





Dehumping is requested by the majority of patients who apply for rhinoplasty.1 There are several techniques for dehumping. The author utilizes the algorithm based on the dynamics of the techniques to decide on preservation or resection approach for dehumping.2 Middle vault reconstruction after hump resection is important for aesthetic and functional reasons. Although there are various techniques suggested for this purpose, spreader grafts and flaps are employed most often.1,3,4
Although spreader flaps are widely employed by different surgeons, they have various disadvantages.1,5 These include lack of utility in noses with a small hump and in cases in which the upper lateral cartilage is strong, difficulty in obtaining 3-dimensional symmetry in severely asymmetric noses, low potential for correcting septal curvatures, and difficulty in controlling for long-term changes (if the scoring or stitches applied to weaken the cartilage are excessive, the splay and spreader feature of the flap may decrease; if it is weak, it may cause widening of the middle vault and asymmetries in the long postoperative period).1,5 For these reasons, the author prefers spreader grafts to classic spreader flaps. After applying the spreader grafts, a mucoperichondrial spreader flap (MSF) is applied in suitable patients to obtain more symmetrical dorsal aesthetic lines while closing the middle vault.
The hump is properly excised as a component. After the mucoperichondrium of the upper lateral cartilage is dissected, the excessive parts of the cartilage are removed (Video demonstrating the application of the MSF is available online at www.aestheticsurgeryjournal.com). Septoplasty and osteotomies are employed according to the requirements of the nose. After the spreader grafts are properly applied, the middle roof is closed, and, depending on the condition of the middle vault, the utilization of an MSF is decided. An MSF is applied on the more defective side of the middle vault. While the middle vault is closed with horizontal mattress sutures, the dissected mucoperichondrium of the upper lateral cartilage is raised with thin forceps and the suture is passed deeper to create the MSF. Thanks to the MSF, the remaining part of the upper lateral cartilage is placed more laterally (Figure 1). In cases in which an MSF is not applied, the remaining part of the upper lateral cartilage is directly sutured to the spreader graft or septum. Depending on the case, the thickness of the flap can be designed by applying asymmetrical on the front and back, right and left, to create more symmetrical dorsal aesthetic lines.

Application of right mucoperichondrial spreader flap in this 22-year-old female patient with a left-sided deviated nose.
In this article, the author reviewed 857 patients in whom he applied an MSF among primary rhinoplasty patients he performed surgery on from February 2014 to August 2019. MSF was applied in patients who underwent upper lateral cartilage excision during hump reduction or nasal bridge narrowing. A total of 812 patients were female and 45 were male. The average age was 24 years old (range, 17-51). A unilateral MSF was applied in 584 patients, a bilateral asymmetrical MSF was applied in 251 patients, and a bilateral symmetrical MSF was applied in 22 patients (Figure 2). The follow-up period ranged from 12 to 74 months (median of 25.4 months). Patients whose upper lateral cartilage mucoperichondrium was damaged during dissection and revision cases were excluded from the study. Any patient not having at least 1 year of follow-up was also excluded. The study was conducted in accordance with the guidelines set forth in the Declaration of Helsinki. Written informed consent was obtained from all the patients. No complications, either functionally or aesthetically, were encountered related to MSF application. Postoperative breathing difficulties were experienced in 2 patients with allergic rhinitis in whom complaints resolved after medical treatment. Revision surgery was performed for 3 patients (1 for dorsum irregularity, 1 for nostril asymmetry, and 1 for columella asymmetry).
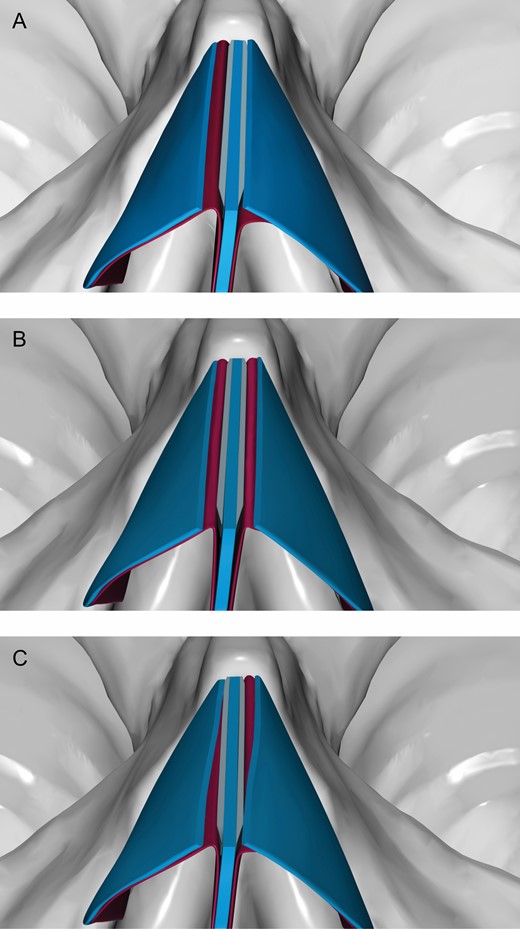
(A) Unilateral, (B) bilateral symmetrical, and (C) bilateral asymmetrical application of the mucoperichondrial spreader flap.
Performing symmetrical procedures on both sides without considering the requirements of the nose is one of the reasons for obtaining failed results in middle vault reconstruction. The presence of asymmetries in most noses and the differences between the upper lateral cartilage make proper application of MSFs according to the needs of the nose necessary when closing the middle vault. Utilizing an MSF has the following aims: (1) supporting the middle vault, especially in noses with thin skin and a narrow middle roof; (2) helping to create a midline perception in the nose by application on the opposite side of the deviation in deviated noses; (3) supporting the middle vault in cases where cartilage for grafting is lacking; and (4) recreating symmetric dorsal aesthetic lines (Figure 3). The main limitation that may prevent MSF application is damage to the upper lateral cartilage mucoperichondrium during dissection. In this respect, dissection should be conducted carefully.



This 27-year-old woman with a minimal linear dorsal deviation to the left side, a low radix, a wide nasal tip, and a hump. (A, C, E, G, I, K, M) Preoperative and (B, D, F, H, J, L, N) 1-year postoperative views are demonstrated from the frontal, helicopter, basal, right profile, right oblique, left profile, and left oblique views. Employing an open approach, hump reduction, radix augmentation, septoplasty, asymmetric osteotomies, bilateral spreader grafts, and right-sided mucoperichondrial spreader flap was performed. Tip-plasty included cephalic resection, transdomal stures, interdomal suture, and columellar strut grafting.
The difference between an MSF and an autospreader flap is that there is no cartilage in the anterior and medial parts of the flap; therefore, the MSF is thinner but more controlled for the long term. The main advantage of MSF compared with autospreader flaps is that it is more predictable. However, MSFs are not an alternative to spreader grafts or flaps. They are tools that can be utilized to obtain more symmetrical dorsal aesthetic lines while closing the middle roof after spreader grafts are applied. Future studies objectively demonstrating the aesthetic and functional effects of MSFs will allow them to be employed more widely.
Disclosures
The author declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
Funding
The author received no financial support for the research, authorship, and publication of this article.
REFERENCES


{kind=link}
{kind=link}
{kind=link}