




Cover image
The left atrial appendage: from embryology to prevention of thromboembolism
Giuseppe Patti1*, Vittorio Pengo2, Rossella Marcucci3, Plinio Cirillo4, Giulia Renda5, Francesca Santilli6, Paolo Calabrò7, Alberto Ranieri De Caterina5,8, Ilaria Cavallari1, Elisabetta Ricottini1, Vito Maurizio Parato9,10, Giacomo Zoppellaro2, Giuseppe Di Gioia1, Pietro Sedati1, Vincenzo Cicchitti9, Giovanni Davì6, Enrica Golia7, Ivana Pariggiano7, Paola Simeone6, Rosanna Abbate3, Domenico Prisco3, Marco Zimarino5, Francesco Sofi3,11, Felicita Andreotti12, and on behalf of the Working Group of Thrombosis of the Italian Society of Cardiology
1Institute of Cardiology, Campus Bio-Medico University, Rome, Italy; 2Department of Cardiac, Thoracic and Vascular Sciences, University of Padova, Padova, Italy; 3Department of Experimental and Clinical Medicine, University of Florence, Florence, Italy; 4Department of Advanced Biological Sciences, University Federico II, Naples, Italy; 5Institute of Cardiology, G. d'Annunzio University, Chieti, Italy; 6Department of Medicine and Aging, G. d'Annunzio University, Chieti, Italy; 7Division of Cardiology, Department of Cardiothoracic Sciences, Second University of Naples, Naples, Italy; 8G Pasquinucci Hospital, Massa, Italy; 9Cardiology Unit, Madonna del Soccorso Hospital, San Benedetto del Tronto, Italy; 10Politecnica Delle Marche University, San Benedetto del Tronto, Italy; 11Don Carlo Gnocchi Foundation, Florence, Italy; and 12Department of Cardiovascular Science, Catholic University, Rome, Italy
The left atrial appendage (LAA) is the main source of thromboembolism in patients with non-valvular atrial fibrillation (AF). As such, the LAA can be the target of specific occluding device therapies. Optimal management of patients with AF includes a comprehensive knowledge of the many aspects related to LAA structure and thrombosis. Here we provide baseline notions on the anatomy and function of the LAA, and then focus on current imaging tools for the identification of anatomical varieties. We also describe pathogenetic mechanisms of LAA thrombosis in AF patients, and examine the available evidence on treatment strategies for LAA thrombosis, including the use of non-vitamin K antagonist oral anticoagulants and interventional approaches.
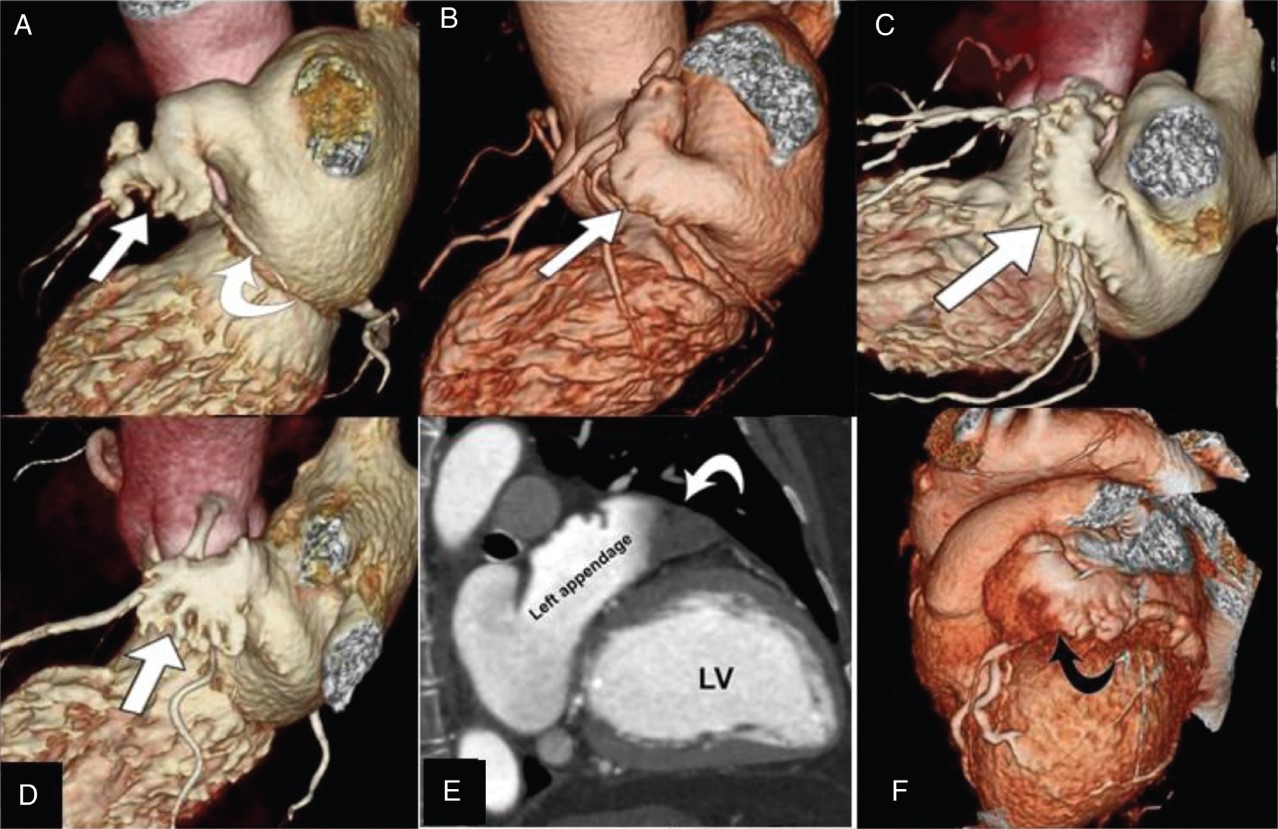
Figure 1 Computed tomography/magnetic resonance imaging of the left atrial appendage. (A–D) Computed tomography three-dimensional volume rendering reconstructions illustrating different left atrial appendage shapes. In (A), a windsock morphology (arrow) with a dominant lobe and an accessory secondary lobe; note the left circumflex coronary artery below the left atrial appendage (curved arrow). In (B), a chickenwing shape, with an evident bend in the proximal part of the dominant lobe (arrow). In (C), a cauliflower morphology (arrow). In (D), a cactus-like shape, with a dominant central lobe and secondary lobes extending from the central lobe in both superior and inferior directions (arrow). (E) Computed tomography image delineating the entire extension of the LAA with a filling defect in the apex consistent with intracavitary thrombus (curved arrow). Left ventricle is indicated. (F) Computed tomography three-dimensional volume rendering reconstruction showing a reduced colour brightness in the apex of the left atrial appendage (curved arrow) due to lack of intracavitary contrast enhancement caused by in situ thrombosis. (G) Left atrial appendage (arrow) on a two-chamber magnetic resonance imaging (magnetic resonance imaging-SSFP sequence). (H) Left atrial appendage with in situ thrombosis (curved arrow) on magnetic resonance imaging.

