





Abstract
Evidence has shown that Hepatitis E virus (HEV) genotype 3 is autochthonous in industrialized countries due to zoonotic transmission through direct contact or consumption of raw or undercooked meat from domestic swine or wild boar. As there is lack of data on seroprevalence of HEV in the general Portuguese population, a wide survey was conducted as part of the HEPeCONTROL project (60DT2), under EEA grants funding.
Sera from a representative sample of the Portuguese population (n = 1656) at different geographic locations (30 territorial units), and age (0–99 years) were collected between July 2015 and February 2016. The sera were tested for the presence of anti-HEV IgG and IgM by EIA using one of the two most commonly used commercial immunoassays in Europe.
The overall HEV IgG seroprevalence was found to be 16.3% increasing with age (P < 0.05) from 0.6% in the 0–9 years group to 30.1% in people older than 70 years. The seroprevalence also varied geographically with generally higher seropositivities (25–30%) in the most rural areas of Portugal. However, the geographical differences were not statistically significant (P > 0.05). Out of 1656 samples, 8 were positive for anti-HEV IgM indicating current of recent HEV infection but no significant differences were found concerning age groups, regions and sex.
The present nation-wide survey provides insight in the epidemiology of HEV in Portugal and confirms that HEV is endemic in the Portuguese population.
Introduction
Hepatitis E virus (HEV) is today widely recognized as a serious public health issue in industrialized countries.1,2 Infection by HEV was in the past mistakenly considered rare and restricted to travellers returning from endemic developing countries.3 Over the past decades published data has definitely refuted that concept. It is now known that infection by HEV genotype 3 is autochthonous in Europe and of zoonotic origin, with swine as the main reservoir. Direct contact with pigs, as well as consumption of undercooked pork meat and sausages are the most important routes of transmission.3–6 In Europe, human HEV genotype 3 infections are often subclinical or asymptomatic, but a range of human illness associated to this genotype has been reported, including fulminant liver failure or chronic liver disease, as well as extra-hepatic manifestations.3,7,8 Epidemiological studies in several European countries have reported highly different HEV seroprevalences (ranging from 0.6% to 52.5%) between and within countries.9 Besides geographical differences, this wide range of seroprevalences has also been linked to other variables, including age and risk of exposure, but mostly the imunoassays used in the studies.9–11
In Portugal, only a few relatively small studies on the seroepidemiology of HEV have taken place.12 In order to provide a clearer understanding of HEV epidemiology in Portugal, we evaluated the presence of anti-HEV antibodies in the sera of a representative selection of the Portuguese population. Risk factors for HEV infection were also determined by studying the HEV seropositivity related to demographic characteristics, namely age, sex and region.
Methods
Ethics approval
This study was approved by a regional ethics commission (Comissão de Ética para a Saúde do Centro Hospitalar de São João; Reference number: 99/2015) and the participants provided informed consent.
Study population
The sample size was calculated according to previously described methods.12 Briefly, a sample size of 1656 was calculated assuming an a priori 50% anti-HEV seroprevalence (yielding the highest possible sample size), a confidence in the estimate of 95%, a maximum allowable error in the prevalence of 3%, and a Portuguese population size of Portugal of 10 541 840 (based on the latest Portuguese census data).13
A stratified random sampling design with all 30 NUTS III regions (Nomenclature of Territorial Units for Statistics; level III) of Portugal as a stratification level was set up in order to provide a representative sample. On the basis of the census data, the stratified distribution in each regional stratum was proportionally sampled by 10 age group (0–9, 10–19, 20–29, 30–39, 40–49, 50–59, 60–69, 70+) and by gender.13 Sera were collected between July 2015 and February 2016 from attendees (or their legal representatives) of Clinical Analysis Laboratories from all NUTS III regions. Attendees were randomly selected based on the required age group and gender until the necessary number of samples was reached in each region. This process provided an accurate representation of the target population in our sample by region, 10-year age groups and gender.
Serological analysis
For the detection of anti-HEV IgG and anti-HEV IgM antibodies in sera the Mikrogen commercial enzyme immunoassays recomWell HEV IgG and recomWell HEV IgM (versions 2015, Mikrogen, Germany) were used and samples were considered positive according to the manufacturer’s instructions.
Statistical analysis
Sex and regional differences in prevalence were evaluated by Chi-square. Age group differences were evaluated by Chi-square for trend analysis. A P-values < 0.05 was considered significant. All statistical analyses were performed using the Statistical Software Package SPSS 20.0 (SPSS Inc., Chicago, IL).
Results
Descriptive analysis of the sampled population (n = 1656) is given in table 1. The sample included a similar number of males and females, 813 (49.1%) and 843 (50.9%), respectively (male : female ratio of 1 : 1.03). Serum samples were obtained from all age groups being the youngest participant 3 months-old and the eldest 99-years-old. The 70+ year group was the stratum with the highest number of individuals (17.9%), while the 0–9 year group included the lowest number (9.9%). Concerning geographical distribution, Lisbon was the region with highest number of individuals included (13.6%) and the region with lowest was Pinhal Interior Sul (1.9%).
Descriptive statistics, anti-HEV IgG and anti-HEV IgM seropositivity according to sex, age groups and region (30 NUTS III regions)
| Variables | No. of samples (%) | HEV IgG positives no (%) | P | HEV IgM positives no. (%) |
|---|---|---|---|---|
| Total | 1656 (100%) | 270 (16.30%) | 8 (0.48%) | |
| Sex | ||||
| Male | 813 (49.1%) | 119 (14.6%) | P > 0.05* | 4 (0.5%) |
| Female | 843 (50.9%) | 151 (17.9%) | 4 (0.5%) | |
| Age group | ||||
| 0–9 | 164 (9.9%) | 1 (0.6%) | P < 0.05** | 0 (0%) |
| 10–19 | 177 (10.7%) | 3 (1.7%) | 0 (0%) | |
| 20–29 | 184 (11.1%) | 5 (2.7%) | 0 (0%) | |
| 30–39 | 225 (13.6%) | 29 (12.9%) | 1 (0.4%) | |
| 40–49 | 220 (13.3%) | 42 (19.1%) | 3 (1.4%) | |
| 50–59 | 206 (12.4%) | 53 (25.7%) | 1 (0.5%) | |
| 60–69 | 184 (11.1%) | 48 (26.1%) | 0 (0%) | |
| 70+ | 296 (17.9%) | 89 (30.1%) | 3 (1.0%) | |
| Region | ||||
| Açores | 40 (2.4%) | 4 (10.0%) | P > 0.05* | 0 (0%) |
| Alentejo Central | 36 (2.2%) | 6 (16.7%) | 1 (2.8%) | |
| Alentejo Litoral | 36 (2.2%) | 3 (8.3%) | 0 (0%) | |
| Algarve | 67 (4.0%) | 8 (11.9%) | 0 (0%) | |
| Alto Alentejo | 36 (2.2%) | 8 (22.2%) | 1 (2.8%) | |
| Alto Trás-os-Montes | 35 (2.1%) | 4 (11.4%) | 1 (2.9%) | |
| Ave | 69 (4.2%) | 11 (15.9%) | 0 (0%) | |
| Baixo Alentejo | 36 (2.2%) | 5 (13.9%) | 0 (0%) | |
| Baixo Mondego | 53 (3.2%) | 11 (20.8%) | 0 (0%) | |
| Baixo Vouga | 66 (4.0%) | 11 (16.7%) | 0 (0%) | |
| Beira Interior Norte | 35 (2.1%) | 9 (25.7%) | 1 (2.9%) | |
| Beira Interior Sul | 35 (2.1%) | 7 (20.0%) | 0 (0%) | |
| Cávado | 61 (3.7%) | 15 (24.6%) | 0 (0%) | |
| Cova da Beira | 35 (2.1%) | 8 (22.9%) | 0 (0%) | |
| Dão-Lafões | 37 (2.2%) | 3 (8.1%) | 0 (0%) | |
| Douro | 36 (2.2%) | 10 (27.8%) | 0 (0%) | |
| Entre Douro e Vouga | 42 (2.5%) | 5 (11.9%) | 0 (0%) | |
| Grande Porto | 149 (9.0%) | 27 (18.1%) | 0 (0%) | |
| Lezíria do Tejo | 36 (2.2%) | 4 (11.1%) | 1 (2.8%) | |
| Lisbon | 226 (13.6%) | 41 (18.1%) | 0 (0%) | |
| Madeira | 44 (2.7%) | 4 (9.1%) | 0 (0%) | |
| Médio Tejo | 34 (2.1%) | 4 (11.8%) | 0 (0%) | |
| Minho-Lima | 37 (2.2%) | 4 (10.8%) | 0 (0%) | |
| Oeste | 54 (3.3%) | 8 (14.8%) | 0 (0%) | |
| Península de Setúbal | 100 (6.0%) | 14 (14.0%) | 0 (0%) | |
| Pinhal Interior Norte | 40 (2.4%) | 5 (12.5%) | 0 (0%) | |
| Pinhal Interior Sul | 32 (1.9%) | 5 (15.6%) | 0 (0%) | |
| Pinhal Litoral | 38 (2.3%) | 4 (10.5%) | 0 (0%) | |
| Serra da Estrela | 36 (2.2%) | 7 (19.4%) | 1 (2.8%) | |
| Tâmega | 75 (4.5%) | 15 (20.0%) | 2 (2.7%) |
| Variables | No. of samples (%) | HEV IgG positives no (%) | P | HEV IgM positives no. (%) |
|---|---|---|---|---|
| Total | 1656 (100%) | 270 (16.30%) | 8 (0.48%) | |
| Sex | ||||
| Male | 813 (49.1%) | 119 (14.6%) | P > 0.05* | 4 (0.5%) |
| Female | 843 (50.9%) | 151 (17.9%) | 4 (0.5%) | |
| Age group | ||||
| 0–9 | 164 (9.9%) | 1 (0.6%) | P < 0.05** | 0 (0%) |
| 10–19 | 177 (10.7%) | 3 (1.7%) | 0 (0%) | |
| 20–29 | 184 (11.1%) | 5 (2.7%) | 0 (0%) | |
| 30–39 | 225 (13.6%) | 29 (12.9%) | 1 (0.4%) | |
| 40–49 | 220 (13.3%) | 42 (19.1%) | 3 (1.4%) | |
| 50–59 | 206 (12.4%) | 53 (25.7%) | 1 (0.5%) | |
| 60–69 | 184 (11.1%) | 48 (26.1%) | 0 (0%) | |
| 70+ | 296 (17.9%) | 89 (30.1%) | 3 (1.0%) | |
| Region | ||||
| Açores | 40 (2.4%) | 4 (10.0%) | P > 0.05* | 0 (0%) |
| Alentejo Central | 36 (2.2%) | 6 (16.7%) | 1 (2.8%) | |
| Alentejo Litoral | 36 (2.2%) | 3 (8.3%) | 0 (0%) | |
| Algarve | 67 (4.0%) | 8 (11.9%) | 0 (0%) | |
| Alto Alentejo | 36 (2.2%) | 8 (22.2%) | 1 (2.8%) | |
| Alto Trás-os-Montes | 35 (2.1%) | 4 (11.4%) | 1 (2.9%) | |
| Ave | 69 (4.2%) | 11 (15.9%) | 0 (0%) | |
| Baixo Alentejo | 36 (2.2%) | 5 (13.9%) | 0 (0%) | |
| Baixo Mondego | 53 (3.2%) | 11 (20.8%) | 0 (0%) | |
| Baixo Vouga | 66 (4.0%) | 11 (16.7%) | 0 (0%) | |
| Beira Interior Norte | 35 (2.1%) | 9 (25.7%) | 1 (2.9%) | |
| Beira Interior Sul | 35 (2.1%) | 7 (20.0%) | 0 (0%) | |
| Cávado | 61 (3.7%) | 15 (24.6%) | 0 (0%) | |
| Cova da Beira | 35 (2.1%) | 8 (22.9%) | 0 (0%) | |
| Dão-Lafões | 37 (2.2%) | 3 (8.1%) | 0 (0%) | |
| Douro | 36 (2.2%) | 10 (27.8%) | 0 (0%) | |
| Entre Douro e Vouga | 42 (2.5%) | 5 (11.9%) | 0 (0%) | |
| Grande Porto | 149 (9.0%) | 27 (18.1%) | 0 (0%) | |
| Lezíria do Tejo | 36 (2.2%) | 4 (11.1%) | 1 (2.8%) | |
| Lisbon | 226 (13.6%) | 41 (18.1%) | 0 (0%) | |
| Madeira | 44 (2.7%) | 4 (9.1%) | 0 (0%) | |
| Médio Tejo | 34 (2.1%) | 4 (11.8%) | 0 (0%) | |
| Minho-Lima | 37 (2.2%) | 4 (10.8%) | 0 (0%) | |
| Oeste | 54 (3.3%) | 8 (14.8%) | 0 (0%) | |
| Península de Setúbal | 100 (6.0%) | 14 (14.0%) | 0 (0%) | |
| Pinhal Interior Norte | 40 (2.4%) | 5 (12.5%) | 0 (0%) | |
| Pinhal Interior Sul | 32 (1.9%) | 5 (15.6%) | 0 (0%) | |
| Pinhal Litoral | 38 (2.3%) | 4 (10.5%) | 0 (0%) | |
| Serra da Estrela | 36 (2.2%) | 7 (19.4%) | 1 (2.8%) | |
| Tâmega | 75 (4.5%) | 15 (20.0%) | 2 (2.7%) |
Chi square.
Chi square for trend.
Descriptive statistics, anti-HEV IgG and anti-HEV IgM seropositivity according to sex, age groups and region (30 NUTS III regions)
| Variables | No. of samples (%) | HEV IgG positives no (%) | P | HEV IgM positives no. (%) |
|---|---|---|---|---|
| Total | 1656 (100%) | 270 (16.30%) | 8 (0.48%) | |
| Sex | ||||
| Male | 813 (49.1%) | 119 (14.6%) | P > 0.05* | 4 (0.5%) |
| Female | 843 (50.9%) | 151 (17.9%) | 4 (0.5%) | |
| Age group | ||||
| 0–9 | 164 (9.9%) | 1 (0.6%) | P < 0.05** | 0 (0%) |
| 10–19 | 177 (10.7%) | 3 (1.7%) | 0 (0%) | |
| 20–29 | 184 (11.1%) | 5 (2.7%) | 0 (0%) | |
| 30–39 | 225 (13.6%) | 29 (12.9%) | 1 (0.4%) | |
| 40–49 | 220 (13.3%) | 42 (19.1%) | 3 (1.4%) | |
| 50–59 | 206 (12.4%) | 53 (25.7%) | 1 (0.5%) | |
| 60–69 | 184 (11.1%) | 48 (26.1%) | 0 (0%) | |
| 70+ | 296 (17.9%) | 89 (30.1%) | 3 (1.0%) | |
| Region | ||||
| Açores | 40 (2.4%) | 4 (10.0%) | P > 0.05* | 0 (0%) |
| Alentejo Central | 36 (2.2%) | 6 (16.7%) | 1 (2.8%) | |
| Alentejo Litoral | 36 (2.2%) | 3 (8.3%) | 0 (0%) | |
| Algarve | 67 (4.0%) | 8 (11.9%) | 0 (0%) | |
| Alto Alentejo | 36 (2.2%) | 8 (22.2%) | 1 (2.8%) | |
| Alto Trás-os-Montes | 35 (2.1%) | 4 (11.4%) | 1 (2.9%) | |
| Ave | 69 (4.2%) | 11 (15.9%) | 0 (0%) | |
| Baixo Alentejo | 36 (2.2%) | 5 (13.9%) | 0 (0%) | |
| Baixo Mondego | 53 (3.2%) | 11 (20.8%) | 0 (0%) | |
| Baixo Vouga | 66 (4.0%) | 11 (16.7%) | 0 (0%) | |
| Beira Interior Norte | 35 (2.1%) | 9 (25.7%) | 1 (2.9%) | |
| Beira Interior Sul | 35 (2.1%) | 7 (20.0%) | 0 (0%) | |
| Cávado | 61 (3.7%) | 15 (24.6%) | 0 (0%) | |
| Cova da Beira | 35 (2.1%) | 8 (22.9%) | 0 (0%) | |
| Dão-Lafões | 37 (2.2%) | 3 (8.1%) | 0 (0%) | |
| Douro | 36 (2.2%) | 10 (27.8%) | 0 (0%) | |
| Entre Douro e Vouga | 42 (2.5%) | 5 (11.9%) | 0 (0%) | |
| Grande Porto | 149 (9.0%) | 27 (18.1%) | 0 (0%) | |
| Lezíria do Tejo | 36 (2.2%) | 4 (11.1%) | 1 (2.8%) | |
| Lisbon | 226 (13.6%) | 41 (18.1%) | 0 (0%) | |
| Madeira | 44 (2.7%) | 4 (9.1%) | 0 (0%) | |
| Médio Tejo | 34 (2.1%) | 4 (11.8%) | 0 (0%) | |
| Minho-Lima | 37 (2.2%) | 4 (10.8%) | 0 (0%) | |
| Oeste | 54 (3.3%) | 8 (14.8%) | 0 (0%) | |
| Península de Setúbal | 100 (6.0%) | 14 (14.0%) | 0 (0%) | |
| Pinhal Interior Norte | 40 (2.4%) | 5 (12.5%) | 0 (0%) | |
| Pinhal Interior Sul | 32 (1.9%) | 5 (15.6%) | 0 (0%) | |
| Pinhal Litoral | 38 (2.3%) | 4 (10.5%) | 0 (0%) | |
| Serra da Estrela | 36 (2.2%) | 7 (19.4%) | 1 (2.8%) | |
| Tâmega | 75 (4.5%) | 15 (20.0%) | 2 (2.7%) |
| Variables | No. of samples (%) | HEV IgG positives no (%) | P | HEV IgM positives no. (%) |
|---|---|---|---|---|
| Total | 1656 (100%) | 270 (16.30%) | 8 (0.48%) | |
| Sex | ||||
| Male | 813 (49.1%) | 119 (14.6%) | P > 0.05* | 4 (0.5%) |
| Female | 843 (50.9%) | 151 (17.9%) | 4 (0.5%) | |
| Age group | ||||
| 0–9 | 164 (9.9%) | 1 (0.6%) | P < 0.05** | 0 (0%) |
| 10–19 | 177 (10.7%) | 3 (1.7%) | 0 (0%) | |
| 20–29 | 184 (11.1%) | 5 (2.7%) | 0 (0%) | |
| 30–39 | 225 (13.6%) | 29 (12.9%) | 1 (0.4%) | |
| 40–49 | 220 (13.3%) | 42 (19.1%) | 3 (1.4%) | |
| 50–59 | 206 (12.4%) | 53 (25.7%) | 1 (0.5%) | |
| 60–69 | 184 (11.1%) | 48 (26.1%) | 0 (0%) | |
| 70+ | 296 (17.9%) | 89 (30.1%) | 3 (1.0%) | |
| Region | ||||
| Açores | 40 (2.4%) | 4 (10.0%) | P > 0.05* | 0 (0%) |
| Alentejo Central | 36 (2.2%) | 6 (16.7%) | 1 (2.8%) | |
| Alentejo Litoral | 36 (2.2%) | 3 (8.3%) | 0 (0%) | |
| Algarve | 67 (4.0%) | 8 (11.9%) | 0 (0%) | |
| Alto Alentejo | 36 (2.2%) | 8 (22.2%) | 1 (2.8%) | |
| Alto Trás-os-Montes | 35 (2.1%) | 4 (11.4%) | 1 (2.9%) | |
| Ave | 69 (4.2%) | 11 (15.9%) | 0 (0%) | |
| Baixo Alentejo | 36 (2.2%) | 5 (13.9%) | 0 (0%) | |
| Baixo Mondego | 53 (3.2%) | 11 (20.8%) | 0 (0%) | |
| Baixo Vouga | 66 (4.0%) | 11 (16.7%) | 0 (0%) | |
| Beira Interior Norte | 35 (2.1%) | 9 (25.7%) | 1 (2.9%) | |
| Beira Interior Sul | 35 (2.1%) | 7 (20.0%) | 0 (0%) | |
| Cávado | 61 (3.7%) | 15 (24.6%) | 0 (0%) | |
| Cova da Beira | 35 (2.1%) | 8 (22.9%) | 0 (0%) | |
| Dão-Lafões | 37 (2.2%) | 3 (8.1%) | 0 (0%) | |
| Douro | 36 (2.2%) | 10 (27.8%) | 0 (0%) | |
| Entre Douro e Vouga | 42 (2.5%) | 5 (11.9%) | 0 (0%) | |
| Grande Porto | 149 (9.0%) | 27 (18.1%) | 0 (0%) | |
| Lezíria do Tejo | 36 (2.2%) | 4 (11.1%) | 1 (2.8%) | |
| Lisbon | 226 (13.6%) | 41 (18.1%) | 0 (0%) | |
| Madeira | 44 (2.7%) | 4 (9.1%) | 0 (0%) | |
| Médio Tejo | 34 (2.1%) | 4 (11.8%) | 0 (0%) | |
| Minho-Lima | 37 (2.2%) | 4 (10.8%) | 0 (0%) | |
| Oeste | 54 (3.3%) | 8 (14.8%) | 0 (0%) | |
| Península de Setúbal | 100 (6.0%) | 14 (14.0%) | 0 (0%) | |
| Pinhal Interior Norte | 40 (2.4%) | 5 (12.5%) | 0 (0%) | |
| Pinhal Interior Sul | 32 (1.9%) | 5 (15.6%) | 0 (0%) | |
| Pinhal Litoral | 38 (2.3%) | 4 (10.5%) | 0 (0%) | |
| Serra da Estrela | 36 (2.2%) | 7 (19.4%) | 1 (2.8%) | |
| Tâmega | 75 (4.5%) | 15 (20.0%) | 2 (2.7%) |
Chi square.
Chi square for trend.
Of the 1656 serum samples studied, 270 tested positive for anti-HEV IgG giving an overall anti-HEV IgG seroprevalence of 16.3% (95% confidence interval: 14.6–18.2) (table 1).
No differences (P = 0.593) in anti-HEV IgG seropositivity were observed between genders with females presenting 17.9% and males 14.6% (table 1). When analyzing age, a significant increase (P < 0.05) of anti-HEV IgG seroprevalence was detected, from the minimum of 0.6% in the 0–9 years age group to the maximum of 30.1% in the 70+ years age group (table 1, figure 1). No significant differences (P > 0.05) in anti-HEV IgG seropositivity were found by gender within each age group.
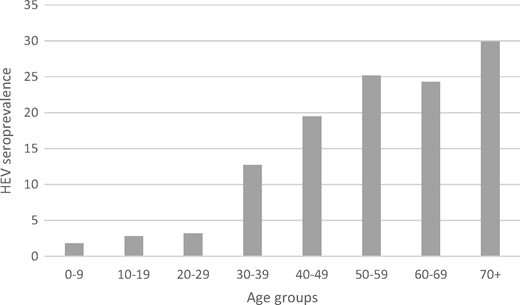
Estimated prevalence of anti-HEV IgG antibodies in Portugal by age groups
The HEV seroprevalence in different regions of Portugal varied from the minimum of 8.1% in Dão-Lafões to 27.8% in Douro (figure 2), but the regional differences were not statistically significant (P > 0.05). The most cosmopolitan regions in Portugal, Lisbon and Grande Porto (NUTS III) had similar anti-HEV IgG seroprevalences of 18.1% (table 1), whereas the most rural NUTS III regions (in the centre of Portugal and in the north to the border of Spain) were the ones presenting higher (25–30%) anti-HEV IgG seroprevalences (figure 2).
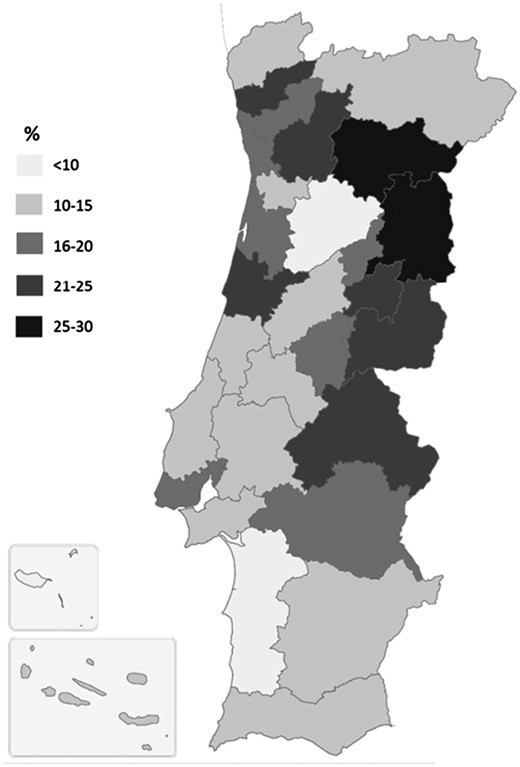
Anti-HEV IgG seroprevalence by region of Portugal (30 NUTS III regions)
All the 1656 serum samples were also tested for anti-HEV IgM. Antibodies were found in 8 individuals, 4 females and 4 males (table 1) indicating current or recent HEV infection. Therefore, the overall anti-HEV IgM seroprevalence was 0.48% (95% confidence interval: 0.3–1.0).
Discussion
The present study is the first large-scale HEV seroprevalence study performed in Portugal. It aimed at clarifying the HEV seroepidemiology in Portugal by analysis of anti-HEV antibodies in sera of a representative selection of the Portuguese population, collected according to gender, age group and regions of Portugal as stratification levels. Unlike most seroprevalence studies in Europe, with sampling of adult blood donors, the present study also included more rarely targeted age groups, namely the very young (0–18-years-old) and individuals above 65 years of age. It hence provides additional value to the study and a broader picture of HEV seroepidemiology across the Portuguese population.
The results indicate an overall anti-HEV IgG seroprevalence of 16.3% in the Portuguese population. Data from Europe report seroprevalences ranging from 0.6% to 52.5%9, however, it is now-a-days well recognized that the prevalence is highly influenced by the geographical location and by the commercial serological assays, which vary considerably in their sensitivity and specificity.14,15 For these reasons, results should be interpreted with caution. In fact, albeit we screened sera with one of the two most commonly used commercial anti-HEV assays in Europe,9 the Mikrogen assay, it has been widely reported that this assay produces discordant results when compared to the other most commonly used, the Wantai assay.9,14,15 In general, seroprevalence studies performed with Mikrogen assay produce lower rates than Wantai.9,14,15 When we compare our results with country data from other European studies that used the Mikrogen assay, it was interesting to find that the Portuguese seroprevalence was similar to others found in Germany, namely 14.5%,16 16.8%,17 18%18 and 17.9%.19
It was interesting to find that the seroprevalence in the Portuguese population was substantial (16.3%), comparing with the fairly low number of autochthonous hepatitis E cases that have been reported so far.8,20 In fact, most cases of HEV genotype 3 are asymptomatic and the symptomatic ones are not usually recognized because the rate of icteric illness is low and severe hepatitis is rare.3
However, the high circulation of HEV genotype3 in both domestic pigs6 and wild boar21 in Portugal can help explain the substantial seroprevalence in the Portuguese population, which has a strong tradition of pork consumption. Moreover, we previously reported that 32% of fatteners group of pigs of Portugal (the ones close to slaughter age and about to enter the food chain for consumption) were excreting HEV in stools.6
In the present study, an increase of anti-HEV IgG seroprevalence with age (P < 0.05) was observed, reaching the maximum of 30% in the eldest. A similar increase has been reported by others3 and is expected by the longer period of exposure to risk factors, cumulatively occurring during the life-time exposure. Accordingly, the youngest age group (0–9-years-old) was also the one with the lowest anti-HEV IgG seroprevalence (0.6%), which is in line with a recent study in Germany suggesting that only a very small number of HEV infections occur in children.22 Similar anti-HEV IgG seropositivity (∼1%) has been also found in recently collected sera from Portuguese children aging 0–4-years-old.23 However, the anti-HEV IgG seroprevalence in these youngest groups must be interpreted with caution since they can include infants in which the presence of maternal antibodies cannot be excluded. In fact, an efficient transplacental transport of anti-HEV IgG has been previously demonstrated by us.24
On the other hand, no significant difference was found in anti-HEV IgG seroprevalence according to gender, which seems to be the case for HEV infections throughout Europe.9
Concerning geographic distribution, no significant difference was observed regarding HEV seroprevalence, although a generally higher seropositivity was found in the most rural areas of Portugal (25–30%), the regions with the highest concentration of pigs.25 As pigs are the main reservoir for HEV, this probably explains the high seropositivity in these regions. Further, the lower seropositivity in the archipelagos of Madeira (9%) and Azores (10%) is consistent with the lowest concentration of pigs.25
Regarding anti-HEV IgM seroprevalence it was not possible to identify statistically significant differences in seropositivity regarding age, gender or region.
In summary, an overall seroprevalence of 16.3% was found in this study, the first nationwide study in Portugal. Moreover, this study provides insight in the HEV infection of the Portuguese general population and generates information on risk profiles regarding demographic data.
Acknowledgements
The present study was supported by European Economic Area Grants (EEA grants) 2009–14, Public Health Inititativeś Programme (PT06) and project HEPeCONTROL (60DT2). The authors would like to acknowledge Laboratório de Análises Clínicas Dr Aires Raposo & Dra Teresinha Raposo Lda, Laboratório de Análises Clínicas S. Lázaro, Laboratório de Análises Clínicas Flaviano Gusmão, Gnóstica—Laboratório de Análises Clínicas, EUROMEDIC–Castelo Branco, Laboratório Manuel Pimenta, Labeto—Centro de Análises Bioquímicas, S.A. (Grupo Beatriz Godinho), Laboratório de Análises Clínicas José Manuel Chau, S.A. (Grupo Beatriz Godinho), Seialab–Laboratório de Análises Clínicas de Seia, S.A. (Grupo Beatriz Godinho), Laboratório de Análises Clínicas Vale do Sousa, Avelab–Laboratório Médico de Análises Clínicas, Laboratório de Análises Clínicas Dra. Albina Marinho, Laboratório de Análises Clínicas Dr. Ferraz Alves, Laboratório de Análises Clínicas Dr. Castro Fernandes, Clídis–Clínica de Diagnósticos de Sines, Laboratório de Análises Clínicas Joaquim J Nunes Oliveira & C S.A., Laboratório de Análises Clínicas Dr. J. Leitão Santos Lda, Laboratório de Análises Clínicas Bernardina Sancho, for the valuable collaboration on sample collection. The authors would like to acknowledge all participants of the study. During the course of the HEPeCONTROL project partial results have been presented as oral communications at the 19th Annual Meeting of the European Society for Clinical Virology, September 2016, Lisbon, Portugal; the International Liver Congress 2016 April 2016, Barcelona, Spain and the 14° Encontro Nacional Actualização Infecciologia, Porto, Portugal, 2015.
The present study is included in HEPeCONTROL Project (60DT2), granted by the Public Health Initiatives Programme (PT06) financed by EEA Grants Financial Mechanism.
Funding
This study was supported by the EEA Grants 20092014, Programme Public Health Initiatives.
Conflicts of interest: None declared.
An overall anti-HEV IgG seroprevalence of 16.3% was found in the Portuguese population.
This HEV seroprevalence increase with age reaching a maximum (30%) in the eldest.
No significant differences in HEV seroprevalence were found between genders and regions of Portugal.
The 16.3% HEV seroprevalence is not in accordance with the low number of reported hepatitis E cases in the country, possibly due to the lack of attention to autochthonous hepatitis E.

{kind=link}
{kind=link}
Comments