





Abstract
Despite the well-established role of CRT in heart failure, major limitations of CRT are an occasional incidence of unsuccessful coronary sinus (CS) lead placement, one third non-responders in conventional CRT patients and higher complications risk in CRT upgrade procedures. The WiSE® Wireless Stimulation Endocardial) CRT System is designed to overcome these limitations. Prior non-randomised studies with the WiSE® CRT System have shown high implant success rates and improvement in LV remodeling and heart failure symptoms.
Pivotal study to assess the safety and effectiveness of the WiSE® CRT System in an international, randomized, two-arm, double blinded, prospective study (randomized part only).
99 Patients with indication for CRT and previously failed CRT implant, considered as high-risk upgrade to conventional CRT, or non-responders to conventional CRT underwent device implantation and were then randomised into treatment (47 pts, System ON) and control (52 pts System OFF) groups for 6 months. Primary efficacy endpoints were change in LVESV, LVEDV, LVEF and QRS over 6 months in blinded Echo and ECG core lab analysis.
Mean ΔLVESV (%) -14.6 (-19.6, -9.6); mean ΔLVEDV (%) -8.1 (-11.9, -4.3) and mean ΔQRS (ms) -41.9 (-50.1, -33.7) in the treatment group were significantly lower/shorter than mean ΔLVESV (%) -5.2 (-10.7, 0.2); mean ΔLVEDV (%) -3.0 (-7.0, 1.0) and mean ΔQRS (ms) -1.7 (-7.1,3.8) in the control group, p=0.005; p=0.027 and p=0.001, 95% CI. Mean ΔLVEF (%) 5.4 (3.2, 7.7) in the treatment group increased significantly compared to control group ΔLVEF (%) 2.4 (0.2, 4.5), p=0.048. 8 of 99 pts were attempted from WiSE CRT implant.
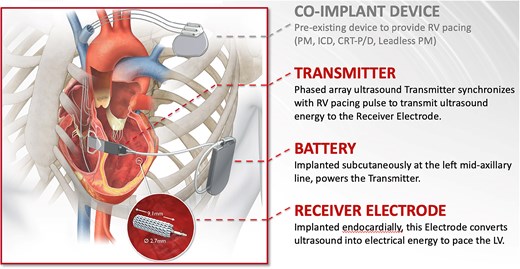
WISE® CRT System
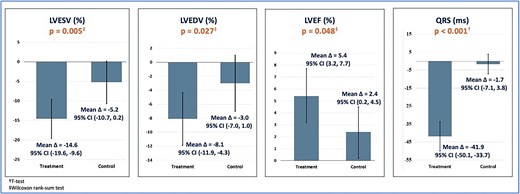
Efficacy entire randomised population

{kind=link}