





Preservation rhinoplasty: the revolution continues. The techniques described by the authors of “Improvement of Alar Concavity With Scroll Ligament Preservation: Sandwich Technique” 1 provide insight into the ongoing revolution in rhinoplasty surgery. As surgeons continue to marry the concepts of structural and preservation rhinoplasty, an algorithm is presented herein that illustrates this paradigm shift for treating alar concavity.
For decades rhinoplasty surgeons have focused on reductive techniques and subsequent grafting to improve long-term functional and aesthetic outcomes. These structural techniques have allowed surgeons to maintain better control of the operation in the short and medium term. However, long-term results remain a challenge as surgeons often watch the beautiful results of their operations partially deteriorate over time due to shrink-wrap forces, structural deterioration, and scar contracture. With this in mind, a new philosophical shift in rhinoplasty continues to evolve—the preservation rhinoplasty (PR).2
PR comprises the following 3 elements: (1) elevating the soft tissue envelope (STE) in a subperichondrial-subperiosteal plane; (2) preserving the dorsum; and (3) maintaining the nasal ligaments and alar cartilages with minimal excision while achieving the desired shape through sutures and tensioning. The principles of preservation surgery have had a profound effect on how we currently approach tip surgery. The era of reflex excisions, transections, and numerous grafts has passed. I now ask myself the following question at each consultation: “Can I preserve the alar cartilages with sutures and nonexcisional techniques?” The 3 critical steps in tip surgery are the following: (1) achieving an ideal domal shape; (2) remodeling the lateral crus; and (3) achieving tip support by utilizing tensioning techniques.
The authors provide practical solutions for dealing with alar (remodeling the lateral crus) concavity in an article that is succinct, well-diagrammed, and rational. They give a clear description of the problem, the associated aesthetic and functional issues, as well as an algorithm for treatment. Multiple techniques are described; however, the essentials are: (1) diagnose the problem as mild, moderate, or severe alar concavity; (2) preserve a 6-mm rim strip of lateral crural cartilage; (3) slide the remaining, preserved cephalic cartilage above or below the 6-mm rim strip; (4) preserve the scroll ligament complex including the longitudinal and vertical scroll ligaments; and (5) add a structural strut graft of cartilage in between the 6-mm rim strip and cephalic cartilage for increased support if necessary. By following these 5 principles, the alar cartilage as well as the scroll ligament complex remains completely intact. In effect, both lateral crural shape and strength are improved, lateral crural volume is decreased, and nothing is removed from the nose. The algorithm is presented as a reconstructive ladder—first preserve and then add structural support only if needed.
This article demonstrates a few very important principles of PR:
The more you take apart, the more you must reconstruct—do not disrupt more than you have to
The more you remove, the greater the scar contracture—use nonexcisional techniques if possible
Instability leads to warping—tensioning is better than floating
Learn a predictable set of techniques that work for you and then expand
One aspect of the article I found interesting was that lateral crural volume/shape was adjusted at the beginning of the tip sequence, and then, as necessary, domal shape and central support was addressed. Two aspects are worth discussion. First, it appears that the authors reflexively decrease the volume of the lateral crura to 6 mm. What is the reason for this? It has been my experience that only rarely does a patient achieve more tip definition by reducing the volume of the lateral crura—tip shape is more reliably achieved by tensioning the cartilage framework against the STE. In fact, the work of Regalado-Briz3 and my own experience in rhinoplasty on Latin patients guided me to the understanding that removal of cartilage in the nasal tip does not give a better tip shape. Theoretically, the authors are creating a 6-mm strip to create 1 layer of the sandwich and then use the remaining cartilage to treat the underlying concavity of the alar cartilage. I wonder what the authors do when the lateral crura is not concave? Do they still routinely perform a cephalic trim of some sort or do they preserve the alar cartilage?
Second, it appears that lateral crural shape and volume are addressed before tip suturing. When working within a structural philosophy, it makes sense to decrease the volume of alar cartilage with a cephalic resection, and then to use sutures and struts to shape and to support the tip, respectively. With a preservation philosophy, I believe it makes sense first to adjust domal shape with sutures and to tension the lateral crural with a lateral crural steal if needed. Once this has been done, the surgeon can then decide if lateral crural volume and shape must be adjusted. Every attempt is made to preserve the maximal amount of alar cartilage. Alar preservation is important because transection and excision (cephalic trim) weaken alar shape and projection. Complete alar preservation is the goal! It has been my experience that domal creation with a lateral crural steal procedure fixes many problems in the lateral crura, including concavity, convexity, length discrepancies, etc, as a neodome is formed. Therefore, I tend to adjust domal shape and lateral crural length before I decide whether I need to modifty the lateral crura. Of course, if after domal creation the lateral crural volume must be adjusted, the surgeon would optimally choose a technique that decreases volume while also strengthening the lateral crura. In 2009, Ozmen et al4 described the technique of incising the cephalic lateral crura longitudinally and then sliding the intact cephalic portion of the lateral crus underneath the remaining strip (Figure 1). Until now, this has been my technique of choice and, in fact, only once in my career have I used a strut as part of the “sandwich.” 5 After reading this article, I thank the authors for opening my eyes to other techniques with a similar philosophy! These sandwich techniques will surely be useful in a large number of cases of severe alar concavity and are easy to perform.
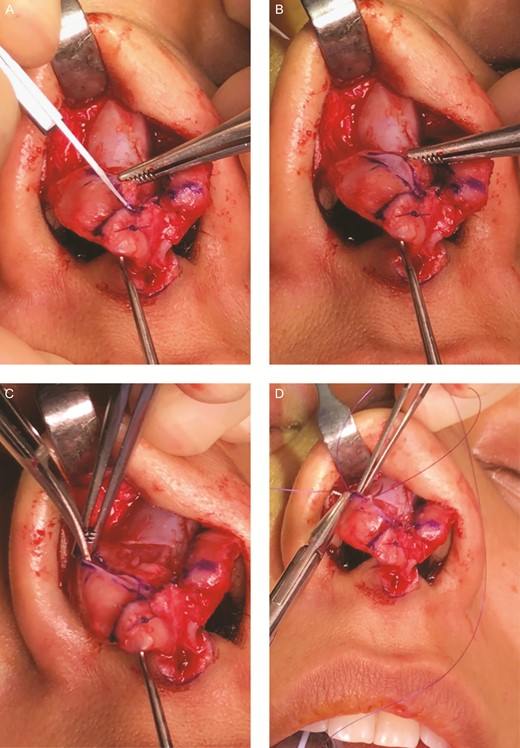
A demonstration of Ozmen et al’s technique on a 25-year-old female patient. (A) After domal creation with lateral crural steal, it is determined that the volume of the lateral crura must be further decreased. An incision is made 8 mm cephalic to the caudal border of the lower lateral cartilage. (B) The remaining cephalic cartilage is distracted cephalically while maintaining the longitudinal scroll ligament. (C) Scissor dissection is used to undermine the remaining lateral crura, helping to break the existing concavity/convexity and to create space for the cephalic portion to be “slid” under. (D) Sutures are used to attach and “sandwich” the 2 pieces of cartilage, making sure the knots are underneath the cartilage.
Future explorations into our ability to preserve nasal structures and to improve both aesthetic and functional outcomes are likely to be forthcoming. Preservation of the scroll ligament complex as well as the alar cartilages should provide long-term aesthetic and functional improvement. Only objective, functional studies will help provide true insight. Ultimately, tensioning of the alar cartilages against the STE occurs due to 3 factors. First, the domal creation sutures enhance domal shape and create tension by forming a straight and strong lateral crus with the caudal border higher than the cephalic border. Second, lateral crural steal creates tension by shortening and straightening the lateral crus. Third, attachment to a strut, and especially a septal extension graft, tensions the tip medially. The combination of these 3 factors as well as ligament reconstruction creates a strong tip complex tensioned at all 3 legs of the tripod with internal ligament support. By utilizing the techniques described above, it is likely that more than 90% of primary rhinoplasty patients will not need anything removed from the lateral crura. These techniques are reliable, easy to perform, and avoid loading the tip with grafts. I again want to congratulate the authors for their thoughtful algorithm for the treatment of alar concavity according to PR techniques and philosophies.
Disclosures
Dr Kosins is a Consultant and designs instruments for Micrins. He is also a Consultant to the Medical Advisory Committee of, and a shareholder in, ZO Skin Health.
Funding
The author received no financial support for the research, authorship, and publication of this article.
References


{kind=link}