






Abstract
Objective: This study was undertaken to determine the extent of endothelium derived nitric oxide (EDNO) production of the internal mammary artery (IMA) bypass graft and of the native coronary circulation by measuring its stable metabolite (NO2: nitrite) in different sampling sites: internal mammary free cut end flow, in the coronary sinus prior and after anastomosis completion, and to compare them to the nitrite level of the normal plasma. Methods: Nitrite level was determined with fluoroscopy using 4 hydroxycoumarin nitrozation in 50 consecutive patient undergoing onpump myocardial revascularization. Results: Nitrite levels in the normal plasma were found to be 31.2 μmol. Nitrite level in systemic and coronary circulation after total heparinization, prior to extracorporeal circulation (ECC) was found to be 60.8 μmol (lower quartile /l.q./: 46.6 μmol, upper quartile /u.q./: 70.0 μmol,) and 58.3 μmol,(l.q.:47.8 μmol, u.q.:70.0 μmol) respectively, and of the IMA bypass graft free cut end flow was 54.4 μmol,(l.q.:42.0 μmol, u.q.:66.8 μmol) while in the coronary sinus, after completion the IMA anastomosis, it was 45.71 μmol (l.q.: 35.0 μmol, u.q.: 55.0 μmol), (all geometric mean). Conclusions: Total heparinization enhances EDNO production. Nitrite concentration in the IMA free cut end flow is similar or greater, than that of the native coronary circulation, however, after IMA bypass graft construction significant reduction (P≪0.001) could be measured in the coronary sinus.
1 Introduction
In normoxia the endothelium of the internal mammary artery produces endothelium derived relaxing factor (EDNO), which active component is nitric oxide (NO) radical. The EDNO production is continuous, and in the plasma, NO radical is an important determinant of vasotone and of actual diameter of the given vessel [1–6,15].
This basal EDNO production takes place in the endothelium of the internal mammary artery (IMA) (and of different arteries, coronaries, as well as of the saphenous vein). In normoxia, nitric oxide, synthetized from l-Arginin has different protective effects. In the tunica media it causes relaxation (cGMP pathway) and blocks mitogenesis of smooth muscle cell (no proliferation). Intravasally, NO reduces platelet adhesion and aggregation, and causes downstream vasodilatation [5].
The level of stable metabolites of EDNO (nitrite and nitrate) in the plasma is between 13.2 and 45.5 μMol [6]. In moderate hypoxia the described vasodilatative mechanism is supported by another endothelial function: the effects of prostanoids synthetized from arachidon acid (e.g. prostacyclin, PGI 2) through the cAMP pathway also creates local and downstream vasodilatation [7].
However, the actual vasotone is perpetually affected by substances with vasoconstrictor effect (endothelin, prostaglandin F 2α) as well as by central vasomotor effects and humoral agents [8–11].
In animal studies, the IMA EDNO effects are investigated in vessel segments preconditioned with different vasoactive substances in order to differentiate endothelium dependent and independent vasodilatative effects.
In this study the nitrite concentration changes were measured in the coronary circulation in order to prove, that IMA bypass grafting through EDNO production would alter (increase?) the nitrite concentration in the coronary vasculature, as a possible way of protecting the ischemic myocardium, and as an indirect (biochemical) proof of long-lasting patency of the IMA bypass graft. It was expected, based on the respective experimental works [12–14,16] that, in samples taken in the period of total heparinization, nitrite levels would be greater than in the normal plasma. Data were collected for EDNO production of the internal mammary artery bypass graft before and after anastomosis completion during extracorporeal circulation.
2 Material and methods
In 1999, out of 668 extracorporeal circulation (ECC) procedure 430 were carried out for ischemic heart disease (IHD). Within this subgroup of patients the team conducting this study performed 74 cases, out of which 50 were suitable for inclusion.
2.1 Patient inclusion criteria
IMA(s) usability, (no premammary artery subclavian stenosis, IMA diameter greater than 2 mm).
Stable myocardial performance, no need for nitrates perioperatively.
2.2 Patients characteristics
Number: 50, female: 11, male: 39. Age groups (years) 40–49: six patients, 50–59:12, 60–69:19, ≧ 70: 13 patients. AP classification I: no patients. II: 19 patients, III: 22, IV: 9 patients. Ejection fraction (%) 30–39:12 patients, 40–49: 11 patients, 50–59: 11 patients, 60–69: 15 patients, ≪70: one patient. Preoperative myocardial infarction (MI) 17 patients, reMI: three patients, (AP: angina pectoris, EF: ejection fraction, reMI: second myocardial infarction).
2.3 Operative technique
Myocardial revascularization was carried out employing extracorporeal circulation with total bypass. Left ventricular vent and aortic cross clamp was employed in moderate hypothermia (30°C centigrade). Coronary sinus balloon catheter was used for retograde cardioplegia (St. Thomas solution) and NO2 sampling. Total bypass (snared cavae), coronary sinus balloon catheter and aortic cross clamp were preconditions of sampling exclusively from the IMA bypass graft derived blood on the venous side [17]. Reference plasma nitrite levels before surgery were determined in ten patients enrolled into the study, while intraoperative reference nitrite level samples were taken from the subclavian vein (Fig. 1 ).
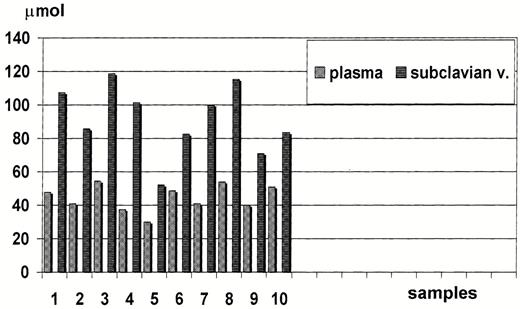
Nitrite levels in the native plasma, and after total heparinization in the subclavian vein (10-10 samples).
2.4 Sample sites
Subclavian vein after total heparinization (activated clotting time (ACT) above 400 s).
Coronary sinus before cross clamp the aorta.
IMA free cut end flow sample taken right before anastomosis construction.
Coronary sinus after IMA bypass graft completion, but before declamping the aorta.
All samples were stored in a tank filled with ice cubes (temperature 2–4°C) and in the laboratory after centrifugation the plasma samples were deep frozen to −20°C centigrade.
Nitrite level determination with 4-hydroxycoumarin (Application of Takafumi Ohta's method) [18].
This fluorometric method is based on the nitrosation of 4-hydroxycoumarin in acidic medium and subsequent reduction to 3-amino-4-hydroxycoumarin, which is fluorescent in alkaline medium. The fluorescence intensity is proportional to the nitrite concentration in the range of 3–1 μg/ml in the sample solution, with a relative standard deviation of 0.5 % (50 μ/ml). The plasma nitrite content was determined after the reduction the nitrate content of the plasma with Cadmium pearls. The plasma volume for measurement was 20 μl. The measurement was carried out with a sample of 50 times dilution, therefore at the calculation of the actual nitrite level this factor had to be taken into consideration.
2.5 Statistical analysis
All data presented in the text are geometric mean, as those represent lognormal distribution. Median and lower and upper quartiles are also presented. Data were analyzed after log-transformation. ANOVA was used for repeated measurements, so a value of P≪0.05 was considered significant. (Satistica SoftStat Inc. Tulsa, OK, USA). Post hoc multiple, paired comparisons were carried out with Bonferroni correction. (Statistical analysis was carried out by Andras Paksi)
3 Results
Nitrite concentrations of the systemic circulation - measured in the subclavian vein after total heparinization compared to samples taken from the normal plasma are described in Fig. 1. Nitrite levels in the systemic circulation are twofold greater than that of the normal plasma.
Fig. 2 describes nitrite concentration of the four sampling sites. Comparing nitrite concentrations measured in the subclavian vein and native coronary circulation the difference is not significant just like between the coronary sinus sample and of the free cut end flow of the IMA bypass graft (before IMA bypass graft completion). Furthermore, if nitrite concentration of the subclavian vein and of the IMA free cut end flow are compared the difference is significant (P≪0.05). When samples of IMA free cut end flow and of coronary sinus samples after bypass completion is are compared, the difference is statistically significant (P≪0.05). Finally, nitrite concentration in the coronary sinus before and after IMA bypass graft completion are consequently lower than prior concentrations, the difference is significant (P≪0.05).
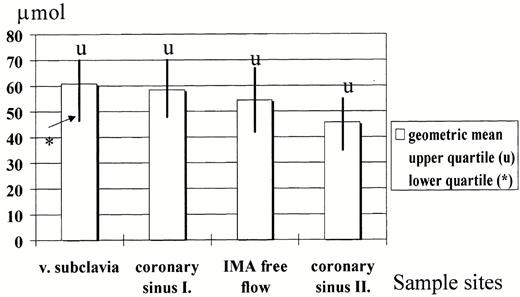
Nitrite concentration in the subclavian vein, in the coronary sinus prior and after IMA bypass graft completion and in the IMA free cut flow.
4 Discussion
The long-lasting effectivity of myocardial revascularization with arteries is based on four factors. These are punctual surgical technique, ideal geometry between the arterial bypass graft and the recipient vessel, intact vasoregulation and finally complex endothelial function of the arterial bypass graft. The effects of IMA EDNO can be studied in animal experiments with bioassay measurements using coronary segments preconditioned with different vasoactive agents to detect EDNO induced vasodilatations.
In clinical practice during heart surgery, certain endothelial functions of the human vasculature can only be studied in pathophysiological and artificial conditions, which per se affect these functions. There are data from Kouretas [11] and Li [13], implying that total heparinization increases EDNO production, while reduces the level of endothelial substances with vasoconstrictive properties (like endothelin).
These experiences support our findings that, using a very sensitive method for nitrite level measurement in the plasma, nitrite concentrations of the systemic and coronary circulation and of IMA bypass graft increase during extracorporeal circulation.
However, after IMA bypass graft completion there is a definite nitrite level reduction in the coronary circulation, though the concentration of the IMA free cut end flow is near the same, or occasionally higher, than that of the native coronary circulation. Furthermore, nitrite concentration in the native coronary circulation is greater, than that after IMA bypass graft completion.
The obeservation of Pearson and coworkers [5] supports these findings. These authors’ experimental work proved, that during normoxia EDNO production is even, while moderate hypoxia induces greater production both of EDNO and prostanoids. During cross clamp time EDNO production may decrease to the observed concentrations in the native coronary circulation as well as in the internal mammary artery graft due to lack of flow in he previous system and diminished flow in the latter. These effects may lead to a certain degree of ischemic injury, which is inductive to decrease EDNO released from the endothelium [19].
In this study we collected data about the changes of the endothelial function of the coronary circulation and of the internal mammary artery bypass graft. A divergent trend of nitrite levels of the coronary circulation and of the IMA endothelium could be observed. Namely, in the first phase of surgery, there has been a definite increase of NO2 level in the plasma and in the native coronary circulation due to the effect of heparin, and a decrease could be found after the IMA anastomosis completion.
To our knowledge, there are no data available as yet about the dynamic changes of EDNO production either in the coronary circulation or in the internal mammary artery bypass graft in clinical settings. Certainly, the inductive effect of total heparinization on EDNO synthesis is far from what may happen in physiological conditions, and appears to be as limitation of the study. (Although, suggests clinical implication: to maintain heparin administration for days after surgery).
Statistical analysis clearly proves, that the applied method for measurement the stable metabolite of EDNO is sensitive and accurate revealing, that there is a trend for diminished nitric oxide production in the endothelium of the internal mammary artery bypass graft during extracorporeal circulation.
Data have been and are being collected from the four sampling sites in off pump cases, as well as in the angiography laboratory during coronarography. in order to obtain baseline NO2 levels for comparison with the presented data.

{kind=link}
{kind=link}