





Abstract
PRKAG2-mutated cardiomyopathies are a rare non-sarcomeric hypertrophic cardiomyopathy, caused by pathological accumulation of glycogen within cardiomyocytes.
The most common electrophysiological alterations associated with this cardiomyopathy are atrial fibrillation (AF) and high degree AV block, including total atrioventricular block.
Furthermore, is known a strong correlation between these cardiomyopathies and the presence of accessory pathways with decremental conduction Mahaim-like.
We present the case of a 58-year-old male patient admitted to our CCU for atrial fibrillation complicated with complete atrioventricular block symptomatic for dyspnea.
In addiction the EKG showed ventricular preexcitation beats, at first mistaken for ventricular escape beats, with positive low amplitude Delta wave in D1-AVL, discordant in the lower leads and negative in V1-V2. (Figure 1)
The cardiac MRI exhibited a significant asymmetric hypertrophy of the interventricular septum (19mm), no LGE, ejection fraction preserved.
During the electrophysiological study (post electrical cardioversion) a severe conduction disturbance was found with AH 250 ms, HV 100 ms.
During isoprenaline infusion 2 gamma/min, an atrial extrasystole causes slatentification of conduction on accessory pathway (AH 190 ms, HV 30 ms) with decremental properties in septal position (assessed by multisite stimulation) and sensitive to adenosine (12 mg).
During ajmaline 20 mg infusion a selective blockage of the accessory pathway was detected, confirming the suspicion of accessory fasciculus-ventricular pathway.
At the end of electrophysiological study septal endomyocardial biopsy (EMB) guided by CARTO 3 v 7.5 mapping system was performed aimed for detection of pathological glycogen accumulations in cardiomyocytes.
Finally, a two-chamber pacemaker was implanted and genetic survey (currently underway) was performed with a genetic screening panel for hypertrophic cardiomyopathy including PRKAG2 mutations.
The electrophysiological study showed a significant supra-hisian and infra-hisian conduction disorder, associated with the presence of a septal fascicolo-ventricular accessory pathway.
EMB confirmed several areas of pathologically rich glycogen cardiomyocytes (Figure 2)
In patients with hypertrophic phenotype cardiomyopathy and presence of ventricular preexcitation by decremental conduction pathways is critical to suspect cardiomyopathy by PRKAG2 mutation.
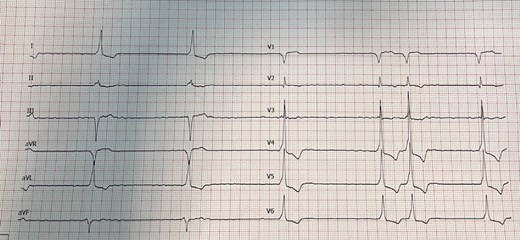
AF complicated with complete AV block, in addiction wide QRS with low amplitude delta wave.
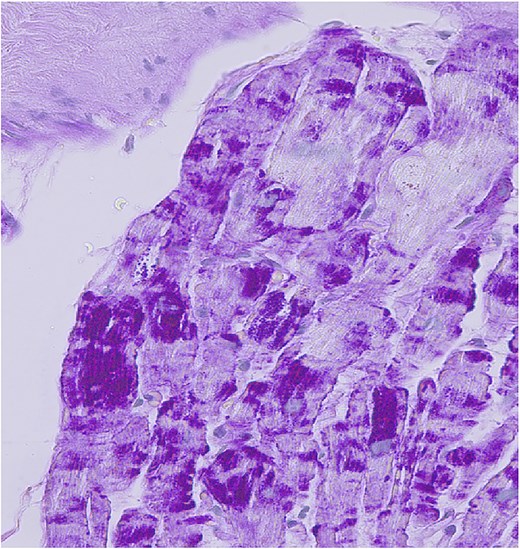
x40. Zonal pathological glycogen accumulation in myocardiocytes detected by periodic acid-Schiff (PAS) staining.

{kind=link}