




Cover image
Diagnosis of malignant coronary vasospasm by 12-lead Holter electrocardiogram and optical coherence tomography
Sarah Bär1†, Tilman Perrin2†, Lorenz Räber1, and Tobias Reichlin1*
1Department of Cardiology, Swiss Cardiovascular Center, Inselspital, University Hospital Bern, University of Bern, 3010 Bern, Switzerland; and 2Department of Cardiology, Bürgerspital Solothurn, 4500 Solothurn, Switzerland
* Corresponding author. Tel: 141 31 664 00 50, Email: [email protected]
†Sarah Bär and Tilman Perrin authors contributed equally to this article.
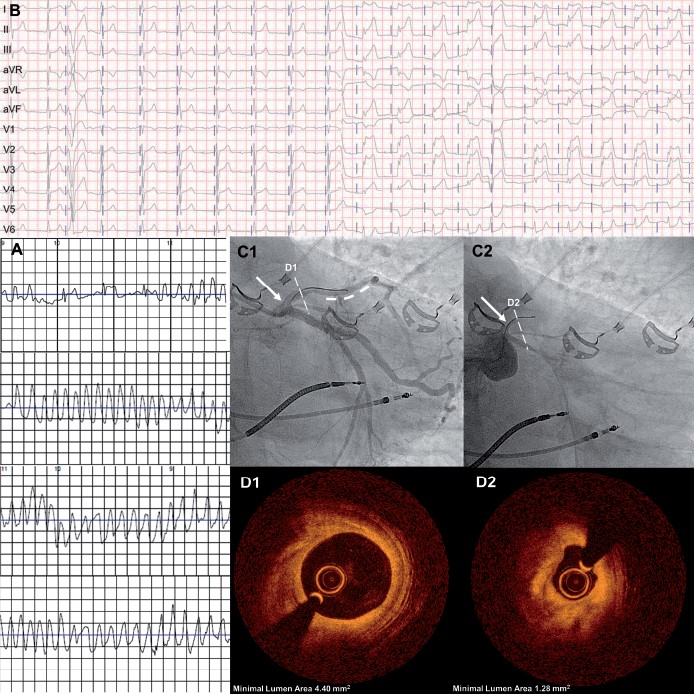
A 73-year-old man presented with recurrent syncopes preceded by angina. Three years earlier, the patient had a pacemaker implanted due to symptomatic sick sinus syndrome. Device interrogation showed several torsade-like ventricular tachycardias (VTs) corresponding with the symptoms. Left ventricular ejection fraction was normal. Coronary angiography revealed diffuse coronary sclerosis and a hazy 50% lesion in the mid left anterior descending artery (LAD), which was treated with a drug-eluting stent. Three days later, the patient experienced another syncope with documentation of ventricular fibrillation by the provided life-vest (Panel A). The pacemaker was upgraded to an implantable cardioverter-defibrillator. During subsequent workup, a 12-lead Holter electrocardiogram (ECG) revealed intermittent giant ST-segment elevations in the anterior and inferior leads (Panel B) with concurrent angina. Repeat coronary angiography showed a good result of the LAD stent (Panel C1, bold dashed line) and normal minimal lumen area of LAD by optical coherence tomography (OCT) (Panel D1). Intracoronary application of 50 µg methergin triggered subtotal left main coronary artery vasospasm (Panel C2) with global ST-segment elevations, severe hypotension and non-sustained VT. The beginning of the spasm was documented by OCT showing a thickening of the media with consecutive lumen narrowing (Panel D2). The vasospasm was reverted by application of sublingual isosorbiddinitrat and intra-coronary nitroglycerine. Repeat testing thereafter was uneventful. A treatment with amlodipine and molsidomine was introduced before discharge. The patient remained symptom-free for 3 months and a 12-lead Holter ECG showed no further ST-segment changes. According to our case, both 12-lead Holter ECG and coronary vasospasm testing should be considered during workup of patients with angina without significant coronary artery disease.
Volume 40, Issue 41, 1 November 2019
Focus Issue on Chronic Coronary Syndromes
Issue @ a Glance
Chronic coronary syndromes: genetics, shear stress, and biomarkers
CardioPulse
ESC CardioMed – A Reference Resource that is always up-to-date: An ESC cardiovascular information resource that is continuously updated for the cardiology community
ESC Textbook of Cardiovascular Medicine wins award: The ESC Textbook wins first prize from the 2019 British Medical Association Medical Book Award in the Cardiology Category
European Society of Cardiology Advocacy: Promoting cardiovascular disease on decision-makers agenda
THEMIS and THEMIS-PCI: New Option for Antiplatelet Therapy in Patients with Stable Atherosclerosis and Diabetes: Key Findings from THEMIS and THEMIS-PCI
Willem Einthoven and the ECG: Antoni Bayés de Luna discusses the discovery of the ECG almost 120 years ago which has remained almost unchanged to the present day
Congress showcases the latest echocardiography developments: The latest developments in echocardiography and potential applications for the future will be highlighted at the 20th International Congress on Advances in Cardiac Ultrasound March 2020
Clinical Research
Coronary artery disease
Genetic variation at the coronary artery disease risk locus GUCY1A3 modifies cardiovascular disease prevention effects of aspirin

Editorial
Variability in aspirin efficacy: all in the genes?
Coronary artery disease
Implications of N-terminal pro-B-type natriuretic peptide in patients with three-vessel disease

Editorial
Quantifying heart failure using natriuretic peptides may help the HEART team in decision-making
Coronary artery disease
A randomized controlled trial of metformin on left ventricular hypertrophy in patients with coronary artery disease without diabetes: the MET-REMODEL trial

Editorial
Regression therapy for cardiovascular disease

Current Opinion
Coronary artery disease
Expert recommendations on the assessment of wall shear stress in human coronary arteries: existing methodologies, technical considerations, and clinical applications


