





Abstract
Botulinum toxin-A (BTX-A) is used in the treatment of nasolabial folds (NLFs). However, lighting and clinician subjectivity play a major role in evaluating the efficacy of this treatment.
By applying 3-dimensional (3D) technology, this study aimed to quantitatively evaluate the effects of BTX-A injection on muscular (M) and muscle–fat pad mixed-type (MF) NLFs.
BTX-A was injected into bilateral marked points on the NLFs, where the levator labii alaeque nasi, zygomaticus minor, and zygomaticus major pull the skin to form the NLF (2 U at each injection site). Pretreatment and posttreatment 3D facial images were captured with static and laughing expressions. The curvature, width, depth, and lateral fat volume of the NLFs were measured to compare the therapeutic efficacy for type M and MF NLFs.
Thirty-nine patients with type M and 37 with type MF NLFs completed the follow-up data. In these patients, the curvature, width, and depth of the NLF showed a significant reduction at 1 month and gradually recovered at 3 and 6 months after treatment, with more significant improvement when laughing than when static. Variations compared to the pretreatment values of type MF were greater than those of type M at each time point. The lateral fat volume of the type MF NLF was significantly reduced (P < .05).
3D technology can quantitatively evaluate the effects BTX-A injection for treating type M and type MF NLFs. BTX-A is more effective on type MF than on type M NLFs.

The nasolabial fold (NLF) is a depressed facial area extending from the alar nasi region to the oral angle region.1 Depending on how it develops, the NLF can be categorized into the following types: skin, fat pad, muscular (M), muscle–fat pad mixed type (MF), and bone retrusion.2 However, the treatment methods for each type of NLF differ. Patients with skin-type NLFs have apparent sagging-related vertical wrinkles and which require facelift surgery to resolve.2 In fat-pad-type NLF patients, facial liposuction can be used.3 Bone-retrusion-type NLFs can be filled with hyaluronic acid4,5 and autologous fat.6 NLFs are dominated by muscular dynamic factors resulting from high tension of muscle contraction without hypertrophy of the fat pad.2 The fold deepens when standing up and laughing. In the supine position, the fold shows no apparent change in the absence of a thick fat pad compared with when standing up both in the static condition and when laughing. Botulinum toxin-A (BTX-A) injection treatment, which is simple to implement, has a rapid and remarkable effect.7-11 Moreover, studies have shown that BTX-A is the best treatment for type M NLFs.12-15 BTX-A inhibits acetylcholine release at the neuromuscular junction of the levator labii alaeque nasi (LLSAN), zygomaticus minor (Zmi), and zygomaticus major (Zmj) muscles involved in NLF composition,1,16 and thereby acts on the dynamic aspects of the NLF caused by excessive muscle contraction.13
In recent years, many methods have been proposed for evaluating nasolabial wrinkles, including photographic comparison and the Wrinkle Severity Rating Scale,17 among others. However, these methods depend on the subjective assessment of clinicians and are susceptible to lighting and body position.18 Artec Eva (Artec 3D; Senningerberg, Luxembourg) is a handheld and noninvasive 3-dimensional (3D) scanner that uses structured-light technology.19,20 The 3D facial imaging surfaces captured by Artec Eva show good accuracy, and this device has become a suitable option for facial surgery assessment.21-25 In the field of computer science, Rhino (Robert McNeel & Associates; Seattle, WA) and Matlab (MathWorks; Natick, MA) are the most popular tools for designing analytical symbols and numerical environments.26,27 They can perform 3D visual image processing with accurate measurement of the curvature, width, depth, and volume changes of 3D models.28-30 In this study, BTX-A injections were investigated in patients with type M and type MF NLFs. 3D measurement techniques were applied to quantify pretreatment and posttreatment NLF changes, including the curvature, width, depth, and lateral fat volume of the NLFs. Our study provides a new idea for 3D measurement and evaluates the efficacy of BTX-A treatment of NLFs. The effects of BTX-A on type M and MF NLFs were also compared.
METHODS
Patients
This study was approved by the IRB of the First Affiliated Hospital of Harbin Medical University and was performed according to the principles of the Declaration of Helsinki. Written informed consent was obtained from all patients. Following the clinical classification of Zhang et al, we formulated a type M and MF classification standard (Table 1).2 Between July 2018 and July 2021, we recruited patients with severe NLFs who were objectively evaluated and assigned to either the M or MF group by 3 plastic surgeons not involved in the study. The study included patients with type M and MF bilaterally symmetric NLFs. The enrolled patients consented to receive no other treatment for correction of the NLF during the study period. The exclusion criteria were as follows: (1) other types of NLF; (2) local skin infection with or without inflammation; (3) abnormal pretreatment examination; (4) history of BTX-A allergy; (5) history of NLF-related cosmetic surgery within the previous 6 months; (6) past history of cough variant asthma, neuromuscular disorder, or pregnancy, lactation, etc; and (7) incomplete data or insufficient follow-up.
Standards for Type M and Type MF NLFs
| Type | State | |||
|---|---|---|---|---|
| Standing upright and still (I) | Standing upright with laughing (II) | Laying supine and still (III) | Laying supine with laughing (VI) | |
| Fat pad | Thick fat pad; the NLF manifests as concave | Deepening of the concavity (+) | NLF becomes slightly shallower, but the concavity remains | NLF slightly shallower than in state II |
| Type M | High tension resulting from muscle contraction; the NLF displays as a deep furrow (+) | Deepening of the fold (++) | NLF shows no clear change (+) | NLF was no shallower than in state II (++) |
| Type MF | Combination of both muscular type and fat-pad type (++) | Deepening of the concavity (+++) | NLF becomes slightly shallower than in state I (+) | NLF becomes slightly shallower than in state II (++) |
| Type | State | |||
|---|---|---|---|---|
| Standing upright and still (I) | Standing upright with laughing (II) | Laying supine and still (III) | Laying supine with laughing (VI) | |
| Fat pad | Thick fat pad; the NLF manifests as concave | Deepening of the concavity (+) | NLF becomes slightly shallower, but the concavity remains | NLF slightly shallower than in state II |
| Type M | High tension resulting from muscle contraction; the NLF displays as a deep furrow (+) | Deepening of the fold (++) | NLF shows no clear change (+) | NLF was no shallower than in state II (++) |
| Type MF | Combination of both muscular type and fat-pad type (++) | Deepening of the concavity (+++) | NLF becomes slightly shallower than in state I (+) | NLF becomes slightly shallower than in state II (++) |
M, muscular type; MF, muscle–fat pad type; NLF, nasolabial fold.
Standards for Type M and Type MF NLFs
| Type | State | |||
|---|---|---|---|---|
| Standing upright and still (I) | Standing upright with laughing (II) | Laying supine and still (III) | Laying supine with laughing (VI) | |
| Fat pad | Thick fat pad; the NLF manifests as concave | Deepening of the concavity (+) | NLF becomes slightly shallower, but the concavity remains | NLF slightly shallower than in state II |
| Type M | High tension resulting from muscle contraction; the NLF displays as a deep furrow (+) | Deepening of the fold (++) | NLF shows no clear change (+) | NLF was no shallower than in state II (++) |
| Type MF | Combination of both muscular type and fat-pad type (++) | Deepening of the concavity (+++) | NLF becomes slightly shallower than in state I (+) | NLF becomes slightly shallower than in state II (++) |
| Type | State | |||
|---|---|---|---|---|
| Standing upright and still (I) | Standing upright with laughing (II) | Laying supine and still (III) | Laying supine with laughing (VI) | |
| Fat pad | Thick fat pad; the NLF manifests as concave | Deepening of the concavity (+) | NLF becomes slightly shallower, but the concavity remains | NLF slightly shallower than in state II |
| Type M | High tension resulting from muscle contraction; the NLF displays as a deep furrow (+) | Deepening of the fold (++) | NLF shows no clear change (+) | NLF was no shallower than in state II (++) |
| Type MF | Combination of both muscular type and fat-pad type (++) | Deepening of the concavity (+++) | NLF becomes slightly shallower than in state I (+) | NLF becomes slightly shallower than in state II (++) |
M, muscular type; MF, muscle–fat pad type; NLF, nasolabial fold.
While patients made static and laughing expressions, and were standing upright, photographs were taken with a digital camera (Nikon D90, Nikon; Minato, Tokyo, Japan)19 and then scanned by Artec Eva to generate 3D images. Photographs and 3D images of all patients were taken pretreatment, and at 1, 3, and 6 months after treatment for observation and data measurement. 3D data were measured and analyzed with Rhino and Matlab software.
Each patient completed an anonymous questionnaire 1 month after BTX-A treatment (the time point at which BTX-A is most effective), which asked the question: to what degree do you think the NLF has been improved. The question had the following 5 possible responses: very much improved, much improved, improved, no change, and worse. Complications of treatment were assessed by self-administered questionnaires. Patients were asked whether they had experienced any side effects, such as pain, swelling, edema, ecchymosis, delayed hypersensitivity reactions, or other adverse events immediately and on days 1, 7, 30, 90, and 180 after injection.
BTX-A Treatment for NLFs
Six injection points at bilateral NLFs were marked before treatment in the standing position19 (Figure 1). Points A1 and A2 were located at the junction between the alar base and the NLF, where the LLSAN pulled the beginning of the NLF while laughing. Points B1 and B2 were the positions where the Zmi pulled the middle portion of the NLF with the greatest tension while laughing. Points C1 and C2 were located at the junction between the region of the mouth corner and the NLF, where the Zmj pulled the NLF when laughing. All patients were placed in the supine position,31,32 and their chins were slightly raised. BTX-A (Botox; Allergan, Irvine, CA) was diluted with normal saline to make a 2 U/0.1 mL solution. Then, 2 U of the prepared BTX-A was injected with a 30-gauge needle into the superficial layer of muscle at each point. All the procedures were performed by the same surgeon. The patients were advised not to use hot compresses or massage the injected area during the first 2 weeks after injection. It was suggested that feedback be provided if there were any adverse reactions.
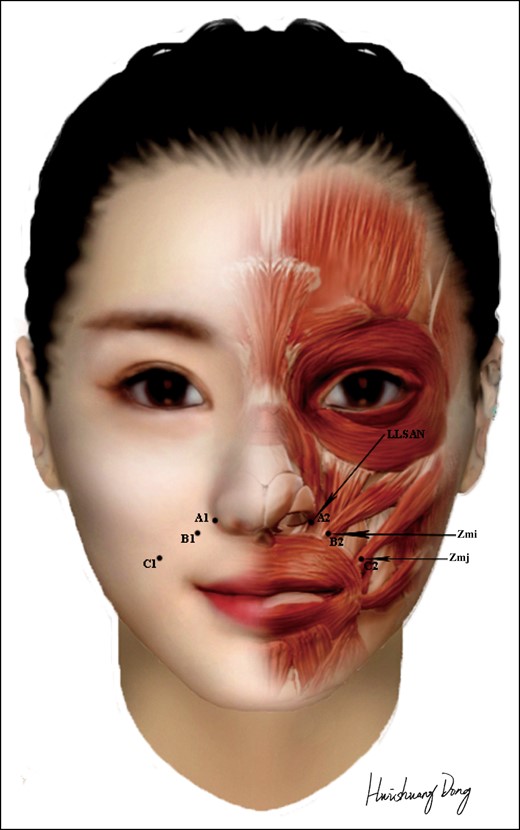
Marked points and injection sites of the nasolabial fold. LLSAN, levator labii alaeque nasi; Zmi, zygomaticus minor; Zmj, zygomaticus major. Created by and published with permission from Huishuang Dong.
3D Measurement Techniques
Patients were required to cover their hair with operating caps, and the men were shaved before scanning.22,23 Artec Eva was directly connected to a computer, and this system required approximately 30 seconds for facial 3D image acquisition. The obtained facial-point cloud data were initially reconstructed to obtain a clear 3D facial image using Artec Studio. On this basis, the straight-line distances between the marked points were measured (Figure 2A, B). The 3D facial images before and after injection were fused to generate a volume-change cloud image (Figure 3A).
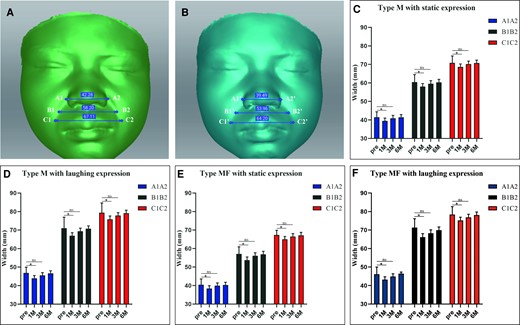
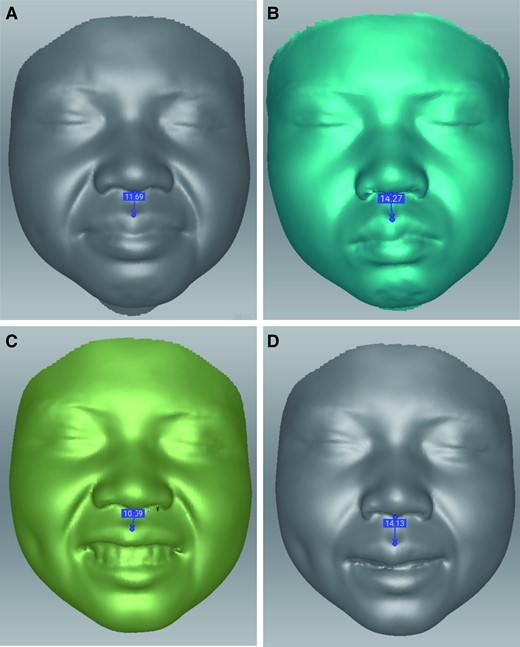
The width of the type MF NLF marked points in Artec Studio Professional software (Artec 3D; Senningerberg, Luxembourg) (A) before and (B) 1 month after BTX-A injection; static expression. (C-F) The width of bilateral marked points changed with time in both type M and type MF NLFs. BTX-A, botulinum toxin-A; M, muscular type; MF, muscle–fat pad mixed type; NLF, nasiolabial fold.
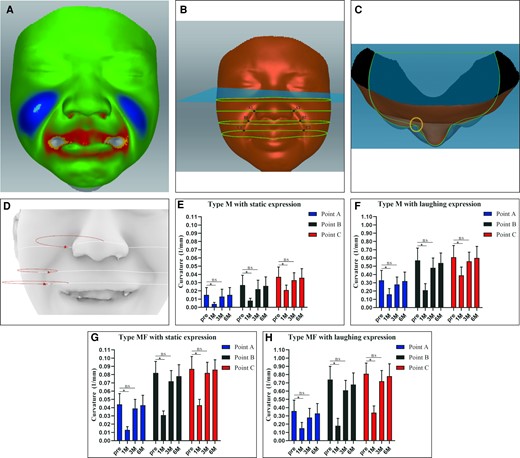
Pretreatment and posttreatment 3D facial images of static expression were fitted. (A) The colors in the different facial areas represent depth variation. The Frankfurt plane is the reference horizontal plane in Artec Studio (Artec 3D; Senningerberg, Luxembourg), and was adjusted to generate 3 horizontal planes where A, B, and C were located. The cross-sectional lines in the 3 planes are captured. (B) The 3D facial images before and after injection were superimposed, and the cross-sectional lines of each layer were extracted. (C) Two green lines indicate the contours of pretreatment and posttreatment models. The circle indicates the right area of the patient's NLF in vertical view. (D) The red circles represent the pretreatment curvature of a type M NLF while laughing in Rhino software. (E-H) The curvature change with time was analyzed by Rhino in both type M and type MF NLFs. The radius of the curvature is measured in millimeters. M, muscular type; MF, muscle–fat pad mixed type; NLF, nasiolabial fold.
The Frankfurt plane was the reference horizontal plane in Artec Studio, and was adjusted to generate 3 horizontal planes where A, B, and C were located. The cross-sectional lines in the 3 planes were captured. The 3D facial images before and after injection were superimposed, and the cross-sectional lines of each layer were extracted (Figure 3B, C). The curvature of the deepest point of the NLF before and after the injection was calculated with Rhino (Figure 3D).
The 3D model was imported into a custom Matlab script to generate scatter plots. The flowchart shows the NLF identification process (Supplemental Figure 1). Once the NLF had been established, scatter plots before and after injection were fused. A horizontal line was created, with the tip of the nose as a reference. The difference between the distance from points A, B, and C before and after injection to this horizontal line (A1A1′, B1B1′, and C1C1′) was measured, representing the change in the depth of the NLF (Figure 4A).
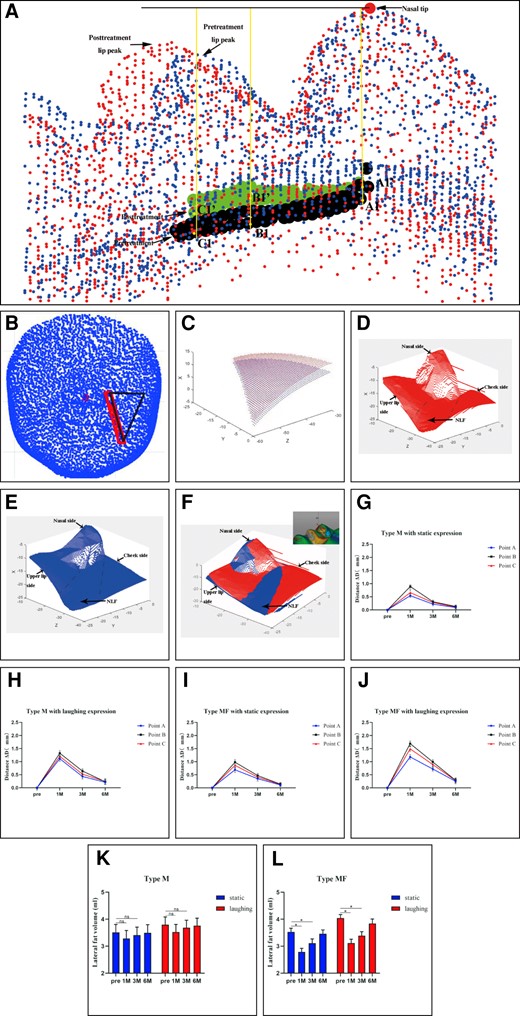
(A) Taking the nasal tip as the reference frame, the change in the distance to the nasal tip of the marked points of type MF NLFs after 1 month was measured in Matlab (MathWorks; Natick, MA). (B) The triangular regions determined by the starting point, the stop point, and a point 2 cm from the starting point horizontally from the pretreatment NLF were selected to measure fat volume changes in the lateral areas of the NLF before and after injection. (C) The lateral fat volume was selected and analyzed by Matlab. (D, E) The pretreatment and posttreatment NLF map were generated in Matlab. (F) Both of them were fitted. (G-J) The change in distance of marked points with time was analyzed by Matlab in both type M and type MF NLFs. (K, L) The lateral fat volume in both type M and MF NLFs was chosen and analyzed by Matlab. M, muscular type; MF, muscle–fat pad mixed type; NLF, nasolabial fold.
After 3D facial data were imported into Matlab, the NLF and lateral cheek regions were intercepted and fused. The triangular regions determined by the starting point, stop point, and point 2 cm from the starting point horizontally of the pretreatment NLF were selected to measure fat volume changes in the NLF lateral areas before and after injection (Figure 4B-F).
Statistical Analysis
Quantitative data satisfying normality tests are expressed as mean [standard deviation]. Measurements between groups were compared by paired-sample t-tests. All statistical analyses were performed with IBM SPSS version 26.0 software (IBM Corp., Armonk, NY), with a 2-sided P < .05 considered statistically significant.
Results
Ninety patients, 45 type M and 45 type MF subjects aged 20-52 years, received BTX-A treatment between July 2018 and July 2021. Eleven of these individuals were lost to follow-up between February and July 2020 due to coronavirus disease. Two patients were excluded without completing the follow-up on time, and 1 subject received other treatments for NLF after BTX-A injection and was withdrawn from the study. Seventy-six patients (69 females, 7 males), with a mean age of 32.4 years (range, 20-52 years), were followed up within 6 months after treatment and completed the study. Thirty-nine subjects (35 females, 4 males), with a mean age of 31.1 years (range, 20-48 years), had type M NLFs. Thirty-seven subjects (34 females, 3 males), with a mean age of 33.8 years (range, 22-52 years), had type MF NLFs.
Case 1
A 24-year-old female with type MF NLFs presented significant improvements in both static and laughing expressions in the first month (Figure 5; Supplemental Figure 2).
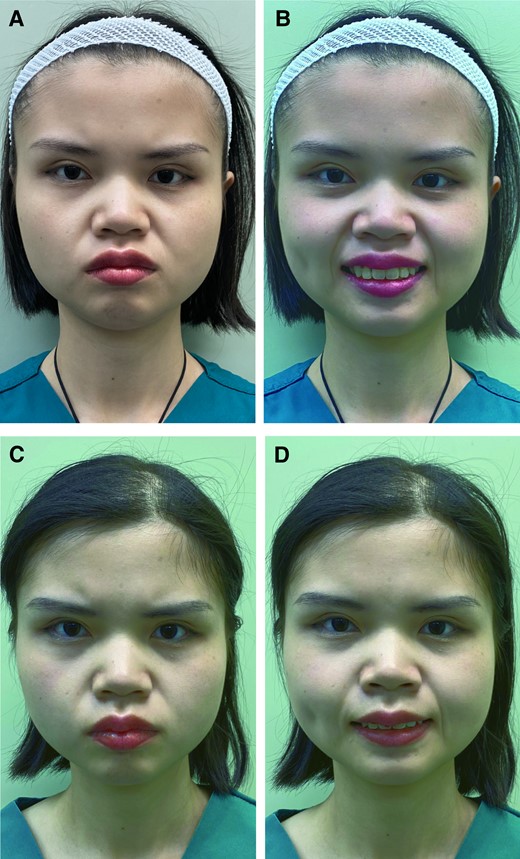
A 24-year-old female with a type MF NLF: pretreatment photographs showing the frontal view (A) in static expression and (B) while laughing. Type MF NLFs combine high tension of muscle contraction and hypertrophy of the fat pad. The fold deepens when standing up and smiling. In the supine position, the fold is reduced due to the smaller effect of gravity on the fat pad compared with when standing up, both for static and laughing expressions. In total, 6 points of the bilateral NLF needed to be injected: the levator labii alaeque nasi, zygomaticus minor, and zygomaticus major muscles (2 U at each injection site). The patient was followed up 1, 3, and 6 months after treatment. She showed significant improvements after 1 month of BTX A treatment: frontal view photographs (C) in static expression and (D) while laughing. BTX-A, botulinum toxin-A; MF, muscle–fat pad mixed type; NLF, nasolabial fold.
Case 2
A 29-year-old male with type M NLFs presented with improvements in laughing expression in the first month (Figure 6; Supplemental Figure 3). Among all groups, the widths between the 3 paired marks of bilateral NLFs decreased by the first month (P < .05) and recovered gradually by the third and sixth months (P > .05) (Figure 2C-F). In the M group, compared with preinjection, the NLF widths in the static condition decreased only by the first month (Figure 2C). The NLF widths in the laughing condition decreased in the first and third months, with the width variations being greater than those in the static condition (Figure 2D). In the MF group, the NLF widths both in static and laughing conditions decreased in the first and third month, with point B decreasing significantly more than points C and A (Figure 2E, F).
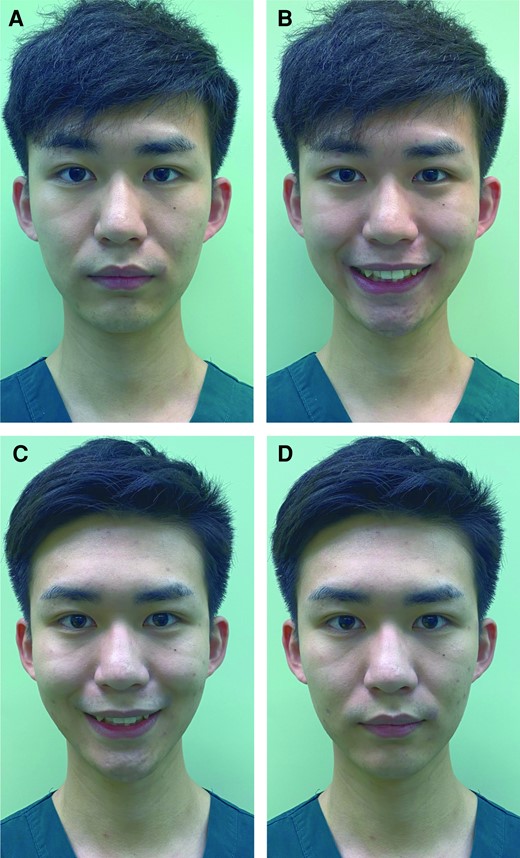
A 29-year-old male with a type M NLF: pretreatment photographs showing the frontal view (A) in static expression and (B) while laughing. For type M NLFs, there is muscular contraction resulting in high tension. The fold deepens when standing up and laughing. In the supine position, the fold shows no apparent change without a thick fat pad compared with when standing up both in static expression and while laughing. In total, 6 points of the bilateral NLF needed to be injected: the levator labii alaeque nasi, zygomaticus minor, and zygomaticus major muscles (2 U at each injection site). The patient was followed up 1, 3, and 6 months after treatment. He showed improvements (C) in laughing expression and no obvious change (D) in static expression in the first month. BTX-A, botulinum toxin-A; M, muscular type; NLF, nasiolabial fold.
Among all the groups, the curvatures were minimal in the first month (P < .05) and recovered gradually by the third and sixth months (P > .05) (Figure 3E-H). In the M group, compared with preinjection, the curvatures of 3 paired NLF marks in the static condition decreased only in the first month (Figure 3E). The curvatures in the laughing condition decreased by the first and third months, greater than those in static conditions (Figure 3F). In the MF group, the curvatures both in static and laughing conditions decreased by the first and third months, with point B decreasing significantly more than points C and A, and the changes while laughing were greater than those in the static condition (Figure 3G, H). Furthermore, at the first and third months, the variations in curvatures of the MF group were greater both in static and laughing conditions than those of the M group.
The depth variations (ΔD) of the 3 paired points were highest at the first month, lowest in the third month, and recovered in the sixth month (Figure 4G-J). In the M group, ΔD was greater in the laughing than in the static condition (Figure 4G, H). In the MF group, ΔD was also greater in the laughing than in the static condition, with point B improving significantly more than points C and A (Figure 4I, J). Additionally, the ΔD of the MF group, both in static and laughing conditions, was greater than that of the M group by the first and third months.
In the M group, the volume of the lateral adipose tissue of the NLF in static (pretreatment, 3.511 mL [0.292 mL] vs 1 month after [1M], 3.287 mL [0.297 mL]) and laughing (pretreatment, 3.793 mL [0.290 mL] vs 1M, 3.525 mL [0.282 mL]) conditions was slightly reduced in the first month (P > .05), but showed no statistical difference between each time point (Figure 4K). In the MF group, the fat volume in static (pretreatment, 3.530 mL [0.135mL] vs 1M, 2.784 mL [0.138mL]) and laughing (pretreatment, 4.024 mL [0.131] vs 1M, 3.117 [0.141] mL) conditions was the lowest in the first month (P < .05), and then gradually recovered (Figure 4L), and the variations were greater under laughing than under static conditions.
The results of the survey of satisfaction and complications are shown in Supplemental Figure 4. These showed that MF type NLFs had a higher percentage of satisfied patients compared with M type NLFs (Supplemental Figure 4A). Some patients felt pain and swelling in the early stage (Day 0-1). Some patients felt they had an unnatural appearance when smiling and exhibited more eye wrinkles (Supplemental Figure 4B, C). None of the patients had significant edema, ecchymosis, delayed hypersensitivity reactions, or other adverse events.
DISCUSSION
The NLF is a special and complex facial anatomic area. The anatomic features of type M and MF NLFs are as follows: (1) the formation of the NLF is closely related to the movement of facial muscles, such as the LLSAN, Zmi, and Zmj;33 (2) muscle fibers are directly inserted into the dermis beneath the NLF;34 and (3) the subcutaneous fat content of the NLF is very low, and the lateral region can accommodate abundant adipose tissue.1 Type M NLFs become deep in the static condition and even deeper in laughing conditions due to excessive muscle contractions. For type MF NLFs, on the basis of the movement of facial muscles, the relative height difference between the hypertrophy fat pad and the NLF increases, so type MF NLFs are deeper than type M NLFs in static conditions; while laughing, the muscle tightly pulls the NLF skin and squeezes adipose tissue upwards and outwards further, leading to a greater relative height difference, which makes the NLF especially prominent.2 Therefore, we selected the LLSAN, Zmi, and Zmj as markers to inject BTX-A, thereby inhibiting contraction of the 3 major muscles to reduce traction and indentation in the nasolabial area and achieve facial rejuvenation.
A comparison of the photographs indicated that the NLFs of the M group showed slight improvements in static and an obvious improvement in laughing conditions after BTX-A treatment. In addition, patients in the MF group showed more obvious improvements in both static and laughing states. Therefore, BTX-A had a better effect on type MF than on type M NLFs, which might be attributed to the change in the relative positional relationship between the muscle-skin attachment point and lateral adipose tissue. Our study innovatively introduced 3D scanning and measurement techniques to evaluate objectively and quantitatively the treatment effect and differences of BTX-A on the 2 types of NLF.
In recent years, several standard methods for evaluating NLFs have been proposed, including the Wrinkle Severity Rating Scale,15 the modified scale,35 and the 10-point facial wrinkle assessment scale.36 However, these methods are based on evaluation by clinicians, which is subjective and easily affected by lighting and body position.16 In addition, it is difficult to quantify the changes in the NLF because the horizontal and vertical cross sections and spatial position of the NLF cannot be depicted in photographs. However, the application of 3D measurement techniques can accurately reflect the spatial position changes of the NLF. Our study chose the Artec Eva 3D scanner, which can accurately capture (to within <1 mm) the NLF to evaluate changes in width, depth, curvature, and facial volume.17,18 In our results, the shortened width for type M and type MF NLFs suggested that BTX-A relaxed the muscles that pulled the NLF, leading to NLF adduction. Decreasing the curvature and depth of the NLF indicated that BTX-A made the NLF shallow by relaxing the tension and pulling on the skin attached to the LLSAN, Zmi, and Zmj muscles. In addition, NLF improvement was more obvious in the M and MF groups while laughing. Meanwhile, a greater improvement in NLF of type MF than type M by 3D measurement was observed, probably because BTX-A injection had an effect on the lateral fat pad while affecting muscle contraction (Figure 7).
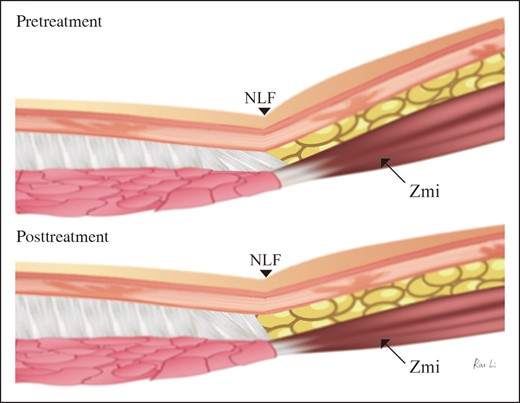
Anatomic diagrams showing the formation and change of the NLF. NLF, nasiolabial fold; Zmi, zygomaticus minor.
From an autopsy study, Kwon et al reported that the LLSAN, Zmi, and Zmj sent muscle fibers to the dermis to pull the skin of the NLF.1 Moreover, the traction of the LLSAN and Zmi in the lateral area of the NLF also causes extrusion of the fat compartment, deepening the NLF. We found no significant difference in the lateral fat-pad volume changes in the M group after treatment; however, the volume of the MF group decreased significantly after injection (Figure 4I). Therefore, because BTX-A affects the contraction functions of the LLSAN, Zmi, and Zmj, it weakens the traction of muscle fibers to the skin attachment point and improves type M NLFs without fat-pad displacement. On the basis of the above, the extrusion of muscles on the lateral fat pad was reduced so that the fat pad could move to the medial region, resulting in a decrease in height between the fat pad and the NLF (Figure 4D-F). Therefore, the improvements in curvature, width, and depth were more obvious in the MF group. Kwon et al also considered that the Zmi was the main muscle that pulled the medial skin of the NLF and limited the lateral adipose tissue, although this was even more obvious when the Zmi contracted.1 Thus, point B (skin attachment of the Zmi) of type MF produced a better improvement than that obtained with points C and A. All of the above explains why BTX-A had a better effect on the MF group.
BTX-A inhibits muscle contractions. Hyaluronic acid injections or fat grafting can be used to fill depressions. These 2 treatments have different mechanisms. Placing the patient in the sitting position is better for judging the degree of severity of the NLF, so it is recommended to choose the sitting position when filling. Research on facial skin movement in different positions recommends filling the NLF at 45° to 60°.19 In the supine position, for type M, the stop points of the muscles do not change much compared with the sitting position. For type MF, 2 factors are involved: high tension of muscle contraction and hypertrophy of fat pad. Fat pads can interfere with the injection of the NLF muscles in the sitting position. To exclude the effect of gravity on the fat pad in the sitting position on the selection of injection sites, we chose the supine position for more precise injection into the stop points of the muscles. In addition, the supine position maximizes the contact area between the body and the operating table, reducing patient fatigue. This position is beneficial for blood circulation to the limbs and brain, reducing the stress that patients might experience.31,32
This study had several limitations. First, BTX-A as an adjuvant therapy for NLF treatment, mainly acting on muscle dynamic factors, has certain limitations, and generally loses its effectiveness within 6 months. However, BTX-A can provide good conditions for combination treatments of NLFs, such as BTX-A with hyaluronic acid and autologous fat grafting for muscle and bone retrusion mixed types of NLFs. BTX-A can weaken the muscle contraction movement, which stabilizes the local environment of the fillers thereby promoting retention. Second, the eye wrinkles of the 2 types of subjects increased when they laughed after BTX-A injection (Figure 8). This indicated that when laughing, the compensatory contraction of the orbicularis oculi muscle produces an upward contraction effect that participates in smiling after BTX-A treatment. We also found that the philtrum length was significantly increased in the 2 types of patients when laughing (Figure 9). This indicated that the weakened contraction strength of the LLSAN caused upper lip drop and reduced tooth exposure, resulting in an unnatural appearance when laughing. Some patients felt they had an unnatural appearance when smiling (Supplemental Figure 4B, C). This limited their mouth opening while chewing hard, not just while laughing during the follow-up, and would be alarming to some patients. This indicated that the weakened contraction strength of the LLSAN caused the upper lip drop. After treatment, tooth exposure was significantly reduced and the range of motion of laughter became small. Gong et al found that anterior gingival exposure and bilateral posterior gingival exposure were significantly reduced after BTX-A injection because of upper lip dropping.9 This is consistent with our study. Therefore, we recommend that only 1 U of BTX-A should be injected into the LLSAN for NLF treatment without gingival smile. If NLF patients also have gingival smile, we suggest that 2 U of BTX-A should be injected into the LLSAN to treat both the NLF and the gingival smile. In addition, BTX-A should be injected around the eyes to prevent the deepening of periorbital wrinkles. Intradermal injection of BTX-A is a frequently performed procedure in aesthetic dermatology to improve facial skin tone, texture, wrinkles, and enlarged pores.37-40 Other researchers report injecting BTX-A over 2 weeks into the whole face skin at doses of 0.125 U/0.5 cm2. In our study we injected 12 U into the layer of muscles (2 U at each injection site) instead of microdroplet injection. It is a pity that so far we have not received any feedback on changes of skin tone from our patients.
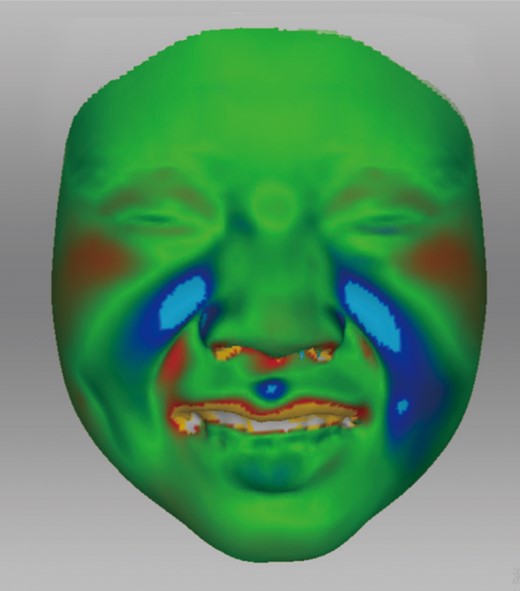
Pretreatment and 1-month posttreatment 3D scans of periocular changes while laughing of a muscle–fat pad mixed-type nasiolabial fold. The red regions indicated that the increased contractile force of orbicularis oculi at 1-month posttreatment.
The length change of the philtrum (A, C) before and (B, D) after 1 month of botulinum toxin-A treatment of a muscle–fat pad mixed-type nasiolabial fold.
Moreover, in the future, facial computed tomography and MRI should be combined to observe changes in soft tissue distribution in type M and MF NLFs treated with BTX-A.41,42 Due to the onset of COVID-19 since 2019, we lost complete follow-up data for 11 subjects. We will recruit more patients with type M and type MF NLFs to improve our experimental study.
CONCLUSIONS
3D technology can accurately and quantitatively analyze the efficacy of BTX-A for treating type M and type MF NLFs through measurement of curvature, width, depth, and fat-pad volume change. Moreover, BTX-A reduces the extrusion effect of muscles on fat pads. BTX-A is more effective for treating type MF NLFs compared with type M.
Supplemental Material
This article contains supplemental material located online at www.aestheticsurgeryjournal.com.
Acknowledgments
Ms Li and Dr Chen contributed equally to this work as co-first authors.
Funding
This study was supported by the National Natural Science Foundation of China (No. 82102356), the Outstanding Young Medical Talents Training Funding Project of the First Affiliated Hospital of Harbin Medical University (No. 2021J05), the Scientific Research and Innovation Foundation of the First Affiliated Hospital of Harbin Medical University (No. 2019B24), the Applied Technology Research and Development Project of Heilongjiang Province (No. GA20C019), and the Postgraduate Research & Practice Innovation Program of Harbin Medical University (No. YJSCX202088HYD).
Disclosures
The authors declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
REFERENCES
Author notes
Ms Li is a medical student, The Plastic and Aesthetic Center, The First Affiliated Hospital of Harbin Medical University, Harbin, P. R. China.
Dr Chen is a plastic surgeon, The Plastic and Aesthetic Center, The First Affiliated Hospital of Harbin Medical University, Harbin, P. R. China.
Dr Sun is a professor, College of Aerospace and Civil Engineering, Harbin Engineering University, Harbin, P. R. China.
Dr Hao is a plastic surgeon, The Plastic and Aesthetic Center, The First Affiliated Hospital of Harbin Medical University, Harbin, P. R. China.
Dr Luo are professor, The Plastic and Aesthetic Center, The First Affiliated Hospital of Harbin Medical University, Harbin, P. R. China.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}