort | 2013 | Girls and boys | 50 | Mean: 16.2 | No previous HT | QOL, Depression | No GAS before or during study | Moderate |
| López de Lara, 2020 [38] Spain | Prospective cohortb | 2018 | Girls and boys | 23 | Mean: 16 (range, 14-18) | No previous HT | Depression, Anxiety | No GAS before or during study | Moderate |
Abbreviations: ENIGI, European Network for the Investigation of Gender Incongruence; GAS, gender-affirming surgery; HT, hormone therapy; NR, not reported; QOL, quality of life.
bIncluded a cisgender control group or a comparison to general population norms
cAll participants were also included in de Vries (2011) [34]
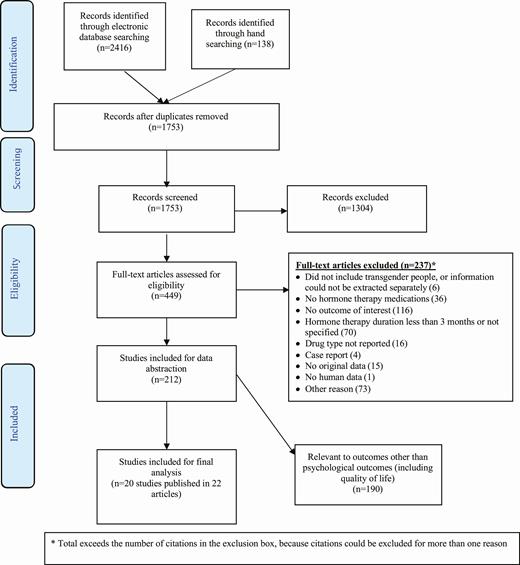
PRISMA flow diagram.
The time frame covered in the included studies began in 1972 [43], but most studies dated from post-2000. Eight studies were conducted in Italy [27-29, 31, 32, 36, 39, 41]; 2 each in Belgium [37, 48], the Netherlands [34, 35, 43, 44], the United States [30, 47], and Spain [38, 45]; and 1 in the United Kingdom [33], Turkey [42], and France [46]. One study recruited participants from Switzerland and Germany [40]. One study was part of the European Network for the Investigation of Gender Incongruence (ENIGI), which is a research collaborative between clinics providing gender-affirming care to transgender people in Ghent (Belgium), Amsterdam (Netherlands), Oslo (Norway), and Hamburg (Germany). The ENIGI study included in this review drew participants only from the Ghent clinic [37].
The study sizes ranged from 20 to 1331, although most had fewer than 60 participants. Fourteen studies reported on testosterone formulations in adult transgender men [27, 29, 31-33, 36, 39-46, 48]. These formulations were typically injectable testosterone cypionate or enanthate, although some studies used long-acting injectable testosterone undecanoate or daily transdermal gels. Ten studies reported on estrogen formulations in adult transgender women, usually in conjunction with an anti-androgen such as cyproterone acetate or spironolactone [28, 31, 33, 36, 37, 39, 43-47]. Estrogen formulations included transdermal, oral, or injectable estradiol (commonly estradiol valerate) or conjugated estrogens. Three studies reported on the psychological effects of GnRH therapy for puberty delay among mixed-gender groups of transgender adolescents [30, 34, 35, 38]. No study reported on hormone therapy among nonbinary people.
All studies that reported information about recruitment drew their participants largely or exclusively from specialized clinics dedicated to providing gender-affirming care for transgender people. These clinics were typically part of larger systems such as university hospitals. Clinic-based studies often applied strict eligibility criteria that included a period of psychiatric evaluation and a formal diagnosis of gender dysphoria before hormone therapy was initiated. Some studies also reported that psychological counseling was either available or required during the course of hormone therapy. In many cases, hormone therapy was considered a prerequisite for gender-affirming surgeries. The type and timing of gender-affirming surgeries and the proportion of participants for whom hormone therapy and surgeries were assessed simultaneously varied widely: some studies assessed only participants who had not had any type of gender-affirming surgery [27, 28, 30-32, 34, 36, 38-40, 42, 46, 47], while in others some or all participants underwent gender-affirming surgeries during the study period [29, 33, 35, 43-45, 48].
Quality of Life
Seven studies, including 1 RCT [27], 2 before-after trials [28, 29], 2 prospective cohorts [30, 39], and 2 cross-sectional studies [46, 48], assessed QOL (Table 2). An RCT found an improvement of approximately 5.5 points on a 10-point measure of life satisfaction across 3 groups of transgender men (n = 15 each) after 1 year of testosterone treatment (P < 0.05) [27]. A before-after trial similarly reported that life satisfaction scores almost doubled among transgender men (n = 50) over 5 years [29]. A prospective study found a 16% improvement in QOL scores among transgender women (n = 56) after 1 year of treatment (P < 0.05) but no change among transgender men (n = 27) [39]. Another before-after trial reported no difference in SF-36 scores among 2 groups of transgender women (n = 20 each) after 1 year [28]. Among adolescents, a mixed-gender prospective cohort (n = 50) showed no difference in QOL scores after a year of endocrine interventions, which included combinations of GnRH analogues and estrogen or testosterone formulations [30]. No study found that hormone therapy decreased QOL scores. We conclude that hormone therapy may improve QOL among transgender people. The strength of evidence for this conclusion is low due to concerns about bias in study designs, imprecision in measurement because of small sample sizes, and confounding by factors such as gender-affirming surgery status.
Effects of Gender-Affirming Hormone Therapy on Quality of Life Among Transgender People
| Author, year Study design | Transgender population | Treatment / comparison (n) | QOL measures | Length of treatment | Findings |
|---|---|---|---|---|---|
| Pelusi, 2014 [27] RCTa | Men | Testoviron depot (15) vs testosterone gel (15) vs testosterone undecanoate (15) | VAS (general life satisfaction) | 54 weeks | Mean QOL scores increased from 2.8 to 8.5 (P < 0.05) in the testoviron depot arm, from 3.2 to 8.9 (P < 0.05) in the testosterone gel arm, and from 2.6 to 8.0 (P < 0.05) in the testosterone undecanoate arm.d There was no difference across arms. |
| Gava, 2016 [28] Before-after trial | Women | Cyproterone acetate + estradiol (20) vs leuprolide acetate + estradiol (20) | VAS (general life satisfaction) SF-36 | 12 months | Mean QOL scores did not change in either arm. No comparisons across arms were reported. |
| Gava, 2018 [29] Before-after triala | Men | Testosterone undecanoate (25)c vs testosterone enanthate (25)c | VAS (general satisfaction) | 5 years | Mean QOL scores increased from 4.3 ± 3.1 to 8.1 ± 1.8 (P < 0.001) in the testosterone undecanoate arm and from 4.3 ± 3.8 to 8.3 ± 1.7 (P < 0.001) in the testosterone enanthate arm. No comparisons across arms were reported. |
| Manieri, 2014 [39] Prospective cohort | Women | HT (56) | WHOQOL | 12 months | Mean QOL scores increased from 62.5 to 72.2 (P < 0.05).d |
| Manieri, 2014 [39] Prospective cohort | Men | HT (27) | WHOQOL | 12 months | Mean QOL scores did not change. |
| Wierckx, 2011 [48] Cross-sectionalb | Men | HT (47)c | SF-36 | At least 3 years | Mean QOL scores on the VT and MH subscales were lower for transgender men than cisgender men (VT subscale: 62.1 ± 20.7 vs 71.9 ± 18.3, P = 0.002; MH subscale: 72.6 ± 19.2 vs 79.3 ± 16.4, P = 0.020). There were no other differences between transgender men and either cisgender men or cisgender women. |
| Gorin-Lazard, 2012 [46] Cross-sectionalb | Women and men | HT (44) vs no HT (17) | SF-36 | Median: 20 months (range, 12–42 months) | Mean QOL scores were generally higher in the group receiving HT vs the group not receiving HT (MCS: 51.0 ± 7.7 vs 39.8 ± 12.7, P = 0.003; MH subscale: 76.4 ± 14.1 vs 59.1 ± 19.6, P = 0.004; RE subscale: 88.6 ± 22.7 vs 54.9 ± 40.7, P = 0.001; SF subscale: 83.2 ± 23.3 vs 69.9 ± 24.2, P = 0.026). There were no differences in the other subscales. |
| Achille, 2020 [30] Prospective cohort | Girls and boys | GnRH treatment + HT (47) | Q-LES-Q-SF | 12 months | Mean QOL scores did not change. |
| Author, year Study design | Transgender population | Treatment / comparison (n) | QOL measures | Length of treatment | Findings |
|---|---|---|---|---|---|
| Pelusi, 2014 [27] RCTa | Men | Testoviron depot (15) vs testosterone gel (15) vs testosterone undecanoate (15) | VAS (general life satisfaction) | 54 weeks | Mean QOL scores increased from 2.8 to 8.5 (P < 0.05) in the testoviron depot arm, from 3.2 to 8.9 (P < 0.05) in the testosterone gel arm, and from 2.6 to 8.0 (P < 0.05) in the testosterone undecanoate arm.d There was no difference across arms. |
| Gava, 2016 [28] Before-after trial | Women | Cyproterone acetate + estradiol (20) vs leuprolide acetate + estradiol (20) | VAS (general life satisfaction) SF-36 | 12 months | Mean QOL scores did not change in either arm. No comparisons across arms were reported. |
| Gava, 2018 [29] Before-after triala | Men | Testosterone undecanoate (25)c vs testosterone enanthate (25)c | VAS (general satisfaction) | 5 years | Mean QOL scores increased from 4.3 ± 3.1 to 8.1 ± 1.8 (P < 0.001) in the testosterone undecanoate arm and from 4.3 ± 3.8 to 8.3 ± 1.7 (P < 0.001) in the testosterone enanthate arm. No comparisons across arms were reported. |
| Manieri, 2014 [39] Prospective cohort | Women | HT (56) | WHOQOL | 12 months | Mean QOL scores increased from 62.5 to 72.2 (P < 0.05).d |
| Manieri, 2014 [39] Prospective cohort | Men | HT (27) | WHOQOL | 12 months | Mean QOL scores did not change. |
| Wierckx, 2011 [48] Cross-sectionalb | Men | HT (47)c | SF-36 | At least 3 years | Mean QOL scores on the VT and MH subscales were lower for transgender men than cisgender men (VT subscale: 62.1 ± 20.7 vs 71.9 ± 18.3, P = 0.002; MH subscale: 72.6 ± 19.2 vs 79.3 ± 16.4, P = 0.020). There were no other differences between transgender men and either cisgender men or cisgender women. |
| Gorin-Lazard, 2012 [46] Cross-sectionalb | Women and men | HT (44) vs no HT (17) | SF-36 | Median: 20 months (range, 12–42 months) | Mean QOL scores were generally higher in the group receiving HT vs the group not receiving HT (MCS: 51.0 ± 7.7 vs 39.8 ± 12.7, P = 0.003; MH subscale: 76.4 ± 14.1 vs 59.1 ± 19.6, P = 0.004; RE subscale: 88.6 ± 22.7 vs 54.9 ± 40.7, P = 0.001; SF subscale: 83.2 ± 23.3 vs 69.9 ± 24.2, P = 0.026). There were no differences in the other subscales. |
| Achille, 2020 [30] Prospective cohort | Girls and boys | GnRH treatment + HT (47) | Q-LES-Q-SF | 12 months | Mean QOL scores did not change. |
Abbreviations: GnRH, gonadotropin-releasing hormone; HT, hormone therapy; MCS, Mental Component Summary; MH, mental health; QOL, quality of life; RCT, randomized controlled trial; RE, role functioning/emotional; SF, social functioning; SF-36, Short Form-36 Health Survey; VAS, visual analog scale; VT, vitality; WHOQOL, World Health Organization Quality of Life measure.
a10 participants on testosterone enanthate and 15 participants on testosterone undecanoate were included in both Pelusi [27] and Gava (2018) [29]
bIncluded a cisgender control group or a comparison to general population norms
cIncluded participants who had undergone gender-affirming surgery/surgeries, or surgery status not reported
dNo standard deviations reported
Effects of Gender-Affirming Hormone Therapy on Quality of Life Among Transgender People
| Author, year Study design | Transgender population | Treatment / comparison (n) | QOL measures | Length of treatment | Findings |
|---|---|---|---|---|---|
| Pelusi, 2014 [27] RCTa | Men | Testoviron depot (15) vs testosterone gel (15) vs testosterone undecanoate (15) | VAS (general life satisfaction) | 54 weeks | Mean QOL scores increased from 2.8 to 8.5 (P < 0.05) in the testoviron depot arm, from 3.2 to 8.9 (P < 0.05) in the testosterone gel arm, and from 2.6 to 8.0 (P < 0.05) in the testosterone undecanoate arm.d There was no difference across arms. |
| Gava, 2016 [28] Before-after trial | Women | Cyproterone acetate + estradiol (20) vs leuprolide acetate + estradiol (20) | VAS (general life satisfaction) SF-36 | 12 months | Mean QOL scores did not change in either arm. No comparisons across arms were reported. |
| Gava, 2018 [29] Before-after triala | Men | Testosterone undecanoate (25)c vs testosterone enanthate (25)c | VAS (general satisfaction) | 5 years | Mean QOL scores increased from 4.3 ± 3.1 to 8.1 ± 1.8 (P < 0.001) in the testosterone undecanoate arm and from 4.3 ± 3.8 to 8.3 ± 1.7 (P < 0.001) in the testosterone enanthate arm. No comparisons across arms were reported. |
| Manieri, 2014 [39] Prospective cohort | Women | HT (56) | WHOQOL | 12 months | Mean QOL scores increased from 62.5 to 72.2 (P < 0.05).d |
| Manieri, 2014 [39] Prospective cohort | Men | HT (27) | WHOQOL | 12 months | Mean QOL scores did not change. |
| Wierckx, 2011 [48] Cross-sectionalb | Men | HT (47)c | SF-36 | At least 3 years | Mean QOL scores on the VT and MH subscales were lower for transgender men than cisgender men (VT subscale: 62.1 ± 20.7 vs 71.9 ± 18.3, P = 0.002; MH subscale: 72.6 ± 19.2 vs 79.3 ± 16.4, P = 0.020). There were no other differences between transgender men and either cisgender men or cisgender women. |
| Gorin-Lazard, 2012 [46] Cross-sectionalb | Women and men | HT (44) vs no HT (17) | SF-36 | Median: 20 months (range, 12–42 months) | Mean QOL scores were generally higher in the group receiving HT vs the group not receiving HT (MCS: 51.0 ± 7.7 vs 39.8 ± 12.7, P = 0.003; MH subscale: 76.4 ± 14.1 vs 59.1 ± 19.6, P = 0.004; RE subscale: 88.6 ± 22.7 vs 54.9 ± 40.7, P = 0.001; SF subscale: 83.2 ± 23.3 vs 69.9 ± 24.2, P = 0.026). There were no differences in the other subscales. |
| Achille, 2020 [30] Prospective cohort | Girls and boys | GnRH treatment + HT (47) | Q-LES-Q-SF | 12 months | Mean QOL scores did not change. |
| Author, year Study design | Transgender population | Treatment / comparison (n) | QOL measures | Length of treatment | Findings |
|---|---|---|---|---|---|
| Pelusi, 2014 [27] RCTa | Men | Testoviron depot (15) vs testosterone gel (15) vs testosterone undecanoate (15) | VAS (general life satisfaction) | 54 weeks | Mean QOL scores increased from 2.8 to 8.5 (P < 0.05) in the testoviron depot arm, from 3.2 to 8.9 (P < 0.05) in the testosterone gel arm, and from 2.6 to 8.0 (P < 0.05) in the testosterone undecanoate arm.d There was no difference across arms. |
| Gava, 2016 [28] Before-after trial | Women | Cyproterone acetate + estradiol (20) vs leuprolide acetate + estradiol (20) | VAS (general life satisfaction) SF-36 | 12 months | Mean QOL scores did not change in either arm. No comparisons across arms were reported. |
| Gava, 2018 [29] Before-after triala | Men | Testosterone undecanoate (25)c vs testosterone enanthate (25)c | VAS (general satisfaction) | 5 years | Mean QOL scores increased from 4.3 ± 3.1 to 8.1 ± 1.8 (P < 0.001) in the testosterone undecanoate arm and from 4.3 ± 3.8 to 8.3 ± 1.7 (P < 0.001) in the testosterone enanthate arm. No comparisons across arms were reported. |
| Manieri, 2014 [39] Prospective cohort | Women | HT (56) | WHOQOL | 12 months | Mean QOL scores increased from 62.5 to 72.2 (P < 0.05).d |
| Manieri, 2014 [39] Prospective cohort | Men | HT (27) | WHOQOL | 12 months | Mean QOL scores did not change. |
| Wierckx, 2011 [48] Cross-sectionalb | Men | HT (47)c | SF-36 | At least 3 years | Mean QOL scores on the VT and MH subscales were lower for transgender men than cisgender men (VT subscale: 62.1 ± 20.7 vs 71.9 ± 18.3, P = 0.002; MH subscale: 72.6 ± 19.2 vs 79.3 ± 16.4, P = 0.020). There were no other differences between transgender men and either cisgender men or cisgender women. |
| Gorin-Lazard, 2012 [46] Cross-sectionalb | Women and men | HT (44) vs no HT (17) | SF-36 | Median: 20 months (range, 12–42 months) | Mean QOL scores were generally higher in the group receiving HT vs the group not receiving HT (MCS: 51.0 ± 7.7 vs 39.8 ± 12.7, P = 0.003; MH subscale: 76.4 ± 14.1 vs 59.1 ± 19.6, P = 0.004; RE subscale: 88.6 ± 22.7 vs 54.9 ± 40.7, P = 0.001; SF subscale: 83.2 ± 23.3 vs 69.9 ± 24.2, P = 0.026). There were no differences in the other subscales. |
| Achille, 2020 [30] Prospective cohort | Girls and boys | GnRH treatment + HT (47) | Q-LES-Q-SF | 12 months | Mean QOL scores did not change. |
Abbreviations: GnRH, gonadotropin-releasing hormone; HT, hormone therapy; MCS, Mental Component Summary; MH, mental health; QOL, quality of life; RCT, randomized controlled trial; RE, role functioning/emotional; SF, social functioning; SF-36, Short Form-36 Health Survey; VAS, visual analog scale; VT, vitality; WHOQOL, World Health Organization Quality of Life measure.
a10 participants on testosterone enanthate and 15 participants on testosterone undecanoate were included in both Pelusi [27] and Gava (2018) [29]
bIncluded a cisgender control group or a comparison to general population norms
cIncluded participants who had undergone gender-affirming surgery/surgeries, or surgery status not reported
dNo standard deviations reported
Depression
Twelve studies, including 1 before-after trial [28], 9 prospective cohorts [30-36, 38, 40, 42], and 2 cross-sectional studies [45, 47], assessed depression (Table 3). A prospective study found that the proportion of transgender men and transgender women (n = 107) showing symptoms of depression decreased from 42% to 22% over 12 months of treatment (P < 0.001) [31]. In 2 other prospective cohorts, Beck Depression Inventory (BDI-II) scores improved by more than half among both transgender men (n = 26) and transgender women (n = 28) after 24 months of therapy (P < 0.001) [36] and improved from 15.7 ± 12.3 to 8.1 ± 6.2 among transgender men (n = 23) after 6 months (P < 0.001) [40]. A fourth prospective study reported improvements of 1.05 points (95% CI: −1.87, −0.22) and 1.42 points (95% CI: −2.61, −0.24) on the 21-point Hospital Anxiety and Depression Scale (HADS) among 91 transgender women and 64 transgender men after 12 months (P = 0.013 and P = 0.019, respectively) [33]. A before-after trial, however, found no change in BDI-II scores among 2 groups of transgender women (n = 20 each) after 1 year [28]. Two prospective studies reported no difference among transgender men (n = 37) after 24 weeks [42] or among transgender men (n = 50) after 12 months [32], although in the latter study this outcome did not change from a baseline median of 0.0 (“not at all depressed”) on an unvalidated 4-point scale. Among adolescents, 2 mixed-gender prospective cohorts (n = 50 and n = 23, respectively) showed improvements in depression scores after 1 year of treatment with GnRH analogues and estrogen or testosterone formulations (both P < 0.001) [30, 38]. Another prospective study reported that BDI scores improved almost by half among adolescents (n = 41) after a mean of 1.88 years of treatment with GnRH analogues to delay puberty (P = 0.004) [34]. The overall improvement after several subsequent years of testosterone or estrogen therapy in this cohort (n = 32) was smaller, however, resulting in no significant change from baseline [35]. No study found that hormone therapy increased depression. We conclude that hormone therapy may decrease depression among transgender people. The strength of evidence for this conclusion is low due to concerns about study designs, small sample sizes, and confounding.
Effects of Gender-Affirming Hormone Therapy on Depression Among Transgender People
| Author, year Study design | Transgender population | Treatment / comparison (n) | Depression measures | Length of treatment | Findings |
|---|---|---|---|---|---|
| Gava, 2016 [28] Before-after trial | Women | Cyproterone acetate + estradiol (20) vs Leuprolide acetate + estradiol (20) | BDI-II | 12 months | Mean depression scores did not change in either arm. No comparisons across arms were reported. |
| Fisher, 2016 [37] Prospective cohort | Women | HT (28) | BDI-II | 24 months | Mean depression score decreased from 10.12 to 4.58 (P < 0.001).d, e |
| Defreyne, 2018 [33] Prospective cohort | Women | HT (91)c | HADS (depression subscale) | 1 year | Median depression score decreased by 1.05 (95% CI: −1.87, −0.22) on a 21-point scale (P = 0.013). |
| Costantino, 2013 [32] Prospective cohort | Men | HT (50) | Ad hoc questionnaire | 12 months | Depression score did not change from a median of 0.0 at baseline (IQR: 0.0, 1.0). |
| Fisher, 2016 [36] Prospective cohort | Men | HT (26) | BDI-II | 24 months | Mean depression score decreased from 9.31 to 4.25 (P < 0.001).d, e |
| Defreyne, 2018 [33] Prospective cohort | Men | HT (64)c | HADS (depression subscale) | 1 year | Median depression score decreased by 1.42 (95% CI: −2.61, −0.24) on a 21-point scale (P = 0.019). |
| Turan, 2018 [42] Prospective cohortb | Men | HT (37) | SCL-90-R (depression subscale) | 24 weeks | Mean depression score did not change. |
| Metzger, 2019 [40] Prospective cohortb | Men | HT (23) | BDI-II | 6 months | Mean depression score decreased from 15.7 ± 12.3 to 8.1 ± 6.2 (P < 0.001). |
| Colizzi, 2014 [31] Prospective cohort | Women and men | HT (107) | Zung SDS SCL-90-R (depression subscale) | 12 months | Mean Zung SDS score improved from 48.40 ± 10.5 to 39.98 ± 10.79 (P < 0.001), and the proportion with Zung SDS scores indicating mild, moderate, or severe depression (vs no depression) decreased from 42% to 22% (χ 2 = 19.05, P < 0.001). Mean SCL-90-R score decreased from 0.83 ± 0.74 to 0.51 ± 0.49 (P < 0.001), which represents an improvement from possible borderline depression to no depression. |
| Leavitt, 1980 [47] Cross-sectional | Women | HT (22) vs No HT (19) | MMPI (depression subscale) | At least 12 months | Mean depression score was lower in the group receiving HT vs the group not receiving HT (53.1 ± 14.7 vs 65.7 ± 11.2, P = 0.004). |
| Gómez-Gil, 2012 [45] Cross-sectional | Women and men | HT (120)c vs No HT (67)c | HADS (depression subscale) | Mean: 11.0 years (women, range, 1–46 years); 4.7 years (men, range, 1–22 years) | Mean depression score was lower in the group receiving HT vs the group not receiving HT (3.3 ± 3.2 vs 5.2 ± 4.2, P = 0.002).f The proportion with scores indicating depression (vs no depression) was larger in the group not receiving HT (31% vs 8%, χ 2 = 16.46, P = 0.001).f |
| de Vries, 2011 [34] Prospective cohort | Girls and boys | GnRH treatment (41) | BDI | 1.88 years | Mean depression score decreased from 8.31 ± 7.12 to 4.95 ± 6.72 (P = 0.004). |
| de Vries, 2014 [35] Prospective cohorta,b | Girls and boys | GnRH treatment + HT (32)c | BDI | 5.9 years | Mean depression score did not change. |
| Achille, 2020 [30] Prospective cohort | Girls and boys | GnRH treatment + HT (47) | CESD-R, PHQ-9 (modified for adolescents) | 12 months | Mean CESD-R score decreased from 21.4 to 13.9 (P < 0.001); d a score of <16 indicates no clinical depression. Mean PHQ-9 score decreased from 9.0 to 5.4 (P < 0.001).d |
| López de Lara, 2020 [38] Prospective cohortb | Girls and boys | GnRH treatment + HT (23) | BDI-II | 1 year | Mean depression score decreased from 19.3 ± 5.5 to 9.7 ± 3.9 (P < 0.001). |
| Author, year Study design | Transgender population | Treatment / comparison (n) | Depression measures | Length of treatment | Findings |
|---|---|---|---|---|---|
| Gava, 2016 [28] Before-after trial | Women | Cyproterone acetate + estradiol (20) vs Leuprolide acetate + estradiol (20) | BDI-II | 12 months | Mean depression scores did not change in either arm. No comparisons across arms were reported. |
| Fisher, 2016 [37] Prospective cohort | Women | HT (28) | BDI-II | 24 months | Mean depression score decreased from 10.12 to 4.58 (P < 0.001).d, e |
| Defreyne, 2018 [33] Prospective cohort | Women | HT (91)c | HADS (depression subscale) | 1 year | Median depression score decreased by 1.05 (95% CI: −1.87, −0.22) on a 21-point scale (P = 0.013). |
| Costantino, 2013 [32] Prospective cohort | Men | HT (50) | Ad hoc questionnaire | 12 months | Depression score did not change from a median of 0.0 at baseline (IQR: 0.0, 1.0). |
| Fisher, 2016 [36] Prospective cohort | Men | HT (26) | BDI-II | 24 months | Mean depression score decreased from 9.31 to 4.25 (P < 0.001).d, e |
| Defreyne, 2018 [33] Prospective cohort | Men | HT (64)c | HADS (depression subscale) | 1 year | Median depression score decreased by 1.42 (95% CI: −2.61, −0.24) on a 21-point scale (P = 0.019). |
| Turan, 2018 [42] Prospective cohortb | Men | HT (37) | SCL-90-R (depression subscale) | 24 weeks | Mean depression score did not change. |
| Metzger, 2019 [40] Prospective cohortb | Men | HT (23) | BDI-II | 6 months | Mean depression score decreased from 15.7 ± 12.3 to 8.1 ± 6.2 (P < 0.001). |
| Colizzi, 2014 [31] Prospective cohort | Women and men | HT (107) | Zung SDS SCL-90-R (depression subscale) | 12 months | Mean Zung SDS score improved from 48.40 ± 10.5 to 39.98 ± 10.79 (P < 0.001), and the proportion with Zung SDS scores indicating mild, moderate, or severe depression (vs no depression) decreased from 42% to 22% (χ 2 = 19.05, P < 0.001). Mean SCL-90-R score decreased from 0.83 ± 0.74 to 0.51 ± 0.49 (P < 0.001), which represents an improvement from possible borderline depression to no depression. |
| Leavitt, 1980 [47] Cross-sectional | Women | HT (22) vs No HT (19) | MMPI (depression subscale) | At least 12 months | Mean depression score was lower in the group receiving HT vs the group not receiving HT (53.1 ± 14.7 vs 65.7 ± 11.2, P = 0.004). |
| Gómez-Gil, 2012 [45] Cross-sectional | Women and men | HT (120)c vs No HT (67)c | HADS (depression subscale) | Mean: 11.0 years (women, range, 1–46 years); 4.7 years (men, range, 1–22 years) | Mean depression score was lower in the group receiving HT vs the group not receiving HT (3.3 ± 3.2 vs 5.2 ± 4.2, P = 0.002).f The proportion with scores indicating depression (vs no depression) was larger in the group not receiving HT (31% vs 8%, χ 2 = 16.46, P = 0.001).f |
| de Vries, 2011 [34] Prospective cohort | Girls and boys | GnRH treatment (41) | BDI | 1.88 years | Mean depression score decreased from 8.31 ± 7.12 to 4.95 ± 6.72 (P = 0.004). |
| de Vries, 2014 [35] Prospective cohorta,b | Girls and boys | GnRH treatment + HT (32)c | BDI | 5.9 years | Mean depression score did not change. |
| Achille, 2020 [30] Prospective cohort | Girls and boys | GnRH treatment + HT (47) | CESD-R, PHQ-9 (modified for adolescents) | 12 months | Mean CESD-R score decreased from 21.4 to 13.9 (P < 0.001); d a score of <16 indicates no clinical depression. Mean PHQ-9 score decreased from 9.0 to 5.4 (P < 0.001).d |
| López de Lara, 2020 [38] Prospective cohortb | Girls and boys | GnRH treatment + HT (23) | BDI-II | 1 year | Mean depression score decreased from 19.3 ± 5.5 to 9.7 ± 3.9 (P < 0.001). |
Abbreviations: BDI/BDI-II, Beck Depression Inventory; GAS, gender-affirming surgery; GnRH, gonadotropin-releasing hormone; HADS, Hospital Anxiety and Depression Scale; HT, hormone therapy; IQR, interquartile range; MMPI, Minnesota Multiphasic Personality Inventory; NA, not applicable; SCL-90-R, Symptom Checklist 90-Revised; Zung SDS, Zung Self-Rating Depression Scale.
aAll participants were also included in de Vries (2011) [34]
bIncluded a cisgender control group or a comparison to general population norms
cIncluded participants who had undergone gender-affirming surgery/surgeries, or surgery status not reported
dNo standard deviations reported
eAdjusted for age, gender role, and surgery status fAdjusted for age, gender, and education level
Effects of Gender-Affirming Hormone Therapy on Depression Among Transgender People
| Author, year Study design | Transgender population | Treatment / comparison (n) | Depression measures | Length of treatment | Findings |
|---|---|---|---|---|---|
| Gava, 2016 [28] Before-after trial | Women | Cyproterone acetate + estradiol (20) vs Leuprolide acetate + estradiol (20) | BDI-II | 12 months | Mean depression scores did not change in either arm. No comparisons across arms were reported. |
| Fisher, 2016 [37] Prospective cohort | Women | HT (28) | BDI-II | 24 months | Mean depression score decreased from 10.12 to 4.58 (P < 0.001).d, e |
| Defreyne, 2018 [33] Prospective cohort | Women | HT (91)c | HADS (depression subscale) | 1 year | Median depression score decreased by 1.05 (95% CI: −1.87, −0.22) on a 21-point scale (P = 0.013). |
| Costantino, 2013 [32] Prospective cohort | Men | HT (50) | Ad hoc questionnaire | 12 months | Depression score did not change from a median of 0.0 at baseline (IQR: 0.0, 1.0). |
| Fisher, 2016 [36] Prospective cohort | Men | HT (26) | BDI-II | 24 months | Mean depression score decreased from 9.31 to 4.25 (P < 0.001).d, e |
| Defreyne, 2018 [33] Prospective cohort | Men | HT (64)c | HADS (depression subscale) | 1 year | Median depression score decreased by 1.42 (95% CI: −2.61, −0.24) on a 21-point scale (P = 0.019). |
| Turan, 2018 [42] Prospective cohortb | Men | HT (37) | SCL-90-R (depression subscale) | 24 weeks | Mean depression score did not change. |
| Metzger, 2019 [40] Prospective cohortb | Men | HT (23) | BDI-II | 6 months | Mean depression score decreased from 15.7 ± 12.3 to 8.1 ± 6.2 (P < 0.001). |
| Colizzi, 2014 [31] Prospective cohort | Women and men | HT (107) | Zung SDS SCL-90-R (depression subscale) | 12 months | Mean Zung SDS score improved from 48.40 ± 10.5 to 39.98 ± 10.79 (P < 0.001), and the proportion with Zung SDS scores indicating mild, moderate, or severe depression (vs no depression) decreased from 42% to 22% (χ 2 = 19.05, P < 0.001). Mean SCL-90-R score decreased from 0.83 ± 0.74 to 0.51 ± 0.49 (P < 0.001), which represents an improvement from possible borderline depression to no depression. |
| Leavitt, 1980 [47] Cross-sectional | Women | HT (22) vs No HT (19) | MMPI (depression subscale) | At least 12 months | Mean depression score was lower in the group receiving HT vs the group not receiving HT (53.1 ± 14.7 vs 65.7 ± 11.2, P = 0.004). |
| Gómez-Gil, 2012 [45] Cross-sectional | Women and men | HT (120)c vs No HT (67)c | HADS (depression subscale) | Mean: 11.0 years (women, range, 1–46 years); 4.7 years (men, range, 1–22 years) | Mean depression score was lower in the group receiving HT vs the group not receiving HT (3.3 ± 3.2 vs 5.2 ± 4.2, P = 0.002).f The proportion with scores indicating depression (vs no depression) was larger in the group not receiving HT (31% vs 8%, χ 2 = 16.46, P = 0.001).f |
| de Vries, 2011 [34] Prospective cohort | Girls and boys | GnRH treatment (41) | BDI | 1.88 years | Mean depression score decreased from 8.31 ± 7.12 to 4.95 ± 6.72 (P = 0.004). |
| de Vries, 2014 [35] Prospective cohorta,b | Girls and boys | GnRH treatment + HT (32)c | BDI | 5.9 years | Mean depression score did not change. |
| Achille, 2020 [30] Prospective cohort | Girls and boys | GnRH treatment + HT (47) | CESD-R, PHQ-9 (modified for adolescents) | 12 months | Mean CESD-R score decreased from 21.4 to 13.9 (P < 0.001); d a score of <16 indicates no clinical depression. Mean PHQ-9 score decreased from 9.0 to 5.4 (P < 0.001).d |
| López de Lara, 2020 [38] Prospective cohortb | Girls and boys | GnRH treatment + HT (23) | BDI-II | 1 year | Mean depression score decreased from 19.3 ± 5.5 to 9.7 ± 3.9 (P < 0.001). |
| Author, year Study design | Transgender population | Treatment / comparison (n) | Depression measures | Length of treatment | Findings |
|---|---|---|---|---|---|
| Gava, 2016 [28] Before-after trial | Women | Cyproterone acetate + estradiol (20) vs Leuprolide acetate + estradiol (20) | BDI-II | 12 months | Mean depression scores did not change in either arm. No comparisons across arms were reported. |
| Fisher, 2016 [37] Prospective cohort | Women | HT (28) | BDI-II | 24 months | Mean depression score decreased from 10.12 to 4.58 (P < 0.001).d, e |
| Defreyne, 2018 [33] Prospective cohort | Women | HT (91)c | HADS (depression subscale) | 1 year | Median depression score decreased by 1.05 (95% CI: −1.87, −0.22) on a 21-point scale (P = 0.013). |
| Costantino, 2013 [32] Prospective cohort | Men | HT (50) | Ad hoc questionnaire | 12 months | Depression score did not change from a median of 0.0 at baseline (IQR: 0.0, 1.0). |
| Fisher, 2016 [36] Prospective cohort | Men | HT (26) | BDI-II | 24 months | Mean depression score decreased from 9.31 to 4.25 (P < 0.001).d, e |
| Defreyne, 2018 [33] Prospective cohort | Men | HT (64)c | HADS (depression subscale) | 1 year | Median depression score decreased by 1.42 (95% CI: −2.61, −0.24) on a 21-point scale (P = 0.019). |
| Turan, 2018 [42] Prospective cohortb | Men | HT (37) | SCL-90-R (depression subscale) | 24 weeks | Mean depression score did not change. |
| Metzger, 2019 [40] Prospective cohortb | Men | HT (23) | BDI-II | 6 months | Mean depression score decreased from 15.7 ± 12.3 to 8.1 ± 6.2 (P < 0.001). |
| Colizzi, 2014 [31] Prospective cohort | Women and men | HT (107) | Zung SDS SCL-90-R (depression subscale) | 12 months | Mean Zung SDS score improved from 48.40 ± 10.5 to 39.98 ± 10.79 (P < 0.001), and the proportion with Zung SDS scores indicating mild, moderate, or severe depression (vs no depression) decreased from 42% to 22% (χ 2 = 19.05, P < 0.001). Mean SCL-90-R score decreased from 0.83 ± 0.74 to 0.51 ± 0.49 (P < 0.001), which represents an improvement from possible borderline depression to no depression. |
| Leavitt, 1980 [47] Cross-sectional | Women | HT (22) vs No HT (19) | MMPI (depression subscale) | At least 12 months | Mean depression score was lower in the group receiving HT vs the group not receiving HT (53.1 ± 14.7 vs 65.7 ± 11.2, P = 0.004). |
| Gómez-Gil, 2012 [45] Cross-sectional | Women and men | HT (120)c vs No HT (67)c | HADS (depression subscale) | Mean: 11.0 years (women, range, 1–46 years); 4.7 years (men, range, 1–22 years) | Mean depression score was lower in the group receiving HT vs the group not receiving HT (3.3 ± 3.2 vs 5.2 ± 4.2, P = 0.002).f The proportion with scores indicating depression (vs no depression) was larger in the group not receiving HT (31% vs 8%, χ 2 = 16.46, P = 0.001).f |
| de Vries, 2011 [34] Prospective cohort | Girls and boys | GnRH treatment (41) | BDI | 1.88 years | Mean depression score decreased from 8.31 ± 7.12 to 4.95 ± 6.72 (P = 0.004). |
| de Vries, 2014 [35] Prospective cohorta,b | Girls and boys | GnRH treatment + HT (32)c | BDI | 5.9 years | Mean depression score did not change. |
| Achille, 2020 [30] Prospective cohort | Girls and boys | GnRH treatment + HT (47) | CESD-R, PHQ-9 (modified for adolescents) | 12 months | Mean CESD-R score decreased from 21.4 to 13.9 (P < 0.001); d a score of <16 indicates no clinical depression. Mean PHQ-9 score decreased from 9.0 to 5.4 (P < 0.001).d |
| López de Lara, 2020 [38] Prospective cohortb | Girls and boys | GnRH treatment + HT (23) | BDI-II | 1 year | Mean depression score decreased from 19.3 ± 5.5 to 9.7 ± 3.9 (P < 0.001). |
Abbreviations: BDI/BDI-II, Beck Depression Inventory; GAS, gender-affirming surgery; GnRH, gonadotropin-releasing hormone; HADS, Hospital Anxiety and Depression Scale; HT, hormone therapy; IQR, interquartile range; MMPI, Minnesota Multiphasic Personality Inventory; NA, not applicable; SCL-90-R, Symptom Checklist 90-Revised; Zung SDS, Zung Self-Rating Depression Scale.
aAll participants were also included in de Vries (2011) [34]
bIncluded a cisgender control group or a comparison to general population norms
cIncluded participants who had undergone gender-affirming surgery/surgeries, or surgery status not reported
dNo standard deviations reported
eAdjusted for age, gender role, and surgery status fAdjusted for age, gender, and education level
Anxiety
Eight studies, including 7 prospective cohorts [31, 33-35, 37, 38, 41, 42] and 1 cross-sectional study [45], assessed anxiety (Table 4). One prospective study found that Symptom Checklist 90-Revised scores indicating a probable anxiety disorder among a mixed-gender group of adults (n = 107) improved from borderline to normal over 12 months (P < 0.001) [31]. Another prospective study, however, did not find a difference in HADS anxiety scores among either transgender men (n = 64) or transgender women (n = 91) after 1 year [33], and a third study reported no change in the number of transgender men (6/52, 12%) with a diagnosed anxiety disorder after 7 months [41]. Likewise, 2 other prospective studies found no difference in anxiety scores among transgender men (n = 37) after 24 weeks of treatment [42] or transgender women (n = 20) after 12 months [37], although this latter finding represented no change from a baseline median score of 0 (answering “no” to the question, “do you feel anxious?”) on an unvalidated 3-point scale. Among adolescents, 1 prospective study saw mean anxiety scores in a mixed-gender group (n = 23) improve from 33.0 ± 7.2 to 18.5 ± 8.4 after 1 year (P < 0.001) [38], but another reported no changes in anxiety after approximately 2 years of puberty delay treatment with GnRH analogues and 4 years of hormone therapy (n = 32) [35]. No study found that hormone therapy increased anxiety. We conclude that hormone therapy may decrease anxiety among transgender people. The strength of evidence for this conclusion is low due to concerns about study designs, small sample sizes, and confounding.
Effects of Gender-Affirming Hormone Therapy on Anxiety Among Transgender People
| Author, year | Transgender population | Treatment / comparison (n) | Anxiety measures | Length of treatment | Findings |
|---|---|---|---|---|---|
| Fuss, 2015 [37] Prospective cohort | Women | HT (20)c | Ad hoc questionnaire | 12 months | Anxiety score did not change from a median of 0.0 at baseline. |
| Defreyne, 2018 [33] Prospective cohort | Women | HT (91)c | HADS (anxiety subscale) | 1 year | Median anxiety score did not change. |
| Defreyne, 2018 [33] Prospective cohort | Men | HT (64)c | HADS (anxiety subscale) | 1 year | Median anxiety score did not change. |
| Motta, 2018 [41] Prospective cohort | Men | HT (46)c | DSM | 7 months | Proportion diagnosed with an anxiety disorder (6/46, 12%) did not change. |
| Turan, 2018 [42] Prospective cohortb | Men | HT (37) | SCL-90-R (anxiety subscale) | 24 weeks | Mean anxiety score did not change. |
| Colizzi, 2014 [31] Prospective cohort | Women and men | HT (107) | SCL-90-R (anxiety subscale) Zung SAS | 12 months | Mean SCL-90-R score decreased from 1.05 ± 0.95 to 0.54 ± 0.56 (P < 0.001), which represents an improvement from borderline anxiety disorder to no anxiety disorder. Mean Zung SAS score improved from 44.91 ± 9.59 to 37.90 ± 8.97 (P < 0.001), and the proportion with Zung SAS scores indicating mild, moderate, or severe anxiety (vs no anxiety) decreased from 50% to 17% (χ 2 = 33.03, P < 0.001). |
| Gómez-Gil, 2012 [45] Cross-sectional | Women and men | HT (120)c vs No HT (67)c | HADS (anxiety subscale) SADS | Mean: 11.0 years (women, range, 1-46 years); 4.7 years (men, range, 1-22 years) | Mean HADS and SADS scores were lower in the group receiving HT vs the group not receiving HT (6.4 ± 3.7 vs 9.0 ± 4.0, P = 0.001; 8.5 ± 7.8 vs 11.0 ± 7.3, P = 0.038, respectively).d The proportion with scores indicating anxiety (vs no anxiety) was higher in the group not receiving HT (χ 2 = 14.46, P < 0.001).d |
| de Vries, 2011 [34] Prospective cohort | Girls and boys | GnRH treatment (41) | STAI (trait subscale) | 1.88 years | Mean anxiety score did not change. |
| de Vries, 2014 [35] Prospective cohorta,b | Girls and boys | GnRH treatment + HT (32)c | STAI (trait subscale) | 5.9 years | Mean anxiety score did not change. |
| López de Lara, 2020 [38] Prospective cohortb | Girls and boys | GnRH treatment + HT (23) | STAI (trait subscale) | 1 year | Mean anxiety score decreased from 33.0 ± 7.2 to 18.5 ± 8.4 (P < 0.001). |
| Author, year | Transgender population | Treatment / comparison (n) | Anxiety measures | Length of treatment | Findings |
|---|---|---|---|---|---|
| Fuss, 2015 [37] Prospective cohort | Women | HT (20)c | Ad hoc questionnaire | 12 months | Anxiety score did not change from a median of 0.0 at baseline. |
| Defreyne, 2018 [33] Prospective cohort | Women | HT (91)c | HADS (anxiety subscale) | 1 year | Median anxiety score did not change. |
| Defreyne, 2018 [33] Prospective cohort | Men | HT (64)c | HADS (anxiety subscale) | 1 year | Median anxiety score did not change. |
| Motta, 2018 [41] Prospective cohort | Men | HT (46)c | DSM | 7 months | Proportion diagnosed with an anxiety disorder (6/46, 12%) did not change. |
| Turan, 2018 [42] Prospective cohortb | Men | HT (37) | SCL-90-R (anxiety subscale) | 24 weeks | Mean anxiety score did not change. |
| Colizzi, 2014 [31] Prospective cohort | Women and men | HT (107) | SCL-90-R (anxiety subscale) Zung SAS | 12 months | Mean SCL-90-R score decreased from 1.05 ± 0.95 to 0.54 ± 0.56 (P < 0.001), which represents an improvement from borderline anxiety disorder to no anxiety disorder. Mean Zung SAS score improved from 44.91 ± 9.59 to 37.90 ± 8.97 (P < 0.001), and the proportion with Zung SAS scores indicating mild, moderate, or severe anxiety (vs no anxiety) decreased from 50% to 17% (χ 2 = 33.03, P < 0.001). |
| Gómez-Gil, 2012 [45] Cross-sectional | Women and men | HT (120)c vs No HT (67)c | HADS (anxiety subscale) SADS | Mean: 11.0 years (women, range, 1-46 years); 4.7 years (men, range, 1-22 years) | Mean HADS and SADS scores were lower in the group receiving HT vs the group not receiving HT (6.4 ± 3.7 vs 9.0 ± 4.0, P = 0.001; 8.5 ± 7.8 vs 11.0 ± 7.3, P = 0.038, respectively).d The proportion with scores indicating anxiety (vs no anxiety) was higher in the group not receiving HT (χ 2 = 14.46, P < 0.001).d |
| de Vries, 2011 [34] Prospective cohort | Girls and boys | GnRH treatment (41) | STAI (trait subscale) | 1.88 years | Mean anxiety score did not change. |
| de Vries, 2014 [35] Prospective cohorta,b | Girls and boys | GnRH treatment + HT (32)c | STAI (trait subscale) | 5.9 years | Mean anxiety score did not change. |
| López de Lara, 2020 [38] Prospective cohortb | Girls and boys | GnRH treatment + HT (23) | STAI (trait subscale) | 1 year | Mean anxiety score decreased from 33.0 ± 7.2 to 18.5 ± 8.4 (P < 0.001). |
Abbreviations: BAI, Beck Anxiety Inventory; DSM, Diagnostic and Statistical Manual of Mental Disorders; GAS, gender-affirming surgery; GnRH, gonadotropin-releasing hormone; HADS, Hospital Anxiety and Depression Scale; HT, hormone therapy; IQR, interquartile range; SADS, Social Avoidance and Distress Scale; SCL-90-R, Symptom Checklist 90-Revised; STAI, State-Trait Anxiety Inventory; Zung SAS, Zung Self-Rating Anxiety Scale.
aAll participants were also included in de Vries (2011) [34]
bIncluded a cisgender control group or a comparison to general population norms
cIncluded participants who have undergone gender-affirming surgery/surgeries, or surgery status not reported
dAdjusted for age, gender, and education level
Effects of Gender-Affirming Hormone Therapy on Anxiety Among Transgender People
| Author, year | Transgender population | Treatment / comparison (n) | Anxiety measures | Length of treatment | Findings |
|---|---|---|---|---|---|
| Fuss, 2015 [37] Prospective cohort | Women | HT (20)c | Ad hoc questionnaire | 12 months | Anxiety score did not change from a median of 0.0 at baseline. |
| Defreyne, 2018 [33] Prospective cohort | Women | HT (91)c | HADS (anxiety subscale) | 1 year | Median anxiety score did not change. |
| Defreyne, 2018 [33] Prospective cohort | Men | HT (64)c | HADS (anxiety subscale) | 1 year | Median anxiety score did not change. |
| Motta, 2018 [41] Prospective cohort | Men | HT (46)c | DSM | 7 months | Proportion diagnosed with an anxiety disorder (6/46, 12%) did not change. |
| Turan, 2018 [42] Prospective cohortb | Men | HT (37) | SCL-90-R (anxiety subscale) | 24 weeks | Mean anxiety score did not change. |
| Colizzi, 2014 [31] Prospective cohort | Women and men | HT (107) | SCL-90-R (anxiety subscale) Zung SAS | 12 months | Mean SCL-90-R score decreased from 1.05 ± 0.95 to 0.54 ± 0.56 (P < 0.001), which represents an improvement from borderline anxiety disorder to no anxiety disorder. Mean Zung SAS score improved from 44.91 ± 9.59 to 37.90 ± 8.97 (P < 0.001), and the proportion with Zung SAS scores indicating mild, moderate, or severe anxiety (vs no anxiety) decreased from 50% to 17% (χ 2 = 33.03, P < 0.001). |
| Gómez-Gil, 2012 [45] Cross-sectional | Women and men | HT (120)c vs No HT (67)c | HADS (anxiety subscale) SADS | Mean: 11.0 years (women, range, 1-46 years); 4.7 years (men, range, 1-22 years) | Mean HADS and SADS scores were lower in the group receiving HT vs the group not receiving HT (6.4 ± 3.7 vs 9.0 ± 4.0, P = 0.001; 8.5 ± 7.8 vs 11.0 ± 7.3, P = 0.038, respectively).d The proportion with scores indicating anxiety (vs no anxiety) was higher in the group not receiving HT (χ 2 = 14.46, P < 0.001).d |
| de Vries, 2011 [34] Prospective cohort | Girls and boys | GnRH treatment (41) | STAI (trait subscale) | 1.88 years | Mean anxiety score did not change. |
| de Vries, 2014 [35] Prospective cohorta,b | Girls and boys | GnRH treatment + HT (32)c | STAI (trait subscale) | 5.9 years | Mean anxiety score did not change. |
| López de Lara, 2020 [38] Prospective cohortb | Girls and boys | GnRH treatment + HT (23) | STAI (trait subscale) | 1 year | Mean anxiety score decreased from 33.0 ± 7.2 to 18.5 ± 8.4 (P < 0.001). |
| Author, year | Transgender population | Treatment / comparison (n) | Anxiety measures | Length of treatment | Findings |
|---|---|---|---|---|---|
| Fuss, 2015 [37] Prospective cohort | Women | HT (20)c | Ad hoc questionnaire | 12 months | Anxiety score did not change from a median of 0.0 at baseline. |
| Defreyne, 2018 [33] Prospective cohort | Women | HT (91)c | HADS (anxiety subscale) | 1 year | Median anxiety score did not change. |
| Defreyne, 2018 [33] Prospective cohort | Men | HT (64)c | HADS (anxiety subscale) | 1 year | Median anxiety score did not change. |
| Motta, 2018 [41] Prospective cohort | Men | HT (46)c | DSM | 7 months | Proportion diagnosed with an anxiety disorder (6/46, 12%) did not change. |
| Turan, 2018 [42] Prospective cohortb | Men | HT (37) | SCL-90-R (anxiety subscale) | 24 weeks | Mean anxiety score did not change. |
| Colizzi, 2014 [31] Prospective cohort | Women and men | HT (107) | SCL-90-R (anxiety subscale) Zung SAS | 12 months | Mean SCL-90-R score decreased from 1.05 ± 0.95 to 0.54 ± 0.56 (P < 0.001), which represents an improvement from borderline anxiety disorder to no anxiety disorder. Mean Zung SAS score improved from 44.91 ± 9.59 to 37.90 ± 8.97 (P < 0.001), and the proportion with Zung SAS scores indicating mild, moderate, or severe anxiety (vs no anxiety) decreased from 50% to 17% (χ 2 = 33.03, P < 0.001). |
| Gómez-Gil, 2012 [45] Cross-sectional | Women and men | HT (120)c vs No HT (67)c | HADS (anxiety subscale) SADS | Mean: 11.0 years (women, range, 1-46 years); 4.7 years (men, range, 1-22 years) | Mean HADS and SADS scores were lower in the group receiving HT vs the group not receiving HT (6.4 ± 3.7 vs 9.0 ± 4.0, P = 0.001; 8.5 ± 7.8 vs 11.0 ± 7.3, P = 0.038, respectively).d The proportion with scores indicating anxiety (vs no anxiety) was higher in the group not receiving HT (χ 2 = 14.46, P < 0.001).d |
| de Vries, 2011 [34] Prospective cohort | Girls and boys | GnRH treatment (41) | STAI (trait subscale) | 1.88 years | Mean anxiety score did not change. |
| de Vries, 2014 [35] Prospective cohorta,b | Girls and boys | GnRH treatment + HT (32)c | STAI (trait subscale) | 5.9 years | Mean anxiety score did not change. |
| López de Lara, 2020 [38] Prospective cohortb | Girls and boys | GnRH treatment + HT (23) | STAI (trait subscale) | 1 year | Mean anxiety score decreased from 33.0 ± 7.2 to 18.5 ± 8.4 (P < 0.001). |
Abbreviations: BAI, Beck Anxiety Inventory; DSM, Diagnostic and Statistical Manual of Mental Disorders; GAS, gender-affirming surgery; GnRH, gonadotropin-releasing hormone; HADS, Hospital Anxiety and Depression Scale; HT, hormone therapy; IQR, interquartile range; SADS, Social Avoidance and Distress Scale; SCL-90-R, Symptom Checklist 90-Revised; STAI, State-Trait Anxiety Inventory; Zung SAS, Zung Self-Rating Anxiety Scale.
aAll participants were also included in de Vries (2011) [34]
bIncluded a cisgender control group or a comparison to general population norms
cIncluded participants who have undergone gender-affirming surgery/surgeries, or surgery status not reported
dAdjusted for age, gender, and education level
Death by Suicide
One retrospective study reported in 2 publications assessed death by suicide (Table 5) [43, 44]. The first publication reported that 3 transgender women in the Amsterdam gender dysphoria study cohort (n = 303) died by suicide between 1972 and 1986 [43]. The authors calculated the number of suicide deaths expected in an age-matched stratum of the general male Dutch population over this period to be 0.208. No data were reported for transgender men (n = 122). An update to this study reported 17 deaths by suicide among transgender women (n = 966) and 1 among transgender men (n = 365) between 1975 and 2007 [44]. The age- and sex-stratified standardized mortality ratios were 5.70 (95% CI: 4.93, 6.54) and 2.22 (95% CI: 0.53, 6.18), respectively. The risk of bias for this study was serious due to the difficulty of identifying appropriate comparison groups and uncontrolled confounding by surgery status and socioeconomic variables such as unemployment. We cannot draw any conclusions on the basis of this single study about whether hormone therapy affects death by suicide among transgender people.
Effects of Gender-Affirming Hormone Therapy on Death by Suicide Among Transgender People
| Author, year | Transgender population | Treatment / comparison (n) | Measures | Length of treatment | Findings |
|---|---|---|---|---|---|
| Asscheman, 1989 [43] Retrospective cohorta,b | Women | HT (303)c | Death by suicide (confirmed by autopsy report) | Median: 4.4 years (range, 6 months to 13 years) | 3 transgender women (1%) died by suicide between 1972 and 1986. The adjusted number of suicide deaths expected among the general Dutch male population was 0.208. |
| Asscheman, 2011 [44] Retrospective cohorta,b | Women | HT (966)c | Death by suicide (confirmed by medical report or physician information) | Median: 18.6 years (range, 0.7–44.5 years) | 17 transgender women (2%) died by suicide between 1975 and 2007. The age-stratified SMR compared to the general Dutch male population was 5.70 (95% CI: 4.93, 6.54). |
| Asscheman, 1989 [43] Retrospective cohorta,b | Men | HT (122)c | Death by suicide (confirmation procedure NR) | Median: 3.6 years (range, 6 months to 13 years) | No deaths by suicide among transgender men were reported during the study period. |
| Asscheman, 2011 [44] Retrospective cohorta,b | Men | HT (365)c | Death by suicide (confirmed by medical report or physician information) | Median: 18.4 years (range, 4.7–42.6 years) | 1 transgender man (0.3%) died by suicide between 1975 and 2007. The age-stratified SMR compared to the general Dutch female population was 2.22 (95% CI: 0.53, 6.18). |
| Author, year | Transgender population | Treatment / comparison (n) | Measures | Length of treatment | Findings |
|---|---|---|---|---|---|
| Asscheman, 1989 [43] Retrospective cohorta,b | Women | HT (303)c | Death by suicide (confirmed by autopsy report) | Median: 4.4 years (range, 6 months to 13 years) | 3 transgender women (1%) died by suicide between 1972 and 1986. The adjusted number of suicide deaths expected among the general Dutch male population was 0.208. |
| Asscheman, 2011 [44] Retrospective cohorta,b | Women | HT (966)c | Death by suicide (confirmed by medical report or physician information) | Median: 18.6 years (range, 0.7–44.5 years) | 17 transgender women (2%) died by suicide between 1975 and 2007. The age-stratified SMR compared to the general Dutch male population was 5.70 (95% CI: 4.93, 6.54). |
| Asscheman, 1989 [43] Retrospective cohorta,b | Men | HT (122)c | Death by suicide (confirmation procedure NR) | Median: 3.6 years (range, 6 months to 13 years) | No deaths by suicide among transgender men were reported during the study period. |
| Asscheman, 2011 [44] Retrospective cohorta,b | Men | HT (365)c | Death by suicide (confirmed by medical report or physician information) | Median: 18.4 years (range, 4.7–42.6 years) | 1 transgender man (0.3%) died by suicide between 1975 and 2007. The age-stratified SMR compared to the general Dutch female population was 2.22 (95% CI: 0.53, 6.18). |
Abbreviations: HT, hormone therapy; NR, not reported; SMR, standardized mortality ratio.
aAn unknown number of participants were included in both Asscheman (1989) [43] and Asscheman (2011) [44]
bIncluded a cisgender control group or a comparison to general population norms
cIncludes participants who had undergone gender-affirming surgery/surgeries, or surgery status not reported
Effects of Gender-Affirming Hormone Therapy on Death by Suicide Among Transgender People
| Author, year | Transgender population | Treatment / comparison (n) | Measures | Length of treatment | Findings |
|---|---|---|---|---|---|
| Asscheman, 1989 [43] Retrospective cohorta,b | Women | HT (303)c | Death by suicide (confirmed by autopsy report) | Median: 4.4 years (range, 6 months to 13 years) | 3 transgender women (1%) died by suicide between 1972 and 1986. The adjusted number of suicide deaths expected among the general Dutch male population was 0.208. |
| Asscheman, 2011 [44] Retrospective cohorta,b | Women | HT (966)c | Death by suicide (confirmed by medical report or physician information) | Median: 18.6 years (range, 0.7–44.5 years) | 17 transgender women (2%) died by suicide between 1975 and 2007. The age-stratified SMR compared to the general Dutch male population was 5.70 (95% CI: 4.93, 6.54). |
| Asscheman, 1989 [43] Retrospective cohorta,b | Men | HT (122)c | Death by suicide (confirmation procedure NR) | Median: 3.6 years (range, 6 months to 13 years) | No deaths by suicide among transgender men were reported during the study period. |
| Asscheman, 2011 [44] Retrospective cohorta,b | Men | HT (365)c | Death by suicide (confirmed by medical report or physician information) | Median: 18.4 years (range, 4.7–42.6 years) | 1 transgender man (0.3%) died by suicide between 1975 and 2007. The age-stratified SMR compared to the general Dutch female population was 2.22 (95% CI: 0.53, 6.18). |
| Author, year | Transgender population | Treatment / comparison (n) | Measures | Length of treatment | Findings |
|---|---|---|---|---|---|
| Asscheman, 1989 [43] Retrospective cohorta,b | Women | HT (303)c | Death by suicide (confirmed by autopsy report) | Median: 4.4 years (range, 6 months to 13 years) | 3 transgender women (1%) died by suicide between 1972 and 1986. The adjusted number of suicide deaths expected among the general Dutch male population was 0.208. |
| Asscheman, 2011 [44] Retrospective cohorta,b | Women | HT (966)c | Death by suicide (confirmed by medical report or physician information) | Median: 18.6 years (range, 0.7–44.5 years) | 17 transgender women (2%) died by suicide between 1975 and 2007. The age-stratified SMR compared to the general Dutch male population was 5.70 (95% CI: 4.93, 6.54). |
| Asscheman, 1989 [43] Retrospective cohorta,b | Men | HT (122)c | Death by suicide (confirmation procedure NR) | Median: 3.6 years (range, 6 months to 13 years) | No deaths by suicide among transgender men were reported during the study period. |
| Asscheman, 2011 [44] Retrospective cohorta,b | Men | HT (365)c | Death by suicide (confirmed by medical report or physician information) | Median: 18.4 years (range, 4.7–42.6 years) | 1 transgender man (0.3%) died by suicide between 1975 and 2007. The age-stratified SMR compared to the general Dutch female population was 2.22 (95% CI: 0.53, 6.18). |
Abbreviations: HT, hormone therapy; NR, not reported; SMR, standardized mortality ratio.
aAn unknown number of participants were included in both Asscheman (1989) [43] and Asscheman (2011) [44]
bIncluded a cisgender control group or a comparison to general population norms
cIncludes participants who had undergone gender-affirming surgery/surgeries, or surgery status not reported
Discussion
This systematic review of 20 studies found evidence that gender-affirming hormone therapy may be associated with improvements in QOL scores and decreases in depression and anxiety symptoms among transgender people. Associations were similar across gender identity and age. The strength of evidence for these conclusions is low due to methodological limitations (Table 6). It was impossible to draw conclusions about the effects of hormone therapy on death by suicide.
Strength of Evidence of Studies that Evaluate the Psychological Effects of Hormone Therapy Among Transgender People
| Outcome | Number of studies (n) | Strength of evidence | Summarya |
|---|---|---|---|
| Quality of life | 1 randomized controlled trial [27] (45)b 2 before-after trials [28, 29] (65)b 2 prospective cohorts [30, 39] (133) 2 cross-sectional studies [46, 48] (108) | Lowe | Hormone therapy may improve quality of life among transgender people.g |
| Depression | 1 before-after trial [28] (40) 9 prospective cohorts [30-36, 38, 40, 42] (569)c 2 cross-sectional [45, 47] (228) | Lowe | Hormone therapy may alleviate depression among transgender people.g |
| Anxiety | 7 prospective cohorts [31, 33-35, 37, 38, 41, 42] (464)c 1 cross-sectional [45] (187) | Lowe | Hormone therapy may alleviate anxiety among transgender people.g |
| Death by suicide | 1 retrospective cohort [43, 44] (1756)d | Insufficientf | There is insufficient evidence to draw a conclusion about the effect of hormone therapy on death by suicide among transgender people. |
| Outcome | Number of studies (n) | Strength of evidence | Summarya |
|---|---|---|---|
| Quality of life | 1 randomized controlled trial [27] (45)b 2 before-after trials [28, 29] (65)b 2 prospective cohorts [30, 39] (133) 2 cross-sectional studies [46, 48] (108) | Lowe | Hormone therapy may improve quality of life among transgender people.g |
| Depression | 1 before-after trial [28] (40) 9 prospective cohorts [30-36, 38, 40, 42] (569)c 2 cross-sectional [45, 47] (228) | Lowe | Hormone therapy may alleviate depression among transgender people.g |
| Anxiety | 7 prospective cohorts [31, 33-35, 37, 38, 41, 42] (464)c 1 cross-sectional [45] (187) | Lowe | Hormone therapy may alleviate anxiety among transgender people.g |
| Death by suicide | 1 retrospective cohort [43, 44] (1756)d | Insufficientf | There is insufficient evidence to draw a conclusion about the effect of hormone therapy on death by suicide among transgender people. |
aDue to similarity of findings, the summary is the same for transgender men and transgender women and for adolescents and adults
cAll 55 participants in de Vries (2014) [35] were also included among the 70 participants in de Vries (2011) [34] and are counted once
dAn unknown number of participants were included in both Asscheman (1989) [43] and Asscheman (2011), [44] so the unique sample size is smaller than indicated here
eEvidence downgraded due to study limitations, including uncontrolled confounding, and imprecision because of small sample sizes
fEvidence downgraded due to study limitations, including confounding and a lack of meaningful comparison groups, and imprecision in measurement of a rare event
gThe body of cross-sectional evidence tended to align with the conclusion
Strength of Evidence of Studies that Evaluate the Psychological Effects of Hormone Therapy Among Transgender People
| Outcome | Number of studies (n) | Strength of evidence | Summarya |
|---|---|---|---|
| Quality of life | 1 randomized controlled trial [27] (45)b 2 before-after trials [28, 29] (65)b 2 prospective cohorts [30, 39] (133) 2 cross-sectional studies [46, 48] (108) | Lowe | Hormone therapy may improve quality of life among transgender people.g |
| Depression | 1 before-after trial [28] (40) 9 prospective cohorts [30-36, 38, 40, 42] (569)c 2 cross-sectional [45, 47] (228) | Lowe | Hormone therapy may alleviate depression among transgender people.g |
| Anxiety | 7 prospective cohorts [31, 33-35, 37, 38, 41, 42] (464)c 1 cross-sectional [45] (187) | Lowe | Hormone therapy may alleviate anxiety among transgender people.g |
| Death by suicide | 1 retrospective cohort [43, 44] (1756)d | Insufficientf | There is insufficient evidence to draw a conclusion about the effect of hormone therapy on death by suicide among transgender people. |
| Outcome | Number of studies (n) | Strength of evidence | Summarya |
|---|---|---|---|
| Quality of life | 1 randomized controlled trial [27] (45)b 2 before-after trials [28, 29] (65)b 2 prospective cohorts [30, 39] (133) 2 cross-sectional studies [46, 48] (108) | Lowe | Hormone therapy may improve quality of life among transgender people.g |
| Depression | 1 before-after trial [28] (40) 9 prospective cohorts [30-36, 38, 40, 42] (569)c 2 cross-sectional [45, 47] (228) | Lowe | Hormone therapy may alleviate depression among transgender people.g |
| Anxiety | 7 prospective cohorts [31, 33-35, 37, 38, 41, 42] (464)c 1 cross-sectional [45] (187) | Lowe | Hormone therapy may alleviate anxiety among transgender people.g |
| Death by suicide | 1 retrospective cohort [43, 44] (1756)d | Insufficientf | There is insufficient evidence to draw a conclusion about the effect of hormone therapy on death by suicide among transgender people. |
aDue to similarity of findings, the summary is the same for transgender men and transgender women and for adolescents and adults
cAll 55 participants in de Vries (2014) [35] were also included among the 70 participants in de Vries (2011) [34] and are counted once
dAn unknown number of participants were included in both Asscheman (1989) [43] and Asscheman (2011), [44] so the unique sample size is smaller than indicated here
eEvidence downgraded due to study limitations, including uncontrolled confounding, and imprecision because of small sample sizes
fEvidence downgraded due to study limitations, including confounding and a lack of meaningful comparison groups, and imprecision in measurement of a rare event
gThe body of cross-sectional evidence tended to align with the conclusion
Uncontrolled confounding was a major limitation in this literature. Many studies simultaneously assessed different types of gender-affirming care and did not control for gender-affirming surgery status, making it difficult to isolate the effects of hormone therapy. Others failed to report complete information about surgery status. Additional factors that may influence both access to care and psychological outcomes, including extent of social or legal gender affirmation and exposure to determinants of health such as discrimination, were typically not considered. In addition, some evidence indicates that cyproterone acetate, a common anti-androgen assessed in many studies alongside estrogen therapy, may increase depression, which may be a source of confounding [49].
Another source of potential bias was recruitment of participants from specialized clinics that impose strict diagnostic criteria as a prerequisite for gender-affirming care. The dual role of clinicians and researchers as both gatekeepers and investigators may force transgender study participants to over- or understate aspects of their mental health in order to access gender-affirming care [8]. Similarly, transgender clinic patients may feel that they cannot opt out of research-related activities, which is a serious concern for the validity of psychological outcome measurements.
Clinic-based recruitment also overlooks transgender people who cannot access these clinics for financial or other reasons and misses those whose need for gender affirmation does not fit into current medical models. This is a particular concern for nonbinary and other gender-diverse people, for whom a model of gender affirmation as a linear transition from one binary gender to another is inaccurate [50].
Most studies used well-known scales for measuring psychological outcomes. None of these scales, however, have been specifically validated for use in transgender populations [51]. Furthermore, many scales are normed separately for (presumed cisgender) men and women [52]. Inconsistency in identification of appropriate general population norms hinders comparisons between transgender and cisgender groups, which is a major related research question that requires further investigation.
Beyond methodological concerns in the studies we assessed, our review has other limitations. First, it is likely subject to publication bias, as we may have missed studies not published in the peer-reviewed literature. Second, a number of potentially relevant studies could not be included because the authors did not report on a minimum of 3 months of treatment or did not clearly state the type and/or duration of therapy, including the range for cross-sectional studies [53-65]. Finally, even where outcome measurements were similar across studies, heterogeneity in study designs, study populations, intervention characteristics, and reporting of results (ie, some studies reported results separately by gender identity, while others did not), prevented us from quantitatively pooling results.
More research is needed to further explore the relationship between gender-affirming hormone therapy and QOL, death by suicide, and other psychological outcomes, especially among adolescents. Future studies should investigate these outcomes in larger groups of diverse participants recruited outside clinical settings. Studies assessing the relationship between gender-affirming hormone therapy and mental health outcomes in transgender populations should be prospective or use strong quasi-experimental designs; consistently report type, dose, and duration of hormone therapy; adjust for possible confounding by gender-affirming surgery status; control for other variables that may independently influence psychological outcomes; and report results separately by gender identity. Despite the limitations of the available evidence, however, our review indicates that gender-affirming hormone therapy is likely associated with improvements in QOL, depression, and anxiety. No studies showed that hormone therapy harms mental health or quality of life among transgender people. These benefits make hormone therapy an essential component of care that promotes the health and well-being of transgender people.
Abbreviations
- BDI
Beck Depression Inventory
- ENIGI
European Network for the Investigation of Gender Incongruence
- GnRH
gonadotropin-releasing hormone
- HADS
Hospital Anxiety and Depression Scale
- QOL
quality of life
- RCT
randomized controlled trial
- SF-36
Short Form-36 Health Survey
- WPATH
World Professional Association for Transgender Health
Acknowledgments
Financial Support: This review was partly funded by the World Professional Association for Transgender Health.
Author Contributions: R.S. developed and implemented the search strategy with input from K.B., L.W., and K.R. K.B., L.W., R.S., V.D., K.M., and K.R. screened and assessed studies, extracted data, and graded strength of evidence. K.B. wrote the report, which was reviewed by all co-authors.
Additional Information
Disclosure Summary: This review was partially funded by the World Professional Association for Transgender Health (WPATH). The authors of this manuscript are responsible for its content. Statements in the manuscript do not necessarily reflect the official views of or imply endorsement by WPATH.
Data Availability
Some or all data generated or analyzed during this study are included in this published article or in the data repository listed in the References.

{kind=link}