





Patients with atrial fibrillation (AF) have a high risk of stroke and mortality, which can be considerably reduced by oral anticoagulants (OAC). Recently, four non-vitamin-K oral anticoagulants (NOACs) were compared with warfarin in large randomized trials for the prevention of stroke and systemic embolism. Today's clinician is faced with the difficult task of selecting a suitable OAC for a patient with a particular clinical profile or a particular pattern of risk factors and concomitant diseases. We reviewed analyses of subgroups of patients from trials of vitamin K antagonists vs. NOACs for stroke prevention in AF with the aim to identify patient groups who might benefit from a particular OAC more than from another. In the first of a two-part review, we discuss the choice of NOAC for stroke prevention in the following subgroups of patients with AF: (i) stable coronary artery disease or peripheral artery disease, including percutaneous coronary intervention with stenting and triple therapy; (ii) cardioversion, ablation and anti-arrhythmic drug therapy; (iii) mechanical valves and rheumatic valve disease, (iv) patients with time in therapeutic range of >70% on warfarin; (v) patients with a single stroke risk factor (CHA2DS2VASc score of 1 in males, 2 in females); and (vi) patients with a single first episode of paroxysmal AF. Although there are no major differences in terms of efficacy and safety between the NOACs for some clinical scenarios, in others we are able to suggest that particular drugs and/or doses be prioritized for anticoagulation.
Introduction
Patients with atrial fibrillation (AF) have a high risk of stroke, which can be considerably reduced by oral anticoagulants (OACs). Large randomized phase III trials have compared five non-vitamin-K oral anticoagulants (NOACs) with warfarin for prevention of stroke and systemic embolism.1–4 Dabigatran was evaluated at two different doses in the RE-LY trial.1 Two NOACs were evaluated using one dose, with protocol-mandated dose adaptations: rivaroxaban in the ROCKET AF study2 and apixaban in the ARISTOTLE trial.3 Edoxaban was evaluated at two doses, each with dose adaptation, in the ENGAGE AF-TIMI 48 trial4 (Table 1). Apixaban has also been compared with aspirin in patients unable or unwilling to take a vitamin K antagonist (VKA).5 The first agent to be studied, ximelagatran, was taken off the market due to hepatic toxicity.6–8 No direct head-to-head comparisons have been reported for the four available NOACs, and it is therefore difficult for the practising physician to choose between different drugs and different doses.
Doses of the different NOACs in the four large comparative trials in AF patients
| NOAC | Dose |
|---|---|
| Dabigatran (RELY) | 150 mg twice daily 110 mg twice daily |
| Rivaroxaban (ROCKAT-AF) | 20 mg once daily, protocol-mandated dose reduction to15 mg |
| Apixaban (ARISTOTLE) | 5 mg twice daily, protocol-mandated dose reduction to 2.5 mg |
| Edoxaban (ENGAGE-AF) | 60 mg once daily, protocol-mandated dose reduction to 30 mg 30 mg once daily, protocol-mandated dose reduction to15 mg |
| NOAC | Dose |
|---|---|
| Dabigatran (RELY) | 150 mg twice daily 110 mg twice daily |
| Rivaroxaban (ROCKAT-AF) | 20 mg once daily, protocol-mandated dose reduction to15 mg |
| Apixaban (ARISTOTLE) | 5 mg twice daily, protocol-mandated dose reduction to 2.5 mg |
| Edoxaban (ENGAGE-AF) | 60 mg once daily, protocol-mandated dose reduction to 30 mg 30 mg once daily, protocol-mandated dose reduction to15 mg |
Study acronyms in brackets.
Doses of the different NOACs in the four large comparative trials in AF patients
| NOAC | Dose |
|---|---|
| Dabigatran (RELY) | 150 mg twice daily 110 mg twice daily |
| Rivaroxaban (ROCKAT-AF) | 20 mg once daily, protocol-mandated dose reduction to15 mg |
| Apixaban (ARISTOTLE) | 5 mg twice daily, protocol-mandated dose reduction to 2.5 mg |
| Edoxaban (ENGAGE-AF) | 60 mg once daily, protocol-mandated dose reduction to 30 mg 30 mg once daily, protocol-mandated dose reduction to15 mg |
| NOAC | Dose |
|---|---|
| Dabigatran (RELY) | 150 mg twice daily 110 mg twice daily |
| Rivaroxaban (ROCKAT-AF) | 20 mg once daily, protocol-mandated dose reduction to15 mg |
| Apixaban (ARISTOTLE) | 5 mg twice daily, protocol-mandated dose reduction to 2.5 mg |
| Edoxaban (ENGAGE-AF) | 60 mg once daily, protocol-mandated dose reduction to 30 mg 30 mg once daily, protocol-mandated dose reduction to15 mg |
Study acronyms in brackets.
In this two-part consensus document, we review the results of analyses for particular subgroups of patients from the five main trials and propose that the use of particular drugs or doses be prioritized for particular patients on the basis of these sub-analyses. In part 1, we discuss patients which are usually seen by cardiologists. This review does not compete with the European Heart Rhythm Association (EHRA) practical guide recommendations9 or other evidence-based clinical practice guidelines.
Patients with stable coronary artery disease
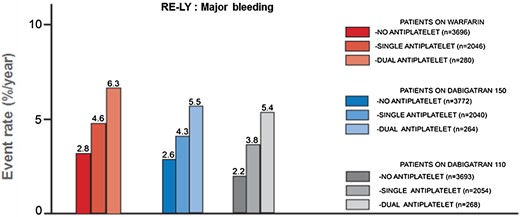
Post hoc analysis from the RE-LY trial: Dabigatran (low dose: grey bars; high dose: blue bars) and warfarin (red bars) have been analysed with regard to the occurrence of major-bleeding complications, stratified according to single OAC administration (light colour), combination therapy with one antiplatelet agent (middle-intensity colour), and together with dual antiplatelet therapy (high-intensity colour). Adapted from Dans et al.10
There is good evidence for the utility of chronic VKA therapy in patients with stable CAD, whereas NOACs have been less well investigated in such patients. Nevertheless, in pre-specified subgroup analyses reported in the primary publications from the four main NOAC trials, patients with both AF and CAD had very few acute coronary events across all study arms (<1.5%/year), including those randomized to warfarin who received VKA monotherapy, and patients in the NOAC arms who received NOAC monotherapy. Clearly, this finding, based on subgroup analyses, represents relatively weak evidence, and more definite conclusions about the optimal drug choice for patients with stable CAD would require prospective trials adequately powered with respect to this particular population.
There is no clear preference for any of the currently available NOACs over VKA for patients with both AF and CAD. A joint European consensus document endorsed by the Heart Rhythm Society and Asia-Pacific Heart Rhythm Society refutes the concern that dabigatran may increase the risk of acute myocardial infarction.11 Moreover, the large FDA Medicare analysis found no evidence of an increased risk of myocardial infarction in patients taking dabigatran compared with warfarin.12
Based on our interpretation of available data, we suggest
| First choice | Monotherapy with an NOAC is preferable for patients with AF and stable CAD. This suggestion is applicable to all NOACs |
| Second choice | In selected patients, addition of aspirin is still indicated in the long-term, based on individual risk assessment and coronary anatomy |
| Comment | In the absence of direct comparative studies, no particular NOAC can be favoured over another |
| First choice | Monotherapy with an NOAC is preferable for patients with AF and stable CAD. This suggestion is applicable to all NOACs |
| Second choice | In selected patients, addition of aspirin is still indicated in the long-term, based on individual risk assessment and coronary anatomy |
| Comment | In the absence of direct comparative studies, no particular NOAC can be favoured over another |
| First choice | Monotherapy with an NOAC is preferable for patients with AF and stable CAD. This suggestion is applicable to all NOACs |
| Second choice | In selected patients, addition of aspirin is still indicated in the long-term, based on individual risk assessment and coronary anatomy |
| Comment | In the absence of direct comparative studies, no particular NOAC can be favoured over another |
| First choice | Monotherapy with an NOAC is preferable for patients with AF and stable CAD. This suggestion is applicable to all NOACs |
| Second choice | In selected patients, addition of aspirin is still indicated in the long-term, based on individual risk assessment and coronary anatomy |
| Comment | In the absence of direct comparative studies, no particular NOAC can be favoured over another |
Patients with stable peripheral artery disease
Only limited data are available on the use of NOACs as antithrombotic therapy in patients with peripheral artery disease (PAD). Patients with PAD in ROCKET AF (5.9%) did not have a significantly higher risk of stroke or systemic embolism than did patients without PAD, and outcomes in patients treated with rivaroxaban and warfarin paralleled those in the trial as a whole. There was a significant interaction for major or non-major clinically relevant bleeding in patients with PAD treated with rivaroxaban compared with warfarin (hazard ratio, HR: 1.40, 95% confidence interval, CI: 1.06–1.86) and those without PAD (HR: 1.03, 95% CI: 0.95–1.11; interaction P = 0.037).13 Randomized trials of edoxaban and rivaroxaban in patients with PAD are currently underway.14
Based on our interpretation of available data we suggest:
| First choice | Until new evidence emerges, drug choice for antithrombotic therapy in patients with AF and PAD is the same as in those with AF and stable CAD |
| First choice | Until new evidence emerges, drug choice for antithrombotic therapy in patients with AF and PAD is the same as in those with AF and stable CAD |
| First choice | Until new evidence emerges, drug choice for antithrombotic therapy in patients with AF and PAD is the same as in those with AF and stable CAD |
| First choice | Until new evidence emerges, drug choice for antithrombotic therapy in patients with AF and PAD is the same as in those with AF and stable CAD |
Patients undergoing percutaneous coronary intervention and stenting
Patients with AF and an acute coronary syndrome or stable CAD may require percutaneous coronary intervention with stenting. In these patients, the need for OAC treatment to prevent stroke and for dual antiplatelet therapy to prevent stent thrombosis must be balanced against the increased risk of bleeding (particularly intracranial haemorrhage) with dual or triple antithrombotic therapy.
The use of VKAs in this setting has been the subject of observational studies and one completed randomized trial,15 and is currently under investigation in comparison with NOACs in additional trials. All phase III trials of NOACs allowed the concomitant use of aspirin (≤100 mg/day) for patients undergoing percutaneous coronary interventions, but only the RE-LY trial included a substantial number of patients on concomitant clopidogrel with or without aspirin.10 Ongoing trials will provide additional data for NOACs or warfarin in combination with aspirin and/or P2Y12 inhibitors (clopidogrel, prasugrel, or ticagrelor) (REDUAL-PCI for dabigatran NCT02164864, PIONEER-AF-PCI for rivaroxaban NCT01830543, AUGUSTUS for apixaban NCT02415400).
Management of these patients was recently addressed in the joint European consensus document.11 The document suggested a period of triple therapy (OAC plus aspirin plus clopidogrel), followed by a period of dual therapy (OAC plus single antiplatelet agent, preferably clopidogrel). Once the patient is stable, after 1 year, an OAC alone can be given. When an OAC is prescribed, this can be either controlled VKA therapy [time in therapeutic range (TTR) of >70%; preferred international normalized ratio (INR) range 2.0–2.5] or an NOAC. When an NOAC is combined with dual antiplatelet therapy, the lower dose tested for stroke prevention in AF is recommended.
Based on our interpretation of available data we suggest:
| First choice | In patients with percutaneous coronary intervention after stenting receiving triple therapy, well-controlled VKA (TTR >70%, preferred INR range 2.0–2.5) or an NOAC may be chosen |
| When an NOAC is used in combination with dual antiplatelet therapy, the lower tested and licensed dose for stroke prevention in AF is preferred: dabigatran 110 mg twice daily, rivaroxaban 15 mg once daily, apixaban 2.5 mg twice daily, or edoxaban 30 mg once daily | |
| Comment | There is no preference for one NOAC over another. Published evidence on the combination of dual antiplatelet therapy and an NOAC is currently available only for dabigatran from the RE-LY trial |
| First choice | In patients with percutaneous coronary intervention after stenting receiving triple therapy, well-controlled VKA (TTR >70%, preferred INR range 2.0–2.5) or an NOAC may be chosen |
| When an NOAC is used in combination with dual antiplatelet therapy, the lower tested and licensed dose for stroke prevention in AF is preferred: dabigatran 110 mg twice daily, rivaroxaban 15 mg once daily, apixaban 2.5 mg twice daily, or edoxaban 30 mg once daily | |
| Comment | There is no preference for one NOAC over another. Published evidence on the combination of dual antiplatelet therapy and an NOAC is currently available only for dabigatran from the RE-LY trial |
| First choice | In patients with percutaneous coronary intervention after stenting receiving triple therapy, well-controlled VKA (TTR >70%, preferred INR range 2.0–2.5) or an NOAC may be chosen |
| When an NOAC is used in combination with dual antiplatelet therapy, the lower tested and licensed dose for stroke prevention in AF is preferred: dabigatran 110 mg twice daily, rivaroxaban 15 mg once daily, apixaban 2.5 mg twice daily, or edoxaban 30 mg once daily | |
| Comment | There is no preference for one NOAC over another. Published evidence on the combination of dual antiplatelet therapy and an NOAC is currently available only for dabigatran from the RE-LY trial |
| First choice | In patients with percutaneous coronary intervention after stenting receiving triple therapy, well-controlled VKA (TTR >70%, preferred INR range 2.0–2.5) or an NOAC may be chosen |
| When an NOAC is used in combination with dual antiplatelet therapy, the lower tested and licensed dose for stroke prevention in AF is preferred: dabigatran 110 mg twice daily, rivaroxaban 15 mg once daily, apixaban 2.5 mg twice daily, or edoxaban 30 mg once daily | |
| Comment | There is no preference for one NOAC over another. Published evidence on the combination of dual antiplatelet therapy and an NOAC is currently available only for dabigatran from the RE-LY trial |
Patients undergoing cardioversion
Cardioversion, whether electrical or pharmacological, is associated with a 5–7% risk of clinical thromboembolic events within the first month when patients with AF are not adequately anticoagulated. The risk in adequately anticoagulated patients on VKAs is ∼1%.16–18 A small, prospective observational study demonstrated that VKAs are important both before and after cardioversion.19 Retrospective analyses of the phase III trials of NOACs (RE-LY, ROCKET AF, and ARISTOTLE) found no difference in safety or efficacy between the NOACs and VKA therapy in patients with AF undergoing cardioversion.20–22
In the RE-LY trial (n = 18 113), 1983 cardioversions were performed in 1270 patients. In the intention-to-treat population at 30 days, stroke and systemic embolism rates were low (0.3–0.8%) and major bleeding rates showed no statistical differences between dabigatran and warfarin.20
In the ARISTOTLE trial (n = 18 201), 743 cardioversions were performed in 540 patients (265 patients on apixaban and 275 on warfarin). At 30 days, no stroke or systemic embolism events were reported in either group. One patient in each group developed major bleeding.10
The ROCKET AF investigators excluded patients when cardioversion was planned. Among the 14 264 enrolled patients, 143 underwent 181 electrical cardioversions and 142 underwent 194 pharmacological cardioversions on study medication.22 In the long-term on-treatment analysis, there were no significant differences between treatment groups in the incidence of stroke or systemic embolism or hospitalization. The incidence of major bleeding or non-major clinically relevant bleeding was increased in rivaroxaban-treated patients (HR 1.51; 95% CI 1.12–2.05; P = 0.0072).
The trials cannot be directly compared because of differences in methodology and study populations. Although none of these trial subgroups was adequately powered for outcomes, collectively the data suggest that the NOACs are comparable with warfarin in terms of safety and efficacy in patients with AF undergoing cardioversion, and may offer a suitable alternative to warfarin in this setting.
The exploratory X-VeRT trial specifically investigated the use of rivaroxaban in 1504 patients undergoing cardioversion.23 The primary efficacy outcome (composite of stroke, transient ischaemic attack, peripheral embolism, myocardial infarction, and cardiovascular death) occurred in two patients (0.51%) on rivaroxaban and five patients (1.02%) on warfarin. Major bleeding occurred in 0.6% of patients on rivaroxaban and 0.8% on warfarin. Rivaroxaban was associated with a significantly shorter time to cardioversion (mean 25 days) compared with VKAs (34 days) (P < 0.001).4 The results suggest that rivaroxaban is a safe and effective alternative to VKAs, providing a practical advantage by facilitating earlier cardioversion.19
Ongoing trials (EMANATE [NCT02100228] and ENSURE [NCT02072434]) will provide additional information about the safety of cardioversion in patients taking NOACs, with a focus on anticoagulant-naïve patients and/or patients in need of rapid cardioversion.
Based on our interpretation of available data we suggest:
| First choice | VKAs remain the standard of care in patients with AF undergoing cardioversion |
| The available data suggest that the NOACs are safe and effective alternatives, with practical advantages such as shortening the time to cardioversion | |
| Comment | Post hoc analyses suggest no apparent differences in safety and efficacy between apixaban, dabigatran, and rivaroxaban |
| First choice | VKAs remain the standard of care in patients with AF undergoing cardioversion |
| The available data suggest that the NOACs are safe and effective alternatives, with practical advantages such as shortening the time to cardioversion | |
| Comment | Post hoc analyses suggest no apparent differences in safety and efficacy between apixaban, dabigatran, and rivaroxaban |
| First choice | VKAs remain the standard of care in patients with AF undergoing cardioversion |
| The available data suggest that the NOACs are safe and effective alternatives, with practical advantages such as shortening the time to cardioversion | |
| Comment | Post hoc analyses suggest no apparent differences in safety and efficacy between apixaban, dabigatran, and rivaroxaban |
| First choice | VKAs remain the standard of care in patients with AF undergoing cardioversion |
| The available data suggest that the NOACs are safe and effective alternatives, with practical advantages such as shortening the time to cardioversion | |
| Comment | Post hoc analyses suggest no apparent differences in safety and efficacy between apixaban, dabigatran, and rivaroxaban |
Patients undergoing catheter ablation
Catheter ablation is an established treatment modality for patients with AF, particularly those with symptomatic paroxysmal AF. Thromboembolic events are among the most serious procedure-related complications, with an incidence between 1 and 5%.24–28 Silent brain lesions detected by magnetic resonance imaging are common after AF ablation (10–15% of patients),29 but their clinical relevance and implications for long-term cognitive decline are uncertain.30 Since it is unclear whether these lesions are due to thrombi or other blood material denatured by heating,31 it remains uncertain whether these lesions can be avoided by careful anticoagulation. There is consensus favouring anticoagulation during the ablation procedure with unfractionated heparin, targeting an activated clotting time of 300 s. Non-randomized studies have found lower thromboembolic risk when ablation is performed without discontinuing warfarin compared with warfarin discontinuation.28 A trial in which 1584 patients were randomized to continuous vs. interrupted warfarin found only 2 strokes in the group continuing with warfarin compared with 29 strokes and 10 transient ischaemic attacks in the discontinuation group (P < 0.001).32 Accordingly, uninterrupted warfarin administration at the time of AF ablation is preferred at many institutions, as reflected in the 2012 updated European Society of Cardiology (ESC) guidelines.33
Early experience with two NOACs (dabigatran and rivaroxaban) in conjunction with AF ablation has been reported from observational studies and case series.34,35 A number of observational studies compared the safety and efficacy of dabigatran vs. VKAs for AF ablation. A meta-analysis of 10 mostly single-centre retrospective studies found significant heterogeneity, including different regimens of NOAC interruption before and after ablation.36 Among 3648 patients, 2241 received warfarin and 1407 dabigatran. There were only 12 thromboembolic events, 3 during warfarin treatment and 9 during dabigatran therapy (odds ratio 2.38; 95% CI 0.82–6.85). The rate of major bleeding was similar for warfarin and dabigatran (odds ratio 1.05; 95% CI 0.62–1.80). Rates of minor bleeding events were also similar between the two treatment groups. The conclusion was that dabigatran is similar to warfarin in terms of safety and efficacy when used for peri-procedural anticoagulation in patients undergoing AF ablation.
Experience with rivaroxaban in conjunction with AF ablation is similarly limited to a few observational studies comparing rivaroxaban with warfarin.22,37,38 The largest observational prospective registry enrolled 642 patients treated with either uninterrupted warfarin (n = 321) or uninterrupted rivaroxaban (n = 321).38 There were no differences between the rivaroxaban and warfarin groups in the incidence of major bleeding complications [5 (1.6%) for rivaroxaban vs. 7 for warfarin (1.9%); P = 0.772], minor bleeding [16 (5.0%) vs. 19 (5.9%); P = 0.602], or thromboembolism [1 (0.3%) vs. 1 (0.3%); P = 1.0] in the first 30 days after the procedure. The authors concluded that rivaroxaban may be a safe and effective alternative to warfarin in patients undergoing AF ablation. Several observational studies have also reported low bleeding and stroke rates in patients undergoing ablation on uninterrupted apixaban.39–41
The procedure-specific risks of stroke, silent stroke, and bleeding emphasize the importance of acquiring data from randomized trials comparing NOAC therapy and VKAs in patients undergoing AF ablation. In a randomized trial with rivaroxaban (VENTURE-AF), 248 patients scheduled for ablation were randomly assigned to uninterrupted therapy with warfarin or rivaroxaban.42 The incidence of thromboembolic and major bleedings events was low in both treatment arms (one patient in each).
Ongoing trials [AXAFA with apixaban (NCT02227550) and RE-CIRCUIT (NCT02348723) with dabigatran] will provide prospectively collected data on outcomes, including silent ischaemic brain lesions in patients undergoing AF ablation on uninterrupted NOAC therapy compared with uninterrupted warfarin. These trials are exploratory for outcomes such as stroke because of the low event rates, but they should shed some light on major bleeding rates and possibly provide information about the effect of NOAC therapy on silent strokes in patients undergoing AF ablation.
Based on our interpretation of available data we suggest:
| First choice | In patients undergoing AF ablation, the OAC of choice is uninterrupted warfarin |
| Second choice | Uninterrupted dabigatran, apixaban, or rivaroxaban. |
| Third choice | Interrupted warfarin with bridging |
| Comment | Data on the efficacy and safety of edoxaban in patients undergoing AF ablation are not available |
| First choice | In patients undergoing AF ablation, the OAC of choice is uninterrupted warfarin |
| Second choice | Uninterrupted dabigatran, apixaban, or rivaroxaban. |
| Third choice | Interrupted warfarin with bridging |
| Comment | Data on the efficacy and safety of edoxaban in patients undergoing AF ablation are not available |
| First choice | In patients undergoing AF ablation, the OAC of choice is uninterrupted warfarin |
| Second choice | Uninterrupted dabigatran, apixaban, or rivaroxaban. |
| Third choice | Interrupted warfarin with bridging |
| Comment | Data on the efficacy and safety of edoxaban in patients undergoing AF ablation are not available |
| First choice | In patients undergoing AF ablation, the OAC of choice is uninterrupted warfarin |
| Second choice | Uninterrupted dabigatran, apixaban, or rivaroxaban. |
| Third choice | Interrupted warfarin with bridging |
| Comment | Data on the efficacy and safety of edoxaban in patients undergoing AF ablation are not available |
Patients with valvular heart disease and mechanical prosthetic heart valves
Although the use of transcatheter aortic valve implantation is increasing, surgical valve replacement with either bioprosthetic or mechanical valves is the more common approach, with mechanical prostheses having the advantage of durability but the disadvantages of thrombogenicity and need for life-long anticoagulation. An alternative to VKAs is needed and there was the hope that NOACs might fill the role, but the RE-ALIGN trial found even high-dose dabigatran neither safe nor effective.43 In that trial, 252 patients with recent or remote valve replacement were randomly assigned to a VKA (guideline-directed INR target range) or to dabigatran adjusted to a trough plasma level of ≥50 ng/mL. The trial was stopped early due to excess stroke (nine patients in the dabigatran group and none in the warfarin group) and major bleeding (seven patients in the dabigatran vs. two in the warfarin group). There was also excess valve thrombosis with dabigatran. This small study, although not definitive, suggests that dabigatran is not effective and that NOACs should not be selected for patients with mechanical prosthetic valves.
The term ‘non-valvular AF’ was developed to define patient eligibility for enrolment in the historical warfarin trials, excluding individuals with rheumatic mitral stenosis and AF, which was associated with a high risk of stroke. Since these patients were not included in the trials that established the non-inferiority boundaries, they were excluded from the NOAC trials and therefore from the labelling indications for NOAC use. We have little or no data on the efficacy of NOACs in this population, and patients with mitral stenosis should not be treated with NOACs, although the threshold of severity warranting this prohibition has not been established.
Other types of valvular heart disease (VHD), such as mitral or tricuspid insufficiency and aortic stenosis or insufficiency, occur commonly in patients with AF. In the ROCKET AF trial,43 14% of enrolled patients had clinically significant VHD, as did 26% in ARISTOTLE.44,45 In each of these trials, the treatment effect of the NOAC compared with warfarin was similar in patients with and without VHD, but rivaroxaban was associated with a higher risk of bleeding than warfarin in patients with VHD.44 In ARISTOTLE apixaban was associated with fewer bleeding complications in patients with and without VHD.45 Patients in the ROCKET-AF44 and ARISTOTLE45 trials with VHD differed with regard to age, stroke risks, and history of previous stroke or systemic embolism. Thus, NOACs may be prescribed for patients with VHD other than mitral stenosis or mechanical valve prostheses. A few hundred patients with bioprosthetic valves were included in the ARISTOTLE and ENGAGE AF trials, but the results in these subgroups have not been reported. It may be reasonable to treat patients who have bioprosthetic valves with NOACs unless intracardiac thrombus or other features placing the patient at an unusually high risk of thromboembolism or bleeding are present.
Based on our interpretation of available data we suggest:
| First choice | VKAs should be used for anticoagulation in patients with AF and mechanical prosthetic heart valves or moderate or severe (rheumatic) mitral stenosis |
| Comment | In the absence of data on the use of NOACs in this population, dabigatran, rivaroxaban, apixaban, and edoxaban should not be used |
| First choice | VKAs should be used for anticoagulation in patients with AF and mechanical prosthetic heart valves or moderate or severe (rheumatic) mitral stenosis |
| Comment | In the absence of data on the use of NOACs in this population, dabigatran, rivaroxaban, apixaban, and edoxaban should not be used |
| First choice | VKAs should be used for anticoagulation in patients with AF and mechanical prosthetic heart valves or moderate or severe (rheumatic) mitral stenosis |
| Comment | In the absence of data on the use of NOACs in this population, dabigatran, rivaroxaban, apixaban, and edoxaban should not be used |
| First choice | VKAs should be used for anticoagulation in patients with AF and mechanical prosthetic heart valves or moderate or severe (rheumatic) mitral stenosis |
| Comment | In the absence of data on the use of NOACs in this population, dabigatran, rivaroxaban, apixaban, and edoxaban should not be used |
| First choice | In patients with AF and other valve abnormalities (including mitral, aortic, or tricuspid insufficiency and aortic stenosis), apixaban and rivaroxaban may be used |
| Second choice | Dabigatran and edoxaban |
| Third choice | VKAs |
| First choice | In patients with AF and other valve abnormalities (including mitral, aortic, or tricuspid insufficiency and aortic stenosis), apixaban and rivaroxaban may be used |
| Second choice | Dabigatran and edoxaban |
| Third choice | VKAs |
| First choice | In patients with AF and other valve abnormalities (including mitral, aortic, or tricuspid insufficiency and aortic stenosis), apixaban and rivaroxaban may be used |
| Second choice | Dabigatran and edoxaban |
| Third choice | VKAs |
| First choice | In patients with AF and other valve abnormalities (including mitral, aortic, or tricuspid insufficiency and aortic stenosis), apixaban and rivaroxaban may be used |
| Second choice | Dabigatran and edoxaban |
| Third choice | VKAs |
Patients with time in therapeutic range of >70% on warfarin
Patients with well-controlled anticoagulation intensity on VKA therapy (TTR >70%) have a low risk of thromboembolism and bleeding.46–48 An average TTR of >70% for individual patients is recommended in a position statement from the ESC Working Group on Thrombosis Anticoagulation Task Force.49 Where TTR using the linear interpolation method of Rosendaal is not always available, other measures of quality of anticoagulation control, such as proportion of time in therapeutic INR range, may be used. In the randomized trials, the effect size of NOAC compared with warfarin for stroke and bleeding was maintained irrespective of centre-based TTR quartile, and the clear relative risk reduction of NOACs for intracranial haemorrhage compared with VKA persisted, although the difference in absolute rates was small. A high TTR can also easily be altered by acute events, such as infection (requiring antibiotics), hospitalization, decompensated heart failure, and deterioration of renal or hepatic function.
A meta-analysis of the NOAC trials found a greater reduction in major bleeding with the NOACs when centre-based TTR was <66% than when it was ≥66% (relative risk 0.69, 95% CI 0.59–0.81 vs. 0.93, 0.76–1.13; interaction P = 0.022).34 In a longitudinal follow-up of AF patients on a VKA with initial baseline TTR of 100%, the SAMe-TT2R2 score [Sex, Age <60 years, Medical history (at least two of the following: hypertension, diabetes, CAD/myocardial infarction, PAD, heart failure, previous stroke, pulmonary disease, hepatic, or renal disease), Treatment (interacting drugs, e.g. amiodarone for rhythm control), current Tobacco use (two points), Race (non-Caucasian, two points)] identified anticoagulated AF patients who were likely to remain event free on VKA therapy (SAMe-TT2R2 score 0–2, with TTR >70%).50–52 This difference is attributable to adverse events such as thromboembolism and bleeding when the TTR is low or labile.51 The SAMe-TT2R2 score may help to guide the selection of an NOAC or VKA treatment without a trial of warfarin that could expose patients to an increased risk of thromboembolism or intracranial haemorrhage.
Ultimately, patient values and preferences should be considered,53 particularly for patients with TTR of >70% for whom routine anticoagulation INR monitoring is challenging, self-monitoring is unsuitable, or adherence to the dietary, drug, or alcohol restrictions required for safe VKA use is difficult. Substitution of an NOAC may be appropriate for such patients but, as always, associated comorbidities should be considered in choosing one NOAC over another.
Based on our interpretation of available data we suggest:
| First choice | In patients with AF and TTR >70% on warfarin, it is reasonable to continue with VKA treatment, with careful monitoring to ensure that TTR remains >70% |
| Second choice | Substitution of VKA therapy with an NOAC may be considered in relation to the following:
|
| Comment | The selection of an NOAC agent and dose should be based on specific patient characteristics. There is no preference for one NOAC over another. |
| First choice | In patients with AF and TTR >70% on warfarin, it is reasonable to continue with VKA treatment, with careful monitoring to ensure that TTR remains >70% |
| Second choice | Substitution of VKA therapy with an NOAC may be considered in relation to the following:
|
| Comment | The selection of an NOAC agent and dose should be based on specific patient characteristics. There is no preference for one NOAC over another. |
| First choice | In patients with AF and TTR >70% on warfarin, it is reasonable to continue with VKA treatment, with careful monitoring to ensure that TTR remains >70% |
| Second choice | Substitution of VKA therapy with an NOAC may be considered in relation to the following:
|
| Comment | The selection of an NOAC agent and dose should be based on specific patient characteristics. There is no preference for one NOAC over another. |
| First choice | In patients with AF and TTR >70% on warfarin, it is reasonable to continue with VKA treatment, with careful monitoring to ensure that TTR remains >70% |
| Second choice | Substitution of VKA therapy with an NOAC may be considered in relation to the following:
|
| Comment | The selection of an NOAC agent and dose should be based on specific patient characteristics. There is no preference for one NOAC over another. |
One stroke risk factor (CHA2DS2VASc score of 1 in males or 2 in females)
Patients with a single additional stroke risk factor have an increased risk of AF-related stroke. The stroke risk is lower than in patients with multiple vascular risk factors.54,55 Reported ischaemic stroke and thromboembolism rates vary widely, but in some studies the annual risk was 0.5–3.0%.56,57 Different individual single stroke risk factors occurring in isolation to yield a CHA2DS2-VASc [Congestive heart failure (or left ventricular systolic dysfunction), Hypertension, Age ≥75 years (2 points), Diabetes mellitus, prior Stroke or TIA or thromboembolism (2 points), Vascular disease (e.g. PAD, myocardial infarction, and aortic plaque), Age 65–74 years, Sex category (i.e. female sex)] score of 1 in males and 2 in females are not associated with equal stroke risk: the highest risk is associated with hypertension and age 65–74 years followed by diabetes.44,58
Women with a CHA2DS2-VASc score of 1 (or 0 for males) are at low risk, and no antithrombotic therapy is recommended.59 Anticoagulation should be considered for patients with AF and one or more additional stroke risk factors (i.e. men with a CHA2DS2-VASc score of ≥1 or women with a score of ≥2) considering patient preference and further patient characteristics.60,61 Analyses of net clinical benefit (NCB) incorporating stroke, mortality, and bleeding support this approach, with a positive NCB for OAC vs. aspirin, or OAC vs. no treatment, even when only one stroke risk factor is present, while the NCB of aspirin vs. no treatment for this patient group is neutral or negative.55,58,59,62,63
The choice of anticoagulant in this situation cannot be generalized, but several considerations can be delineated. There are no specific randomized trials with NOACs only in patients with a single stroke risk factor, given that absolute event rates would be low.
Subgroup analyses show similar effect sizes for safety and efficacy in patients with only one stroke risk factor for dabigatran and apixaban, whereas the absolute stroke and bleeding risk is relatively low (although above the suggested 1% ischaemic stoke rate treatment threshold for NOACs).64–66 There are data for dabigatran and apixaban in the randomized trials in patients with a single stroke risk factor, whereas trials investigating rivaroxaban and edoxaban mainly recruited patients with two or more stroke risk factors. In the ROCKET AF trial, the proportion of enrolled patients with CHADS2 scores of 2 was capped at 10%.
The data from the small randomized clinical trial subgroups are complemented by real world observational data for using NOACs in such patients.67,68 The largest ‘real world’ dataset comes from Seeger et al., where 7327 patients with a CHA2DS2-VASc score of 1 treated with dabigatran or warfarin were compared in a propensity-matched analysis, where no heterogeneity was seen in efficacy and safety compared with those with CHA2DS2-VASc ≥2.67
Putting these data into context with the VKA data described earlier with a positive NCB for OAC treatment even with a single stroke risk factor, we suggest that OAC should be considered in patients with a single stroke risk factor taking patients values and preferences into consideration, notwithstanding the lack of large randomized trial subgroup data.
Based on our interpretation of available data we suggest:
| First choice | In men or women with AF and an additional stroke risk factor other than sex (i.e. CHA2DS2VASc score of 1 in men or 2 in women), OAC should be considered, based on limited clinical trial data dabigatran (150 mg twice daily is preferred) or apixaban may be considered |
| First choice | In men or women with AF and an additional stroke risk factor other than sex (i.e. CHA2DS2VASc score of 1 in men or 2 in women), OAC should be considered, based on limited clinical trial data dabigatran (150 mg twice daily is preferred) or apixaban may be considered |
| First choice | In men or women with AF and an additional stroke risk factor other than sex (i.e. CHA2DS2VASc score of 1 in men or 2 in women), OAC should be considered, based on limited clinical trial data dabigatran (150 mg twice daily is preferred) or apixaban may be considered |
| First choice | In men or women with AF and an additional stroke risk factor other than sex (i.e. CHA2DS2VASc score of 1 in men or 2 in women), OAC should be considered, based on limited clinical trial data dabigatran (150 mg twice daily is preferred) or apixaban may be considered |
Patients with a single-documented episode of atrial fibrillation
Diagnosis of AF requires electrocardiographic (ECG) documentation. Only an ECG allows differentiation between AF and other supraventricular arrhythmias, and correct interpretation of the ECG should precede initiation of OAC therapy. The natural history of AF is progressive, although patients may be free of AF for prolonged periods (even years). Hence, patients with a first-documented episode should be considered at sufficient risk of stroke to warrant assessment of the need for anticoagulation. Stroke risk was similar in patients with paroxysmal, persistent, and permanent forms of AF in the ACTIVE trial69 and in a prospective cohort of stroke patients,70 while a slightly lower risk has been reported for patients with paroxysmal AF in a sub-analysis of the combined AVERROES and ACTIVE datasets.71 In the ROCKET AF trial, the mortality rate was slightly lower in patients with paroxysmal than with persistent or permanent AF.72 The burden of AF (minutes or hours per month) seems to be related to the risk of thromboembolism, whereas there is a weaker association between the timing of AF episodes and stroke. Some data suggest that the risk of ischaemic stroke is elevated in patients with atrial tachyarrhythmias identified by pacemakers or other implanted arrhythmia devices.73,74 Such patients often develop overt AF. Ongoing trials will determine whether OAC is justified in patients with device-detected atrial high-rate episodes.
In summary, patients with a single episode of AF should be anticoagulated following the same principles as patients with repeated episodes of AF. When the decision is not clear—e.g. in younger patients with a CHA2DS2VASc score of 1—or when the risk of bleeding is high, withholding therapy until AF recurs may be reasonable.
Based on our interpretation of available data we suggest:
| Comment | The choice of OAC is not influenced by the pattern of AF, frequency of AF, or number of AF episodes |
| Comment | The choice of OAC is not influenced by the pattern of AF, frequency of AF, or number of AF episodes |
| Comment | The choice of OAC is not influenced by the pattern of AF, frequency of AF, or number of AF episodes |
| Comment | The choice of OAC is not influenced by the pattern of AF, frequency of AF, or number of AF episodes |
Patients receiving rhythm- and rate-control therapy
The NOACs have fewer interactions than VKAs with food and other medications. The EHRA has published a practical guide listing these interactions.9 Digitalis and β-blockers do not have known interactions with the NOACs. Diltiazem, verapamil, amiodarone, dronedarone, and quinidine interact with the absorption of NOACs in the gastrointestinal tract. These interactions, mediated by the P-glycoprotein system, can increase blood levels by 10–100%.
Amiodarone increases blood levels of NOACs only slightly, and there is generally no need to modify NOAC dose during concomitant amiodarone treatment except in patients with renal impairment who are taking rivaroxaban. Patients treated with amiodarone at the time of randomization in the ENGAGE-AF trial had significantly fewer ischaemic events on edoxaban vs. warfarin than did those who were not on amiodarone.75 Dronedarone increases NOAC levels through interactions with P-glycoprotein and cytochrome P450-3A4, and should not be used in patients taking dabigatran. Indirect data suggest that the lower dose of rivaroxaban (15 mg daily) can be used safely in patients treated with dronedarone. The ENGAGE AF protocol recommended reducing the dose of edoxaban to 30 mg daily during concurrent dronedarone therapy.
Diltiazem has a minor effect on NOAC levels and can be combined without dose reduction except in patients with kidney disease who are taking rivaroxaban. Verapamil decreases the NOAC dose requirement mainly through P-glycoprotein interaction, although it is also a weak inhibitor of cytochrome P450-3A4.
Based on our interpretation of available data we suggest:
| Choice and dose of NOAC | The dose of dabigatran or edoxaban should be reduced in patients taking verapamil |
| No dose reduction is needed in patients taking rivaroxaban with verapamil | |
| Apixaban does not interact with amiodarone or verapamil | |
| Dabigatran is contraindicated in combination with dronaderone | |
| Edoxaban 30 mg should be used in patients on dronedrone |
| Choice and dose of NOAC | The dose of dabigatran or edoxaban should be reduced in patients taking verapamil |
| No dose reduction is needed in patients taking rivaroxaban with verapamil | |
| Apixaban does not interact with amiodarone or verapamil | |
| Dabigatran is contraindicated in combination with dronaderone | |
| Edoxaban 30 mg should be used in patients on dronedrone |
| Choice and dose of NOAC | The dose of dabigatran or edoxaban should be reduced in patients taking verapamil |
| No dose reduction is needed in patients taking rivaroxaban with verapamil | |
| Apixaban does not interact with amiodarone or verapamil | |
| Dabigatran is contraindicated in combination with dronaderone | |
| Edoxaban 30 mg should be used in patients on dronedrone |
| Choice and dose of NOAC | The dose of dabigatran or edoxaban should be reduced in patients taking verapamil |
| No dose reduction is needed in patients taking rivaroxaban with verapamil | |
| Apixaban does not interact with amiodarone or verapamil | |
| Dabigatran is contraindicated in combination with dronaderone | |
| Edoxaban 30 mg should be used in patients on dronedrone |
Limitations and caveats
The suggestions presented in this two-part expert consensus paper were developed by experienced clinicians and investigators based on present and evolving data. Some suggestions been made in the absence of data by consensus or majority decision of the group of authors. Although we comprehensively reviewed and summarized the literature, our search was not systematic or exhaustive and new data are emerging rapidly. Readers should remain alert to evolving evidence. We have not graded the quality of evidence objectively or systematically, and the strength of suggestions is variable and in some cases limited. Readers should also be aware that this consensus statement was developed by individuals who were engaged in the development and clinical evaluation of the NOACs in clinical trials, and that data collected from broad clinical practice are still limited. Finally, in developing advice for the management of patients with specific comorbidities, it is not possible to capture the unique characteristics of individuals and their concomitant therapy, which require case-by-case assessment by physicians and other prescribers, with comprehensive knowledge of the patient's likelihood of tolerating one therapy over another and the patient's expressed values and preferences.
Authors' contributions
Conceived and designed the research: all authors contributed to the review. Drafted the manuscript: each author drafted one section of the manuscript. G.B. and J.L.H, performed the final editing. Made critical revision of the manuscript for key intellectual content: all authors.
Acknowledgements
We acknowledge the editorial support of Rebecca Craven.
Conflict of interest: Dr Aisenberg has received honoraria for speaking or participating on advisory boards for Boehringer Ingelheim, Pfizer, and Portola. Dr Ansell has received honoraria or consulting fees from Boehringer Ingelheim, Bristol-Myers Squibb, Pfizer, Daiichi-Sankyo, Janssen, Instrumentation Laboratories, Roche Diagnostics, Alere Home Monitoring, and Perosphere. Dr Ansell has equity interest in Perosphere. Dr Atar received fees, honoraria from Boehringer Ingelheim, Bayer, BMS/Pfizer, Daiichi-Sankyo, Medtronic, Nycomed-Takeda, Cardiome, and AstraZeneca. Dr Breithardt reports honoraria from Bayer HealthCare and Bristol-Myers Squibb and Pfizer, and consulting and advisory board fees from Bayer HealthCare, Bristol-Myers Squibb and Pfizer, and Sanofi –Aventis. Dr Diener received honoraria for participation in clinical trials, contribution to advisory boards or oral presentations from: Abbott, Allergan, AstraZeneca, Bayer Vital, BMS, Boehringer Ingelheim, CoAxia, Corimmun, Covidien, Daiichi-Sankyo, D-Pharm, Fresenius, GlaxoSmithKline, Janssen-Cilag, Johnson & Johnson, Knoll, Lilly, MSD, Medtronic, MindFrame, Neurobiological Technologies, Novartis, Novo-Nordisk, Paion, Parke-Davis, Pfizer, Sanofi-Aventis, Schering-Plough, Servier, Solvay, St. Jude, Syngis, Talecris, Thrombogenics, WebMD Global, Wyeth, and Yamanouchi. Financial support for research projects was provided by AstraZeneca, GSK, Boehringer Ingelheim, Lundbeck, Novartis, Janssen-Cilag, Sanofi-Aventis, Syngis, and Talecris. The Department of Neurology at the University Duisburg-Essen received research grants from the German Research Council (DFG), German Ministry of Education and Research (BMBF), European Union, NIH, Bertelsmann Foundation, and Heinz-Nixdorf Foundation. HCD has no ownership interest and does not own stocks of any pharmaceutical company. Dr Eikelboom has received honoraria and/or research grants from AstraZeneca, Boehringer Ingelheim, Bayer, Bristol-Myers Squibb, Daiichi-Sankyo, GlaxoSmithKline, Janssen, and Sanofi-Aventis. Dr Ezekowitz has served as a consultant for Boehringer Ingelheim, Pfizer, Bristol-Myers Squibb, Daiichi-Sankyo, Merck, J & J, Bayer, and Medtronic. Dr Granger received grant funding and reports consulting from BMS, Pfizer, Daiichi-Sankyo, BI, Bayer, and Janssen. Dr Halperin reports consulting fees from Bayer HealthCare AG, Boehringer Ingelheim, Daiichi-Sankyo, Johnson & Johnson, Ortho-McNeil-Janssen Pharmaceuticals, Pfizer, Sanofi-Aventis, AstraZeneca, Biotronik, Boston Scientific, Janssen, and Medtronic. Dr Hohnloser has received consulting fees from Bayer, BMS, Sanofi-Aventis, St Jude Medical, Boehringer Ingelheim, Cardiome, and Medtronic Vascular; and lecture fees from Sanofi-Aventis, Bristol-Myers Squibb, Pfizer, Boehringer Ingelheim, and St Jude Medical. Dr Hylek served on advisory boards for Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, Daiichi-Sankyo, Janssen, Medtronic, Pfizer, received honoraria for conference lecture from Bayer, Boehringer Ingelheim, and Pfizer. Dr Kirchhof reports consulting fees and honoraria from 3M Medica, MEDA Pharma, AstraZeneca, Bayer Healthcare, Boehringer Ingelheim, Daiichi-Sankyo, Medtronic, Merck, MSD, Otsuka Pharma, Pfizer/BMS, Sanofi, Servier, Siemens, and TAKEDA; research grants from 3M Medica/MEDA Pharma, Cardiovascular Therapeutics, Medtronic, OMRON, Sanofi, St. Jude Medical, German Federal Ministry for Education and Research, Fondation Leducq, German Research Foundation, and the European Union; travel support received from the European Society of Cardiology, the European Heart Rhythm Association, and from the German Atrial Fibrillation Competence NETwork. Dr Lane has received investigator-initiated educational grants from Bayer Healthcare, Boehringer Ingelheim and Bristol-Myers Squibb. She has also been on the speaker bureau for Boehringer Ingelheim, Bayer, Bristol-Myers Squibb/Pfizer and is a Steering Committee member for a Phase IV trial sponsored by Bristol-Myers Squibb. Dr Lip (i) Guideline membership/reviewing: ESC Guidelines on Atrial Fibrillation, 2010 and Focused Update, 2012; ESC Guidelines on Heart Failure, 2012; American College of Chest Physicians Antithrombotic Therapy Guidelines for Atrial Fibrillation, 2012; NICE Guidelines on Atrial Fibrillation, 2006 and 2014; NICE Quality Standards on Atrial Fibrillation 2015; ESC Cardio-oncology Task Force, 2015; ESC Working Group on Thrombosis position documents (2011–). Chairman, Scientific Documents Committee, European Heart Rhythm Association (EHRA). Reviewer for various guidelines and position statements from ESC, EHRA, NICE, etc. (ii) Steering Committees/trials: Includes steering committees for various Phase II and III studies, Health Economics & Outcomes Research, etc. Investigator in various clinical trials in cardiovascular disease, including those on antithrombotic therapies in atrial fibrillation, acute coronary syndrome, lipids, etc. (iii) Consultant/Advisor/Speaker: Consultant for Bayer, Astellas, Merck, Sanofi, BMS/Pfizer, Biotronik, Medtronic, Portola, Boehringer Ingelheim, Microlife, and Daiichi-Sankyo. Speaker for Bayer, BMS/Pfizer, Medtronic, Boehringer Ingelheim, Microlife, Roche, and Daiichi-Sankyo Dr Veltkamp has received consulting honoraria, research support, travel grants, and speakers' honoraria from Bayer HealthCare, Boehringer Ingelheim, BMS Pfizer, Daiichi-Sankyo, Roche Diagnostics, CSL Behring, St. Jude Medical, Medtronic, and Sanofi-Aventis. Dr Verheugt received honoraria for speaker fees and consultancy honoraria from Bayer Healthcare, Boehringer Ingelheim, BMS/Pfizer, and Daiichi-Sankyo.
References


{kind=link}