






Abstract
The global outbreak of Mycobacterium chimaera infections associated with heater-cooler devices (HCDs) presents several important, unique challenges for the infection prevention community. The primary focus of this article is to assist hospitals in establishing a rapid response for identification, notification, and evaluation of exposed patients, and management of HCDs with regard to placement and containment, environmental culturing, and disinfection.
We are in the midst of a global outbreak of infections due to Mycobacterium chimaera, a species in the Mycobacterium avium complex (MAC) [1–5]. The most serious infections have involved prosthetic valves, vascular grafts, and left ventricular assist devices (LVAD), and all have followed surgical procedures involving cardiopulmonary bypass [6–13]. These infections are associated with the production of M. chimaera–containing bioaerosols produced by the LivaNova (formerly Sorin) 3T heater-cooler device (HCD) [6, 8, 14]. These HCDs were most likely contaminated at the manufacturing facility, as water obtained from the pump assembly area harbored M. chimaera [15]. Whole-genome sequencing confirms that this is a common-source outbreak [15–18], with nearly identical isolates found in 3T HCDs and patients from multiple countries [16–18]. It is therefore likely that most 3T HCDs manufactured over the past decade are contaminated with the same M. chimaera strain [18], and that these contaminated HCDs have been and continue to be used globally [15]. HCDs made by other companies have been found to be contaminated with M. chimaera [10, 18], but have not been associated with the current outbreak [7, 8, 10, 12, 19, 20]. Other nontuberculous mycobacteria (NTM), such as M. abscessus, can contaminate HCDs [21], and the 3T HCD has been linked to other NTM infections [21].
When an M. chimaera–contaminated HCD is operating, the organism can be detected in air samples and on settle plates in the operating room (OR) [6, 8, 10, 14]. Prior work revealed that the concentration of mycobacteria in ejected water droplets is 1000- to 10000-fold higher than in the water itself [22]. When air bubbles in the HCD water tank reach the surface, they burst and water droplets are ejected into the air and escape through openings in the water circuit. The bioaerosol, with a particle size <1 µm, is released into the OR and disseminated via the cooling fans of the HCD, perhaps aided by turbulent air flow [6, 10]. Dissemination of this airborne inoculum results in contamination of the operative field (and/or the implant if it is exposed on the sterile field prior to implantation). This can lead to biofilm formation on an intravascular device, and subsequent dissemination of the infection [15].
The relatively low virulence and slow growth of M. chimaera present major challenges for case finding. Table 1 summarizes the clinical experience to date from the first 52 cases reported from the United States and Europe [7, 10, 13, 23]. Note that the earliest date of a surgery linked to the outbreak was 2008, and the longest period from surgery to clinical presentation has been 6 years [23]. Most cases followed prosthetic valve surgery, and all patients to date who have had the disseminated form of disease (involving liver, spleen, bone marrow, kidney, eye, bones, and joints) have had prosthetic material in place (valve, graft, or LVAD) [7, 10, 13]. Those infected after coronary artery bypass grafting only (no device implant) have had locally invasive infections (sternal wound, mediastinum or pleural space) without dissemination. Cases to date have presented with nonspecific symptoms, most commonly fatigue (90%), followed by fever (75%), sweats (60%), dyspnea (60%), weight loss (60%), and cough (50%) [13]. Histopathology demonstrates noncaseating granulomas in involved tissue, which are rarely smear-positive for acid-fast bacteria (AFB) [13]. Diagnosis has most often been made by AFB blood culture, though other sites (eg, bone marrow) are sometimes culture-positive in the setting of negative blood cultures [13], and polymerase chain reaction has also been valuable in some patients [7].
Clinical Experience for 52 Reported Cases of Heater-Cooler Device–Associated Mycobacterium chimaera Infection
| Patient Characteristics | No. |
|---|---|
| Total No. of cases | 52 |
| Earliest sentinel surgery | 2008 |
| Male, No. (%) | 43 (83) |
| Age, y, mean (range) | 60 (1–83) |
| Duration from surgery to clinical presentation, mo, mean (range) | 17 (1–72) |
| Site of index positive culturea | |
| Blood | 14 |
| Bone marrow | 5 |
| Cardiac tissue or device | 5 |
| Sternal wound | 3 |
| Pleural space | 3 |
| Liver | 2 |
| Urine | 2 |
| LVAD pocket | 1 |
| Presumed source | |
| Prosthetic valve or ring | 32 |
| Aortic graft | 9 |
| LVAD | 6 |
| Sternal wound | 5 |
| Crude mortality at time of publication of cases, No. (%) | 25 (48) |
| Patient Characteristics | No. |
|---|---|
| Total No. of cases | 52 |
| Earliest sentinel surgery | 2008 |
| Male, No. (%) | 43 (83) |
| Age, y, mean (range) | 60 (1–83) |
| Duration from surgery to clinical presentation, mo, mean (range) | 17 (1–72) |
| Site of index positive culturea | |
| Blood | 14 |
| Bone marrow | 5 |
| Cardiac tissue or device | 5 |
| Sternal wound | 3 |
| Pleural space | 3 |
| Liver | 2 |
| Urine | 2 |
| LVAD pocket | 1 |
| Presumed source | |
| Prosthetic valve or ring | 32 |
| Aortic graft | 9 |
| LVAD | 6 |
| Sternal wound | 5 |
| Crude mortality at time of publication of cases, No. (%) | 25 (48) |
Data are presented as No. unless otherwise indicated. Source: [7, 10, 13].
Abbreviation: LVAD, left ventricular assist device.
aOnly 2 case series had complete information (thus, total N = 35).
Clinical Experience for 52 Reported Cases of Heater-Cooler Device–Associated Mycobacterium chimaera Infection
| Patient Characteristics | No. |
|---|---|
| Total No. of cases | 52 |
| Earliest sentinel surgery | 2008 |
| Male, No. (%) | 43 (83) |
| Age, y, mean (range) | 60 (1–83) |
| Duration from surgery to clinical presentation, mo, mean (range) | 17 (1–72) |
| Site of index positive culturea | |
| Blood | 14 |
| Bone marrow | 5 |
| Cardiac tissue or device | 5 |
| Sternal wound | 3 |
| Pleural space | 3 |
| Liver | 2 |
| Urine | 2 |
| LVAD pocket | 1 |
| Presumed source | |
| Prosthetic valve or ring | 32 |
| Aortic graft | 9 |
| LVAD | 6 |
| Sternal wound | 5 |
| Crude mortality at time of publication of cases, No. (%) | 25 (48) |
| Patient Characteristics | No. |
|---|---|
| Total No. of cases | 52 |
| Earliest sentinel surgery | 2008 |
| Male, No. (%) | 43 (83) |
| Age, y, mean (range) | 60 (1–83) |
| Duration from surgery to clinical presentation, mo, mean (range) | 17 (1–72) |
| Site of index positive culturea | |
| Blood | 14 |
| Bone marrow | 5 |
| Cardiac tissue or device | 5 |
| Sternal wound | 3 |
| Pleural space | 3 |
| Liver | 2 |
| Urine | 2 |
| LVAD pocket | 1 |
| Presumed source | |
| Prosthetic valve or ring | 32 |
| Aortic graft | 9 |
| LVAD | 6 |
| Sternal wound | 5 |
| Crude mortality at time of publication of cases, No. (%) | 25 (48) |
Data are presented as No. unless otherwise indicated. Source: [7, 10, 13].
Abbreviation: LVAD, left ventricular assist device.
aOnly 2 case series had complete information (thus, total N = 35).
Optimal treatment of this infection has not been established, but typically involves combination antimicrobial therapy and, if possible, removal of involved prosthetic material [8–10, 12, 13]. In many cases, unfortunately, the patient is too sick or the procedure too high risk for explantation to be attempted [8–10, 12, 13], and there are no data available on the risk for reinfection of a newly placed device into the involved site.
Cases series to date report a very high crude mortality rate (approximately 50%) [7, 10, 13], and it is unknown whether the disseminated form of infection can be cured. Surviving patients include those with localized infections (eg, sternal wound infections) cured with debridement and antibiotics, and those with disseminated infection who remain unwell on treatment. A small number of patients who have had device removal in conjunction with antibiotics are in a postsurgical monitoring period (oral communication, April 2017) [24]. Thus, more clinical experience and longer follow-up are required to better delineate the attributable mortality and the impact of device removal on ability to cure the infection.
The primary roles for hospital epidemiologists and infection preventionists in management of this outbreak include identification and notification of exposed patients, assisting in logistics of medically evaluating exposed symptomatic patients, and mitigating the risk of transmission to prevent additional cases. Our recommendations are based on our experience at the University of Iowa Hospitals and Clinics, where we became aware of our first case of HCD-associated M. chimaera infection in January 2016.
DETERMINATION OF RISK
Any patient who underwent surgery while the LivaNova 3T HCD was running in the OR should be considered exposed and at risk for the development of M. chimaera infection. Thus, if any surgeries were performed with a functioning 3T HCD, case finding and risk mitigation should proceed. All 3T HCDs should be considered contaminated regardless of manufacture date or the results of HCD environmental cultures. Although the US Food and Drug Administration (FDA) reported that the manufacturer of the 3T HCD made changes in its cleaning and disinfection procedures in September 2014, some 3T devices manufactured after September 2014 have tested positive for M. chimaera [20]. The 3T HCD has been used since 2006, holds 60% of the market share, and is used in 200000 surgeries yearly in the United States [25], so the potential for exposure is significant. If a hospital detects a case, the risk of infection is currently estimated to be 1/100–1/1000 patients [19], but is likely variable based upon how centers use their HCDs, the types of surgery performed, cleaning protocols utilized, and the location and orientation of the HCD in the OR.
To date, the disseminated, high-mortality form of M. chimaera infection is limited to those with device implants (valve, graft, LVAD); however, CABG patients are at risk for invasive localized infections. Furthermore, some procedures (eg, transcatheter aortic valve replacement [TAVR], some liver and lung transplants) do not involve a sternotomy but are performed with the HCD running on “standby.” M. chimaera cases have occurred after TAVR, presumably due to contamination of the device prior to implantation, when it is exposed in the OR (on what is erroneously believed to be a sterile field). Until more is known, the Centers for Disease Control and Prevention (CDC) recommends considering all patients undergoing surgery with the HCD running to be exposed [26].
CASE FINDING AND COMMUNICATION
The first step in case finding is to develop a line list of exposed patients. The earliest reported date of surgery associated with a case in this outbreak is 2008 [7], and the 3T unit has been in use since 2006. It is therefore not known when exposure to the outbreak strain of M. chimaera began, but it was sometime between 2006 and 2008. Thus, patients exposed to a 3T HCD since that time should have M. chimaera infection in the differential diagnosis if they develop concerning signs or symptoms. The CDC recommends going back to 1 January 2012 for the purposes of notification, as almost all cases to date have developed manifestations of infection within 4 years [26]. Individual facilities may modify this date based on the time during which they used the 3T HCD, and they may decide to go back further—the longest period reported so far between surgery and clinical presentation is 6 years, so going back to 2010 would be more conservative, and back to 2006 would be the most comprehensive, recognizing that the yield for case detection will likely diminish the further back one goes. The period of exposure should extend until a definitive mitigation strategy (defined below) has been implemented.
HCDs are also used for extracorporeal membrane oxygenation (ECMO), although these HCDs have a different design with an air-tight, closed system. Mycobacterium chimaera strains have been detected in water samples from ECMO-associated HCDs, and this pathogen has grown in respiratory secretions from 3 of 118 ECMO patients at one center. However, on further investigation, the HCDs were not thought to have infected these patients [27]. Thus, notification of ECMO patients is not recommended.
Once the line list of exposed patients has been developed, patients should be individually contacted via closed loop communication. This can be accomplished by sending a letter of explanation requesting that the patient call the hospital for a telephonic symptom screen. Patients who report symptoms should be further evaluated. Some hospitals have established a dedicated clinic to evaluate these patients. Developing algorithms to determine the need for mycobacterial blood cultures can streamline and standardize the evaluation process. For patients who prefer local follow-up, a letter can be provided to the patient to present to the local physician, explaining the problem, symptoms, and an initial approach to clinical evaluation. Patients not responding to the initial letter should be contacted via another mechanism. At the time that patients are notified, press releases should be sent to media outlets, and a webpage for patients and medical professionals should be established with links to FDA and CDC materials [16, 19, 20], frequently asked questions, and contact information for patients to schedule appointments with expert providers. Clinician notification is an important facet of case finding. Letters should be sent to referring providers, and email communications sent to internal providers, with special emphasis on specialists who may encounter infected patients (infectious diseases, cardiology, cardiac surgery, hepatology, hematology/oncology, and ophthalmology). The CDC has developed a notification toolkit that provides templates for several of the above steps in patient and provider notification [26].
To assist in case identification, a lookback of laboratory records should be performed to identify cultures growing MAC in nonrespiratory tract specimens. Most laboratories only have the capacity to identify MAC to the “complex” level; species identification requires molecular approaches that are performed only at mycobacterial reference laboratories. This laboratory lookback list should then be compared to the list of exposed patients to identify any matches. The yield of this approach is unlikely to be high as mycobacterial blood cultures are rarely ordered for immunocompetent patients. In addition, patients with a diagnosis of sarcoidosis should be compared to the exposed patient line list as patients often present with a disseminated granulomatous process [6–9, 12] that may be incorrectly diagnosed as sarcoidosis [13].
Last, an electronic medical record decision support alert can be developed to notify clinicians when a patient with a history of cardiopulmonary bypass in the specified time frame develops fever or is diagnosed with a febrile condition (eg, fever of unknown origin). The alert can remind the clinician that the patient is at risk of M. chimaera infection and suggest that mycobacterial blood cultures be considered. The alert can also be sent to the hospital epidemiologist or an infectious disease physician who can review the chart to assess for risk of infection.
Case finding for HCD-associated M. chimaera infections is challenging for several reasons. Patients may not receive long-term follow-up at the hospital where the surgery was performed. The symptoms of the infection may be nonspecific, and the incubation period is long. Mycobacterial cultures are not typically performed in immunocompetent patients but are required for the diagnosis. The CDC has published interim case finding guidance that covers some of the above information [28].
Once cases are identified, they should be reported to the FDA [20] and public health departments [19]. At this time, a registry of cases does not exist, but is needed to further elucidate the epidemiology and better understand optimal treatment.
PATIENT EVALUATION
Exposed patients with symptoms consistent with M. chimaera infection should undergo evaluation. Mycobacterial cultures may be indicated for those with culture-negative endocarditis, prosthetic vascular graft infection, culture-negative sternal wound infection, mediastinitis, or disseminated infection, including embolic and immunologic manifestations (eg, splenomegaly, arthritis, osteomyelitis, cytopenias, chorioretinitis, lung involvement, hepatitis, nephritis, myocarditis, and elevated inflammatory markers) [9, 10, 12, 13, 15, 19, 28–30]. Additional indications for testing include fatigue, weight loss, fevers, night sweats, arthralgias, or myalgias [12, 13, 31].
Two or 3 mycobacterial blood cultures should be obtained if the patient has signs or symptoms of infection. If those are negative, consideration should be given to culture and histopathology of bone marrow and other affected organs or body sites, and additional blood cultures should be performed in 1–2 months. Early consultation with the clinical microbiology laboratory director should occur as the number of AFB blood cultures obtained could quickly exceed the capacity of the laboratory. For most hospitals, species identification and susceptibility testing will require submission to a reference laboratory. Mycobacterium chimaera grows slowly, and cultures may take 2–8 weeks to turn positive, with even greater delays to speciation. Molecular approaches to detection of M. chimaera are available in reference or research laboratories, but further development and wider availability of such testing are needed to help reduce time to detection.
RISK MITIGATION
Further work is needed to improve the design of HCDs and to establish effective infection prevention strategies. A definitive mitigation strategy requires separating the operative field from the 3T HCD exhaust bioaerosol. The most definitive option is to remove the HCD from the OR, though this may not be feasible for all facilities. We accomplished this via construction of a 6 × 6-inch portal in the OR wall covered by a sliding door to allow for passage of the HCD hoses through the wall to the HCD stationed outside the OR. Determination of the site for the portal should be guided by access to electrical power, safe corridor width, and minimal interference with staff and equipment. At the University of Iowa, these portals were constructed quickly and were fabricated of Corian or stainless steel (Figure 1). There was no demonstrable impact on positive air pressure or air exchange rates. A hose mat was placed inside each OR to protect the HCD hoses from equipment and provide a ramp effect for equipment to be relocated as needed. A cabled remote allows control of the HCD by the perfusionist in the OR with no impact on patient care or staff, and no difficulty with heating or cooling. Notably, Götting et al demonstrated that moving their HCD to an anteroom while leaving the door ajar to accommodate tubing failed to prevent detection of mycobacteria in OR air. This was resolved after they created a channel so that the OR door could close [14].
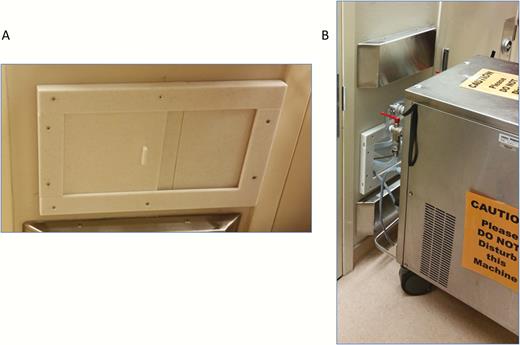
Heater-cooler device hose portals (A) were constructed in all operating rooms (ORs) where cardiopulmonary bypass is performed, with all heater-cooler units moved outside of ORs (B).
Another approach to bioaerosol containment is a custom-made housing for the HCD to ensure separation between the HCD exhaust and the OR air [32]. Smoke testing can be used as a crude verification of air separation [33]. If a definitive mitigation strategy cannot be implemented, HCDs should be oriented so that the exhaust is directed away from the patient. However, the utility of this strategy is unproven and may continue to place the patient at risk.
Mycobacterium chimaera and other NTM have been isolated from municipal water systems [34, 35], and resistance to disinfectants, such as chlorines and ozone, facilitates their persistence in water [36]. In fact, they are ≥1000 times more resistant to disinfectants than Escherichia coli, the industry standard for disinfection. Disinfectant resistance is due to a lipid-rich outer membrane that serves as a hydrophobic barrier, and the production of thick organism-rich biofilms [37].
The resistance to disinfectants and biofilm formation make decontamination of HCDs extremely difficult, if not impossible [14, 32, 37]. Contamination of brand-new 3T HCDs direct from the factory is quickly detectable [8, 15], and multiple cycles of decontamination fail to eliminate M. chimaera [14], as biofilm covering the walls and tubing remains [37]. Once biofilm formation has developed, decontamination can reduce but not completely remove it [14].
Manufacturers’ recommendations for HCD maintenance should be followed [25]. Despite adherence to these recommendations for use of sterile or filtered water, and regular water circuit disinfection and tubing changes, M. chimaera contamination will persist for reasons outlined above. In fact, investigators using far more intensive attempts at disinfection [32, 38] have been unable to eradicate M. chimaera from 3T HCDs [32]. Peracetic acid and removal of all biofilm-coated tubing is needed to suppress M. chimaera levels to below detection [38]; however, a method that consistently decontaminates HCDs has not been demonstrated. Thus, as currently designed, the 3T HCD cannot be safely operated unless exhaust air is physically separated from OR air.
There are several reasons why we recommend against routine sampling of HCD water and air for mycobacteria. First, the performance characteristics of such cultures are not known. Moreover, the fact that cultures from the same HCD will often alternate between positive and negative over time with repeat culturing suggests that negative cultures do not indicate that the HCD is free of mycobacteria (and thus may be falsely reassuring) [32]. Second, few microbiology laboratories have the capability to perform mycobacterial environmental cultures properly. One center sent water samples from the same HCDs to 2 laboratories, one of which found all samples to contain M. chimaera, the other of which reported all results to be negative (oral communication, October 2016). Third, culture results take up to 8 weeks to return, and thus are not particularly “actionable” even if they were thought to have good positive or negative predictive value (which is not established). Thus, the safest strategy is to consider all 3T HCDs to be contaminated.
CONCLUSIONS
This review summarizes a practical approach to communication, case finding, and risk mitigation for the HCD-associated M. chimaera outbreak. Point-source contamination of HCDs with M. chimaera represents a “perfect storm” for a slowly developing, difficult-to-detect global outbreak. Consequently, many patients are at risk for M. chimaera infection due to exposure to bioaerosols produced by HCDs used globally in cardiothoracic surgery. There is currently no evidence to define a lower threshold of mycobacterial contamination in air or water samples for preventing M. chimaera infection. Thus, the most important control measure currently is to remove HCDs from the OR until new HCD designs are available that prevent bioaerosol production.
Note
Potential conflicts of interest. All authors: No reported conflicts of interest. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.


{kind=link}