





Abstract
The suspensory ligamentous system of the penis supports the penis when erect and plays a key role during coitus. These ligaments, which are prone to injury during coitus, are clinically important in penile reconstruction procedures.
The current study investigated the macro- and microanatomy of the suspensory ligamentous system of the penis to determine the origin, course, insertion, dimensions, and tissue composition of these ligaments, knowledge of which is vital for successful penile reconstruction procedures.
The study utilized a total of 49 cadavers. Gross anatomy dissection, MRI, and histological staining were performed to elucidate the topography, dimensions, and tissue composition of the suspensory ligaments of the penis.
Three ligaments were observed to form the suspensory ligamentous system of the penis. The most superficial is the fundiform ligament, which consists of superficial bundles and deep median bundles, with the former arising from the Scarpa's fascia and the latter arising from the linea alba of the anterior abdominal wall; both inserted into the superficial fascia of the penis. The suspensory ligament of the penis arose from the pubic symphysis and inserted into the deep fascia (Buck's fascia) of the penis. The arcuate ligament arose from the body of the pubis and pubic symphysis and inserted into the Buck's fascia. The ligaments were determined to consist of adipose tissue, collagen fibers, elastic fibers and reticular fibers, in varying proportions.
The suspensory ligaments of the penis exhibit a fan-like structure on the penis that allows the forward movement of the penis as a result of engorgement of the erectile bodies while simultaneously offering support.

The suspensory penile ligament (SPL, often referred to as the suspensory penile ligament proper) forms part of a system of ligaments that support the penis in its flaccid and erect positions in the prepubic region.1-5 The suspensory ligamentous system of the penis consists of 3 distinct ligaments: the SPL, the fundiform ligament of the penis, and the arcuate pubic ligament.1-4,6 This system of ligaments helps to support the erect penis at an angle of approximately 30° anterior to the pubic region and also aids in penetration during coitus.3,4,7 The most important of these sets of ligaments is the SPL which facilitates penetration during sexual intercourse; thus, abnormalities of this ligament are associated with erectile dysfunction and poor coitus with the penis requiring manual assistance.4,7-9 Perceived disorders of the SPL are common in patients suffering from body dysmorphic disorder who present with a persistent preoccupation with an imagined defect in physical appearance that often causes clinically significant stress and depression.2
Clinically the SPL is important in penile plastic reconstruction surgery, such as penis-lengthening procedures in patients with small penises, penile dysmorphic disorders, and congenital penile disorders, all of which involve resectioning this ligament.2,10 The SPL is also vulnerable to trauma during sexual intercourse, leading to penile instability and erectile dysfunction.3,7 Penile instability can be caused by congenital absence of the SPL, congenital curvature of the penis, and iatrogenesis during surgery, particularly traditional surgical practices involving male circumcision.2,3,11,12 Despite the importance of the suspensory ligamentous system of the penis in maintaining the functional stability of the penis, very few studies have characterized the anatomy of this system and the available information is elusive. First, there is no consensus on the number, origin, and attachments of the fundiform ligament and the SPL.1,4,13 For example, the origin of the fundiform ligament has been described as either the linea alba or as a continuation of the superficial fascia of the anterior abdominal wall (Scarpa's fascia)4,14 and its insertion has been described as either the deep fascia of the penis (Buck's fascia) or the tunica albuginea.1,15 The same controversy surrounds the SPL, particularly its association with the pubic symphysis and its spatial relation with the dorsal neurovasculature of the penis.1,4,5,13 Second, there is little information about the histological structure of the suspensory ligamentous system, with the available studies being inconclusive.1 These inadequacies may lead to confusion during surgery of the region, resulting in a poor prognosis. The purpose of the current study was to investigate the detailed the macro- and microanatomy of the suspensory ligament system of the penis to enable surgeons to accurately design corrective surgical techniques for this structure and improve patient outcomes.
METHODS
The current study utilized 3 different methods to decipher the macro- and microanatomical structure of the penile suspensory ligamentous system as follows: gross anatomy dissection and morphometry to determine the origin, course, insertion, and dimensions of the 3 divisions of the suspensory ligaments; histology to determine the tissue composition of each division of the suspensory ligamentous system; and MRI to elucidate the presentation of the suspensory ligaments in situ, augmenting gross dissection. The cadavers used in the study were obtained from the School of Anatomical Sciences at the University of the Witwatersrand (Johannesburg, South Africa), and were donated for academic teaching and research purposes. All cadavers were handled and utilized in accordance with ethics requirements of the University of the Witwatersrand (ethics clearance number W-CJ-140604-1). The study was carried out between September 27, 2018 and October 10, 2019.
Dissection and Morphometry of the Penile Suspensory Ligaments
The study utilized 49 adult male cadavers: 26 out of the 49 cadavers had intact (undissected) pelvic regions, while the remaining 23 cadavers had the pelvic region predissected by undergraduate medical students. Standard dissection procedures of the male perineum were followed according to Grant's Dissector.16 Briefly, a T-shaped incision was made in the pubic region as follows: a superior horizontal incision was made along the pubic region similar to the Pfannenstiel-Kerr incision. A vertical incision was made perpendicular to the Pfannenstiel-Kerr incision, extending down to the dorsal surface of the penis. The skin of the pubic region was reflected laterally on both sides, followed by the removal of fat and superficial fascia to reveal the suspensory ligaments. Caution was exercised not to cut any fibrous tissues. Once the ligaments were exposed, their origin, course, and insertion were thoroughly examined. Due to the topographic positioning of the suspensory penile ligamentous system of the penis, the fundiform ligament was examined first followed by the SPL. Images were taken with a Nikon D3400 camera. All metric measurements of the fundiform ligament were taken with sliding Vernier calipers; the SPL dimensions were measured with both string and sliding Vernier calipers. The various measurements of the penile ligaments were taken as described below (see also Figure 1A, B):
Total length of the left superficial bundle of the fundiform ligament (TL-SBFL): distance from the origin of the fundiform ligament (anterior abdominal wall) to the first point of insertion on the penile shaft on the left side.
Total length of the right superficial bundle of the fundiform ligament (TR-SBFL): distance from the origin of the fundiform ligament (anterior abdominal wall) to the first point of insertion on the penile shaft on the right side.
Total length of the deep median bundle of the fundiform ligament (TL-DMBFL): distance from the origin of the DMBFL on the linear alba to the first point of insertion on the penile shaft on the middle.
Total width of the DMBFL (TW-DMBFL): distance at the origin of the DMBFL on the linear alba from the extreme left point to the extreme right point.
Total length of the SPL (TL-SPL): distance of the SPL ligament from the most posterior point of insertion to the free-end of the SPL (along the shaft of the penis) on the dorsum of the penis.
Total height of SPL (TH-SPL): distance from the highest point of origin of the SPL on the pubic symphysis to the most anterior point of insertion of the SPL on the dorsum of the penis.
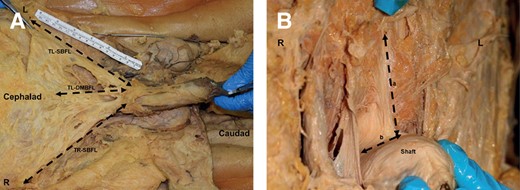
Photographs showing the measurements taken on the suspensory ligaments of the penis. (A) Dimensions of the fundiform ligament: TL-SBFL (total length of the left superficial bundle of the fundiform ligament), TR-SBFL (total length of the right superficial bundle of the fundiform ligament), and TL-DMBFL (total length of the deep median bundle of the fundiform ligament). (B) Dimensions of the suspensory ligament proper: a, height; b, length. L, left side; R, right side.
MRI Analysis of the Suspensory Ligamentous System of the Penis
Two additional adult male cadavers had their perineal regions harvested en bloc, including the root and shaft of the penis. The en bloc specimens were analyzed with an MRI scanner (Siemens Avanto Fit 1.5T) equipped with Syngo software v. II. The specimens were scanned in a 15-channel knee coil with oil marker placed on the left side for specimen A and on the right side for specimen B for orientation purposes. The en bloc sections were scanned at T1, T2 and T3 weighted volumetric interpolated breath-hold examinations in both coronary and sagittal planes. Section thickness was set at 1 mm and field-of-view at 180 mm from the specimens. MRI allowed for the visualization of the DMBFL, the SPL, and the arcuate ligament, making it possible to trace the points of origin and insertion.
Histological Staining and Analysis of the Suspensory Ligamentous System of the Penis
Tissue samples were harvested from the SBFL, the DMBFL, and the SPL from 7 cadavers selected from the dissected cohort as described in the previous section. The harvested ligaments were stored in 10% formaldehyde solution and processed for the following histological stains: hematoxylin and eosin stain for general anatomic orientation and adipose tissue content; Masson's trichrome stain for collagen fibers; Gordon's sweet silver stain for reticular fibers; and Verhoeff's modified stain for elastic fibers. Tissue blocks were serially sectioned at 5 µm thickness in a 1 in 4 series and all sections were stained following standard histological procedures. From each stained section, 10 random camera fields at ×10 magnification were acquired with a high-definition video camera (AxioCam HRC) linked to a compound microscope (Zeiss Axioscope). Composite images were prepared with CorelDraw X7 software v. 13 (Corel Corporation, Ottawa, Canada). No pixelation adjustments of the captured photomicrographs were undertaken except for adjustment of contrast and brightness.
The percentage composition of collagen, elastic, reticular, and adipose tissues in each ligament were estimated from the photomicrographs by means of the point-counting plugin of ImageJ software. The area (A) and area fraction (Afraction) occupied by each of the components were calculated as follows:
where ap = area per point (0.007 mm2) and ∑p = the sum of points falling over the tissue of the component of interest;
where Acamera field is the total area of the camera field at ×10 (0.60 mm2).
Data Analysis
All metric measurements were recorded on Excel spreadsheets and all descriptive statistics, such as mean and range, were calculated. A Shapiro-Wilk test was used to test for the normality of the data. A t-test was used to compare the left and right means. An analysis of variance was used to compare different mean tissue compositions (collagen, elastic, reticular fibers, and adipose tissue) of each ligament (SBFL, DMBFL, SPL). These tests were performed with R statistical software. P = .05 was taken as the level of statistical significance.
RESULTS
Visualization of the Fundiform Ligament
The fundiform ligament is the most superficial element of the penile suspensory ligamentous system and was the first ligament to be observed and described. The fundiform ligament consists of 3 distinct fiber bundles: 2 superficially placed lateral bundles, the left and right SBFLs, and a median but deep bundle, referred to here as the DMBFL (Figure 2A-C). The fundiform ligament was observed deep to the fatty layer (Camper's fascia) of the anterior abdominal wall. The superficial bundles of the fundiform ligament are thick and more fibrous distally towards the dorsum of the penis but very thin and wide superiorly as they fuse with the membranous fascial layer (Scarpa's fascia) of the anterior abdominal wall. At their most lateral extremities, the SBFLs appear more fatty than fibrous. As the SBFLs extend medially and down towards the shaft of the penis, they thicken and become tougher and more fibrous, matching in consistency with that of the DMBFL. The posterior fibers of the SBFLs on each side fuse with the left and right split bundles of the DMBFL. The DMBFL arises from the linea alba of the anterior abdominal wall and extends inferiorly towards the dorsum of the shaft of the penis (Figure 2C). It is fibro-fatty in appearance, shorter than the SBFL, and lies deep to the membranous fascial layer of the anterior abdominal wall. As it extends inferiorly, it splits into left and right bundles before fusing with the corresponding lateral bundles of the SBFL. The left and right fiber bundles of the DMBFL encircle the base of the penis, sending some fibers to insert into the superficial fascia of the penis directly superficial to the Buck's fascia (Figure 2C). The superficial dorsal vein lies immediately deep to the superficial fascia of the penis and the insertion of the fundiform ligament (both SBFL and DMBFL divisions) in the shaft of the penis (Figure 2D). From the anterior view the anterior fibers of the DMBFL resemble an inverted “V” as they split to encircle the penis shaft (Figure 3A, B). After encircling the base of the penis, the majority of the DMBFL fibers, together with the SBFL fibers, extend inferiorly into the scrotum, forming the origin of the scrotal raphe septum (part of the dartos fascia) in the midline (Figure 2A). On MRI scans, the orientation of the DMBFL was further revealed in both coronal and sagittal planes. The DMBFL was traced from superficial to deep and in both planes but its origin fell outside the view of the MRI scans because the en bloc specimens were cut along the superior edge of the pubic symphysis (this plane is below the origin of the DMBFL on the linear alba), but its insertion was clearly discernible. In superficial coronal slices, the DMBFL appeared as a thick and broad ligament that descended towards the dorsal surface of the shaft of the penis (Figure 4A, B). Further posteriorly (deeper layers), the DMBFL split to resemble an inverted “V” shape that encircled the 3 erectile bodies of the penis and the superficial dorsal vein directly superficial to the Buck's fascia (Figure 4C).
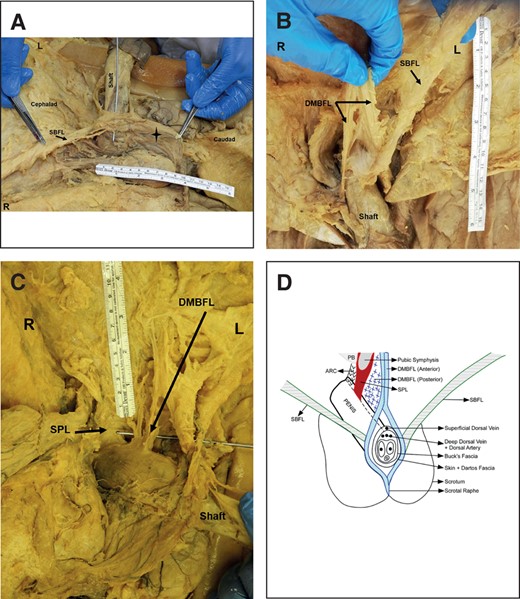
Orientation and topography of the suspensory ligaments of the penis. (A) The SBFL forms a sling around the shaft of the penis and continues into the scrotum as the median raphe ligament (star). (B) The anterior fibers of the DMBFL split into right and left bundles surrounding the penile shaft. (C) The DMBFL splits into anterior and posterior fiber bundles with the anterior fiber bundles fusing the SBFL and the posterior fiber bundle inserting into the deep fascia of the dorsum of the penis, respectively. (D) The topography and divisions of the suspensory ligament complex of the penis. ARC, arcuate ligament; DMBFL, deep median bundle of the fundiform ligament; L, left side; PB, pubic bone; SBFL, superficial bundle of the fundiform ligament; SPL, suspensory penile ligament; R, right side.

Photographs showing the DMBFL and the SPL. (A) Right split half of the DMBFL and the SPL. (B) Splitting of the DMBFL and midline and deep SPL. DMBFL, deep median bundle of the fundiform ligament; L, left side; R, right side; SPL, suspensory penile ligament.
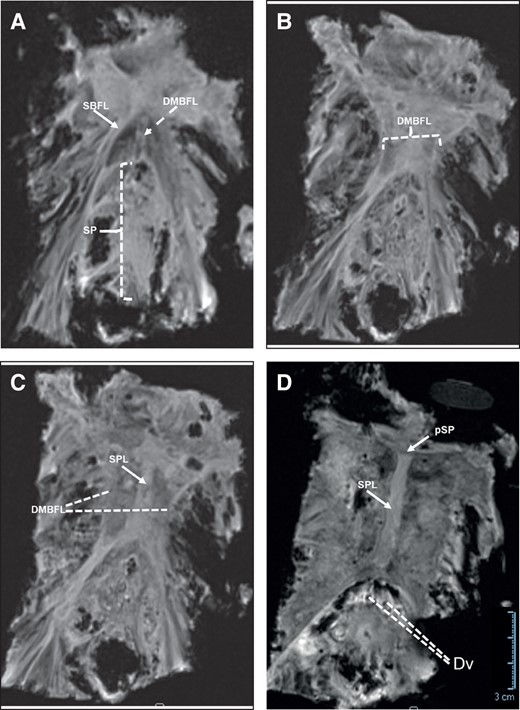
MRI showing a series of coronal plane images of the suspensory ligament system of the penis from superficial to deep (anterior to posterior in anatomical terminology) (A-D). (A) The distal portions of the fundiform ligament showing the SBFL (laterally) and the DMBF (midline) inserting on and encircling the penile shaft (SP). (B) The spread of the DMBFL. (C) The DMBFL splits towards the penile shaft and the SPL (midline) fuses with the fascia of the penis. (D) The SPL arises from the perichondrium of the pubic symphysis and inserts on the deep fascia of the penis (Buck's fascia) above the deep dorsal vasculature of the penis. DMFBL, deep median bundle of the fundiform ligament; Dv, deep dorsal vasculature; pSP, perichondrium of the pubic symphysis; SPL, suspensory penile ligament; SBFL, superficial bundle of the fundiform ligament; SP, penile shaft. Scale bar = 3 cm in (D) applies to all images.
The mean [standard deviation] TL-SBFL and TR-SBFL were 14.3 [1.3] cm and 15.0 [1.7] cm, respectively. There was no statistically significant difference between the TL-SBFL and TR-SBFL (P = .14). The mean TL-DMBFL was 8.5 [1.8] cm and the mean TW-DMBFL was 3.1 [0.8] cm at its origin.
Visualization of the Suspensory Penile Ligament (SPL)
The SPL was observed deeper (anatomically posterior) to the DMBFL and it presented with a tough fibro-fatty consistency throughout. It arises from the anterior edge of the pubic symphysis, extending inferiorly down to its lower border. Its course follows a short distance to reach the dorsum of the penile shaft. Its fibers encircle the shaft of the penis, but at a deeper level than those of the fundiform ligament, adhering tightly with the deep facial layer of the penis (Buck's fascia) (Figure 3A, B). Insertion of the SPL to the Buck's fascia is above (superior to) the deep dorsal veins and the dorsal artery of penis but deeper to the superficial dorsal vein which lies in the superficial fascia (Figure 2D). On MRI scans, the origin of the SPL was directly associated with the perichondrium of the pubic symphysis as seen in both coronal and sagittal planes (Figure 4D). In the coronal plane the ligament descended in the median plane and fused with the Buck's fascia on the dorsum of the penis (Figure 4D). The SPL together with posterior fibers of the DMBFL encircled the penile shaft intimately, fusing with the Buck's fascia. Insertion into the Buck's fascia can be confirmed by the location of the dorsal arteries and the deep dorsal vein of the penis which lies deep to this fascia (Figure 4D). The mean TH-SPL was 2.6 [0.8] cm and the mean TL-SPL was 5.08 [1.1] cm.
Visualization of the Arcuate Ligament
Due to its deeper and restricted location, the arcuate ligament was only visualized on the MRI scans. In the coronal plane, the arcuate ligament appeared as an arched bridge above the erectile bodies of the root of the penis (Figure 5A-C). In more superficial sections, the arcuate ligament fuses with the posterior fibers/portion of the SPL (Figure 5A). In the sagittal plane, the arcuate ligament appeared to originate from the lower margins of pubic arch, including the inferior surfaces of the right and left pubic bodies and the pubic symphysis, and inserts on the Buck's fascia similar to the insertion of the SPL (Figure 5D, E).
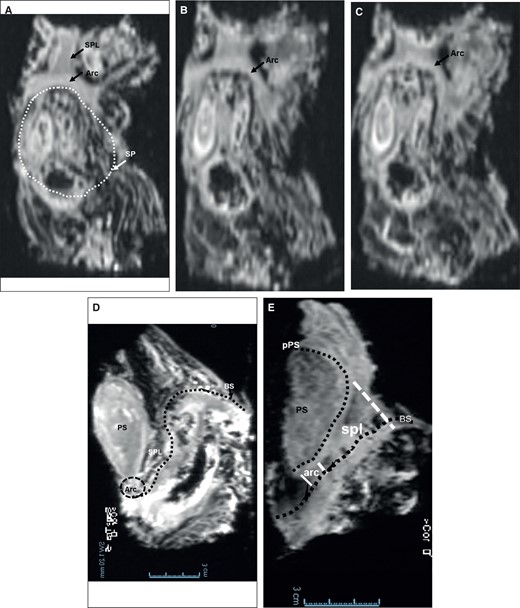
MRI showing a series of coronal plane images of the arcuate ligament from superficial to deep (anterior to posterior in anatomical terminology) (A-C) and the sagittal plane images of both the SPL and the arcuate ligament. (D, C). (A) The SPL and the arcuate ligament appear to fuse above the penile shaft (SP). (B, C) The arcuate ligament above the erectile bodies (root/shaft) of the penis. (D, E) The SPL and the arcuate ligament in the sagittal plane showing their proximal origins from the perichondrium of the pubic symphysis and distal insertions on the Buck's fascia of the penis. Arc, arcuate ligament; BS, Buck's fascia; PS, pubic symphysis; pPS, perichondrium of the pubic symphysis; SPL, suspensory penile ligament; SP, penile shaft. Scale bar = 3 cm in (D, E) applies to all images.
Microanatomic Examination of the Suspensory Ligamentous System of the Penis
All the ligaments examined were composed of varying amounts of adipose tissue and connective tissue fibers (collagen, elastic, and reticular). The mean percentage area fraction (composition) of adipose tissue showed statistically significant differences among the SBFL (53% [2.55%]), DMBFL (43% [2.02%]), and SPL (53% [1.78%]) (F = 45.48; P < .05). The mean percentage area fraction of adipose tissue was lower in the DMBFL than in the SBFL and SPL (P ≤ .05), while there was no statistically significant difference between the SBFL and SPL (P ≥ .05) (Figure 6A-D).
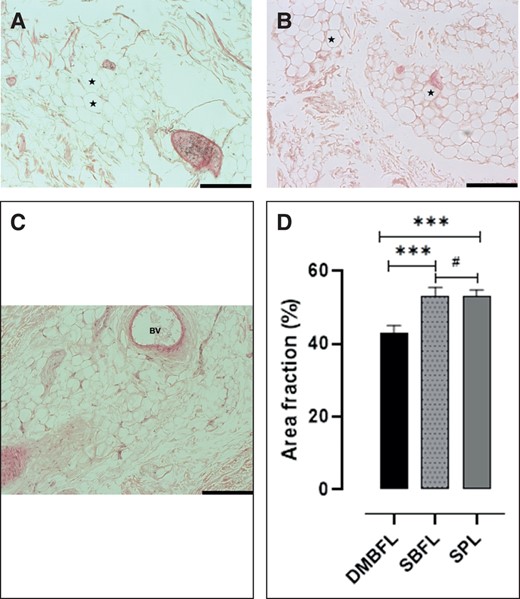
(A-C) The adipose tissue composition in hematoxylin and eosin–stained divisions of the suspensory ligament system of the penis. (A) The adipose tissue composition of the DMBFL. (B) The adipose tissue composition of the SBFL. (C) The adipose tissue composition of the SPL. (D) Bar graph showing the composition of the adipose tissue of each division of the suspensory ligament of the penis. ***Significant difference (P ≤ .05); #no significant difference (P ≥ .05). *Adipocytes. BV, blood vessels; DMBFL, deep median bundle of the fundiform ligament; SBFL, superficial bundle of the fundiform ligament; SPL, suspensory penile ligament. Scale bar =50 µm applies to (A-C).
The mean percentage area fraction of collagen fibers showed statistically significant differences among the SBFL (21% [1.79%]), DMBFL (43% [1.6%]), and SPL (23% [1.35%]) (F = 398.3; P < .05). The mean percentage area fraction of collagen fibers was higher in the DMBFL than in the SBFL and SPL (P < .05). There was no statistically significant difference between the collagen fiber content of the SBFL and SPL (P ≥ .05) (Figure 7A-D).
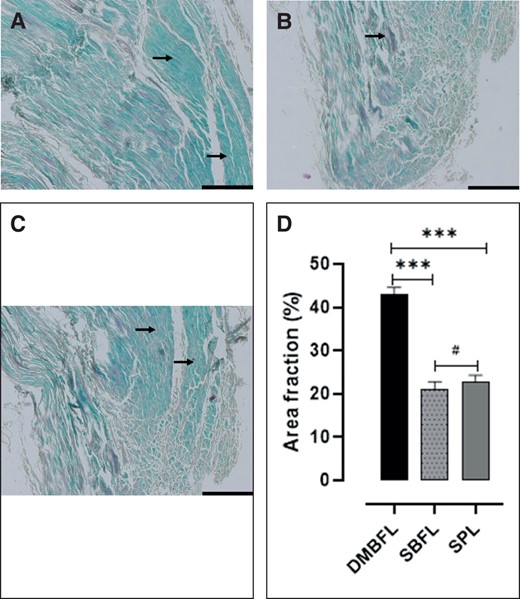
(A-C) The collagen fiber composition of the Masson's trichrome–stained divisions of the suspensory ligament system of the penis. (A) The collagen fiber composition of the DMBFL. (B) The collagen fiber composition of the SBFL. (C) The collagen fiber composition of the SPL. (D) Bar graph showing the composition of the collagen fibers of each division of the suspensory ligament of the penis. ***Significant difference (P ≤ .05); #no significant difference (P ≥ .05). DMBFL, deep median bundle of the fundiform ligament; SBFL, superficial bundle of the fundiform ligament; SPL, suspensory penile ligament. Arrows = collagen fibers. Scale bar = 50 µm applies to (A-C).
The mean percentage area fraction of elastic fibers showed statistically significant differences among the SBFL (23% [0.35%]), DMBFL (13% [0.67%]), and SPL (23% [0.82%]) (F = 559.1; P < .05). The mean percentage area fraction of elastic fibers was lower in the DMBFL than in the SBFL and SPL, but there was no statistically significant difference between the elastic fiber content of the SBFL and SPL (P ≥ .05) (Figure 8A-D).
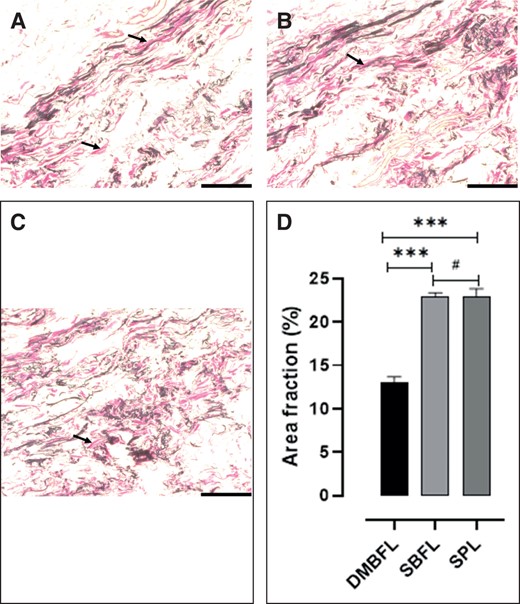
(A-C) The elastic fiber composition of the Verhoeff's elastic–stained divisions of the suspensory ligament system of the penis. (A) The elastic fiber composition of the DMBFL. (B) The elastic fiber composition of the SBFL. (C) The elastic fiber composition of the SPL. (D) Bar graph showing the composition of the elastic fibers of each division of the SPL. ***Significant difference (P ≤ .05); #no significant difference (P ≥ .05). DMBFL, deep median bundle of the fundiform ligament; SBFL, superficial bundle of the fundiform ligament; SPL, suspensory penile ligament Scale bar =50 µm applies to (A, B and C).
Reticular fibers were found mostly as a thin layer of fibers supporting adipocytes in the adipose tissues. The mean percentage area fraction of reticular fibers was comparable across all the DMBFL (13% [3.14%]), SBFL (14% [3.96%]), and SPL (12% [3.29%]) (F = 14.83; P > .05). There was no statistically difference in the mean percentage area fraction of the reticular fibers across all ligaments (P ≥ .05) (Figure 9A-D).
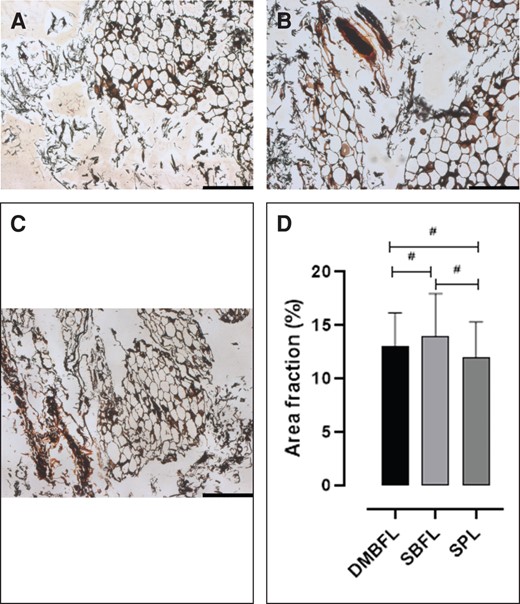
(A-C) The reticular fiber composition of the silver-stained divisions of the suspensory ligament system of the penis. (A) The reticular fiber composition of the DMBFL. (B) The reticular fiber composition of the SBFL. (C) The reticular fiber composition of the SPL. (D) Bar graph showing the composition of the reticular fibers of each division of the suspensory ligament of the penis. #No significant difference (P ≥ .05); *adipocytes within the meshwork of reticular fibers. DMBFL, deep median bundle of the fundiform ligament; SBFL, superficial bundle of the fundiform ligament; SPL, suspensory penile ligament. Scale bar = 50 µm applies to (A-C).
DISCUSSION
The suspensory ligamentous system of the penis is important for elevating and supporting the penis during coitus. The function of the penis and its aesthetic value plays a crucial role in psychological perceptions held by men, especially regarding size. Perceptions of penile size have led to body dysmorphic disorders whereby men perceive their penis as small despite it being of normal size.3 The suspensory ligaments of the penis have been described previously in a few studies,1,4,13 and more recently,5 but there is no consensus on the exact number, origin, course, and insertion points of each ligament. In addition, the histological compositions of the penile ligamentous system have not been fully characterized. Hence the current study examined the macro- and microanatomy of the suspensory ligamentous system of the penis to determine the origin, course, and insertion, and also their tissue composition. The fan-like structure of the ligaments has been shown and clearly confirms the forward movement of the ligament, enabling lengthening of the penis during erection, and retraction during relaxation, while maintaining stability and support of the penis through the attachment to the symphysis pubis and Scarpa's fascia and other anterior abdominal wall structures.
The Fundiform Ligament
The fundiform ligament is the most superficial of the 3 suspensory ligaments. Apart from its topography, the sites of origin from the anterior abdominal wall and insertion on the penile shaft are contentious. In addition, its histological composition is largely unknown. Information about its structure will help towards understanding of the suspensory mechanism of the penis and the associated penile lengthening procedures.
The fundiform ligament has been observed to originate from the Scarpa's fascial layer of the anterolateral abdominal wall,4 but classic anatomy textbooks describe it as arising from the linea alba.17,18 In the current study, the fundiform ligament presented with 2 fiber bundles, the SBFL and the DMBFL. The SBFL is paired and lies on the lateral edges of the lower part of the anterior abdominal wall, whereas the DMBFL lies medial along the midline of the lower part of the anterior abdominal wall. The SBFL was found to be a thickening of fibers arising from the Scarpa's fascia and descends inferomedially towards the penile shaft on each side, while the DMBFL arose from the linear alba on the anterior abdominal wall. The origin and course of the divisions of the fundiform ligament observed in the current study concur with previous studies.1,4 The DMBFL descended along the midline towards the shaft of the penis and split into right and left fiber bundles that encircled the shaft of the penis superficial to the deep fascia of the penis (Buck's fascia). The superficial fascia (Colles's fascia) of the penis lies directly superficial to the deep fascia of the penis and extends into the scrotum, fusing with the fascia of the scrotum (Dartos’s fascia).17,18 The anterior fibers of the DMBFL from the left and right split bundles fuse with the superficial fascia of penis as they insert on the shaft of the penis. However, as evidenced by the MRI scans, the posterior fibers of the DMBFL fuse with the posteriorly located SPL fibers and insert together on the deep fascia of the penis (Buck's fascia). Therefore, the posterior fibers of the DMBFL may be classified as an extension of the SPL anteriorly, while its anterior portion can be described together with the SBFL. This is because the merging of the left and right SBFL fibers to the left and right wings of the DMBFL, respectively, happens just before both bundles encircle the base of the shaft of the penis. In addition, the fused fibers (anterior DMBFL and SBFL) terminate collectively in the scrotal sac as the origin of the scrotal septum raphe. Previously, the fundiform ligament of the penis was observed to encircle the shaft of the penis and continue into the scrotal raphe.4 The identification of the 2 divisions of the fundiform ligament—the SBFL arising from the Scarpa's fascia and the DMBFL from the linea alba—clarifies previous misconceptions in the literature that state that “the fundiform ligament arises either from the Scarpa's fascia4 or from the linea alba of the abdominal wall.”1 In a recent study, Danino et al described the 4 ligaments of the penis and classified them into 2 classes: stabilizing ties (vertical dense ligament and arcuate ligament) and nonstabilizing ties (fundiform ligament and suspensory ligament).5 The observation of the 2 nonstabilizing ties by Danino et al in some way concurs with our observation of 2 divisions of the fundiform ligament (SBFL and DMBFL), but the terminology being used is different and puzzling, particularly regarding the suspensory ligament.5 However, Rees et al observed only a band of discrete fibrous tissue originating in the linea alba that continued down (ie, anatomically posteriorly) to attach to the dorsal surface of the base of penis and extend around the corpora.13 The fibrous band had superficial and deep components, with the superficial component having a width of 3 to 4 cm and a length of 7 to 8 cm along the penis. The deep component of the suspensory ligament was continuous with the deep fascia of the penis on its insertion and was just less than 1 cm in thickness. This observation corresponds with the description of the DMBFL and the SPL as identified in the current study but excludes the SBFL. According to Rees et al, the superficial component of the fundiform ligament (equivalent to the SBFL described herein) is present in females but absent in males and has a width of 7 to 8 cm and length of 8 to 9 cm from its origin to the clitoris. In the present study the SBFL showed a length of about 15 cm from origin to insertion and its origin was expansive on the anterolateral abdominal wall.
The histological findings of the current study on the origin and structure of the SBFL and DMBFL fibers complement the macroanatomic findings in that the SBFL showed considerably fewer (50% less) collagen fibers than that of the DMBFL. The SBFL arose from the membranous layer of fascia (Scarpe's fascia), and is less collagenous than the DMBFL, which arose from the linea alba—a tough fibrous band of tissue (with a high collagen content). In addition, the SBFL showed a higher proportion of adipose tissues than the DMBFL, further indicating that it originated from the fatty membranous structure of Scarpa's fascial layer of the anterior abdominal wall. However, Hoznek et al found the SPL to consist of only collagen fibers, possibly because their study did not include stains for a range of connective tissue types.1 Therefore, it can be deduced that the DMBFL is more important as a suspensory ligament to the penis than the SBFL.
The SPL
The SPL lies between the fundiform ligament anteriorly and the arcuate ligament posteriorly.1 In the current study, the results showed that the SPL originated from the anteroinferior edge of the pubic symphysis and arched inferiorly downwards (ie, anatomically posteriorly) towards the base of the shaft of the penis. The origin of the SPL from the pubic symphysis was further confirmed on the MRI scans where the ligament arose from the perichondrium of the pubic symphysis. These findings concurred with observations from previous studies.1,4 However, Danino et al observed a similar ligament to the canonical SPL and referred to it as a “vertical dense ligament” that participates in the stabilization of the penis.5 In the current study, the mean total height of the SPL was 2.6 [0.8] cm and the mean total length was 5.08 [1.1] cm. In a similar study, Hoznek et al showed that the length and width of the SPL were 3.7 [0.5] cm and 2.7 [0.8] cm, respectively.1 However, Wang et al reported a length range of 2 to 4 cm for the SPL.19
In the current study, the SPL was found to fuse and insert on the deep layer of the penile fascia (Buck's fascia) (Figure 4D). Similarly, an imaging study indicates that the SPL fuses with Buck's fascia and suggested that it carries the greater part of suspensory function of the penis.4 Furthermore, Rees et al described the deeper component of the suspensory ligament to arise from the pubic symphysis and insert through fusion with the Buck's fascia at the base of the shaft of penis.13 However, Hoznek et al concluded that the SPL had connections with the tunica albuginea of the cavernosa, suggesting that it inserts deeper to the Buck's fascia.1 On the other hand, the classic anatomy textbook describes the attachment vaguely as attaching to the fascia of the penis, without specifying whether it attaches to Colle's fascia, Buck's fascia, or the tunica albuginea.17 The SPL carries the greater part of the suspensory function of the penis and is crucial for successful coitus, and therefore is prone to injury during rough coital activities.7 During penile lengthening procedures the SPL is divided to release the penis from the pubic arch and pubic symphysis (Figure 10A-C). This procedure affords the penis some extra length, normally 2 cm, but this affects the control and movement of the penis during coitus. To spare this function of the SPL, the palmaris longus tendon can be used to bridge the gap between the cut edges of the SPL (Figure 10A). Alternatively, an inferiorly pedicled periosteal flap measuring approximately 2.5 cm by 2.5 cm is developed on the inferoanterior aspect of the symphysis pubis and fixed to the stump of the cut suspensory ligament, employing a similar principle to the above (Figure 10B). This maintains the anterior movement of the penis with retention of the fan-like arrangement of the suspensory ligaments (Figure 10C). Histologically the SPL consists of both fibrous material and adipose tissue. The SPL was found to consist of a higher percentage of elastic fibers, followed by adipose tissue and fewer collagen fibers.
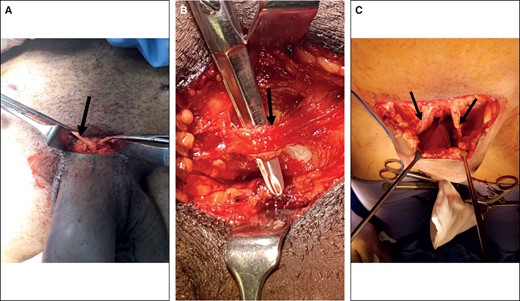
Intraoperative procedures during the division of the suspensory ligament system of the penis to correct a buried penis. (A) Extending the SPL by the palmaris longus tendon. The palmaris longus tendon (arrow) is tunneled beneath a symphysis pubis periosteum and through a hole in the stump of the suspensory ligament of the penis. (B) The development of the pubic symphysis flap (arrow) before division of the superior attachment to the perichondrium of the pubic symphysis to create an inferiorly pedicled flap. (C) The deep median bundle of the fundiform ligament (arrows) spared to provide the residual support for anterior movement of the penis required for an effective erection after fixation of the flap to the SPL. SPL, suspensory penile ligament.
The Arcuate Ligament
In the current study the arcuate ligament was only examined on MRI scans, and results showed it originates from the inferior edges of the pubic symphysis and inserts directly on the deep fascia of the penis (Buck's fascia) at the base of the penis. This finding was consistent with previous studies.1,4,5 In addition, the current findings showed, for the first time, that the arcuate ligament fused with the posterior fibers of the SPL. This fusion of the posterior fibers of the SPL to the arcuate ligaments suggests that the suspensory ligament system of the penis works as a unit in providing support to the erect penis and facilitating coitus.
Limitations of the Study
This study was performed on formaldehyde-fixed cadavers, limiting the understanding of the behavior of the suspensory ligament complex in unpreserved dynamic conditions such as erection.
CONCLUSIONS
This is the largest and most comprehensive study ever done on the macro- and microanatomy of the SPL, and provides detailed structural and topographic information of the suspensory ligamentous system of the penis. The information is crucial during the conceptualization and design of phalloplasty procedures—and any other procedures that implicate the suspensory ligamentous system of the penis—to improve the quality and accuracy of surgical procedures, and to produce better patient outcomes (eg, Figure 10A-C). Surgery based on the division of the SPL and the subpubic arcuate ligament component could be counterproductive to the stability of the penis during coitus. If the integrity of the suspensory ligament is violated during surgery, reconstruction may be mandatory.
Acknowledgments
The authors are grateful to the technical staff of the School of Anatomical Sciences at the University of the Witwatersrand (Johannesburg, South Africa) for their assistance during cadaver dissection and data collection. They also extend our gratitude to the MRI unit staff at Netcare Rosebank Hospital (Johannesburg, South Africa) for their assistance with MRI scanning and interpretation of images. Drs Mariani and Fayman made an equal contribution to this work as co–first authors.
Disclosures
The authors declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
Funding
The authors received no financial support for the research, authorship, and publication of this article.
REFERENCES
Author notes
Dr Mariani is a lecturer and Dr Ihunwo is a professor, School of Anatomical Sciences, University of the Witwatersrand, Parktown, Johannesburg, South Africa.
Dr Fayman is a plastic surgeon, Netcare Rosebank Hospital, Johannesburg, South Africa.
Dr Nkomozepi is an associate professor, Department of Human Anatomy and Physiology, Faculty of Health Sciences, University of Johannesburg, Johannesburg, South Africa.
Dr Mazengenya is an assistant professor, College of Medicine and the Center of Medical and Bio-allied Health Sciences Research, Ajman University, Ajman, United Arab Emirates.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}