





Abstract
Collagenase clostridium histolyticum (CCH) is a treatment for Peyronie's disease (PD) whose efficacy and safety has been demonstrated using a classic protocol and a shortened protocol.
To evaluate the efficacy and safety of an even more intense protocol in which a CCH injection is applied for 3 separate cycles of 1 week.
Prospective, nonrandomized, clinical study of a cohort of 13 patients with PD and non-ventral curvatures, between 30 and 90 degrees and with stable disease were included. Under local anesthesia, 0.9 mg of CCH is infiltrated in 3 parallel and equidistant transverse bands across the plaque in 3 sessions separated by 1 week. Between sessions the patient is instructed to perform home modeling and penis stretching.
The measurements collected were from girth, length of the penis and length of the plaque. Side and degree of curvature. Ultrasound evaluation of the plaque characteristics and assessing the interface between the tunica albuginea and Buck's fascia. Furthermore, questionnaires were collected: International Index of Erectile Function (IIEF) and 15-question and Peyronie's Disease Questionnaire (PDQ). All these parameters were evaluated before and after treatment.
An improvement in curvature was obtained in 76.9% of patients, reaching an improvement in the angle of curvature after the treatment cycles by an average of 19 ° (range 0-35 °) from the beginning. There are also improvements in the results of the IIEF and PDQ questionnaires. Length, penis girth, and plate length measurements hardly changed after treatment. Reported adverse effects are mild and limited to the penis.
We demonstrate the safety and efficacy of CCH in the treatment of PD using a more intense protocol than the previous ones. In addition, reducing the overall duration of allows for greater adherence and compliance of patients.
Introduction
Peyronie's disease (PD) is a condition in which collagen fibers are deposited in the tunica albuginea. It forms a fibrotic plaque that can result in a penile curvature. Often under diagnosed, it has an incidence rate of 3% to 9%. It generally affects men ages 40 to 60.1
It‘s etiology is unknown; it's believed that repetitive microtrauma during intercourse cause abnormal wound healing in patients genetically predisposed.2 Recognized risk factors are diabetes, hypertension and urological manipulations or surgeries.3 Furthermore, PD is more prevalent in men with Dupuytren contracture or Ledderhose disease.4
PD has 2 phases. An acute or inflammatory phase, in which plaque and curvature begin to form. Clinically, patients report pain during erection and a palpable nodule or plaque. Subsequently, chronic or fibrotic phase is characterized by disappearance of pain and stabilization of the curvature, which will rarely resolve spontaneously.4
Patients affected with PD present difficulty or inability to sexual intercourse, as well as significant relationship and psychological disorders.5
When the curvature of the penis prevents intercourse, surgery is indicated. However, many patients prefer conservative treatments such as pharmacotherapy, shock wave therapy, topical, or intralesional treatments.6 Within this last group, Collagenase clostridium histolyticum (CCH) is the one that has demonstrated clinical efficacy and safety for the treatment of PD in selected patients, saving many of them from surgery.7,8 Based on the results obtained in the Maximal Peyronie's Reduction Efficacy and Safety Studies (IMPRESS) I and II. CCH has been approved by the US Food and Drug Administration and the European Medicines Agency.7,9
The objective of the present study is to evaluate the safety and efficacy of CCH in the treatment of PD using a shorter protocol with the aim of reducing the duration of treatment.
Patients And Methods
Prospective, non-randomized, open-label clinical study of a cohort of 13 patients with PD were treated with 3 injections of 0.9mg CCH (Xiapex, Orphan Biovitrum, Stockholm, Sweden) separated by a week between 2018 and 2019 in a tertiary hospital. The research obtained an Institutional Review Board-approved informed.
The patients included present a curvature >30° and ≤90° dorsal or lateral and stable phase of the disease for at least three months.
Patients with complete plaque calcification in ultrasound or patients who had previously other treatments for PD, are excluded.
All of them have more than 18 years and sign a written informed consent prior the treatment.
Measurements
After recruitment, a complete medical history is collected including duration of disease from onset of symptoms.
All patients complete the 15-question Peyronie's Disease Questionnaire (PDQ) and the International Index of Erectile Function (IIEF-15) prior to treatment.
An initial physical examination is performed including measurement of the thickness of the penis in centimeters. Measurement of the penis in maximum extension in centimeters. Plaque location and size measured in centimeters. Side and degree of curvature measured with a goniometer during erection.
Furthermore, an ultrasound evaluation (6–12 MHz multifrequency linear probe, bk3000, Mileparken, Herlev Denmark) was performed, evaluating the size of the plaque, discarding complete calcification of the plaque or septal involvement, and assessing the interface between the fibrous layer, the tunica albuginea, and the loose fascial layer (Buck’s fascia).
All these parameters and questionnaires were also evaluated at the end of the treatment.
Technique
First, the skin is prepared with an antiseptic solution.
Subsequently, dorsal penile blockage anesthesia with 2% lidocaine 10 cc. is performed.
Stretch the flaccid penis to locate and isolate the fibrous plaque of the rest of the tissues
CCH (0,9mg) needle infiltration is performed in 3 parallel and equidistant transverse bands across the plaque (Figure 1 ). Afterward, penile compression is applied and held for 24 hours and anti-inflammatory medication is used for 2–3 days.
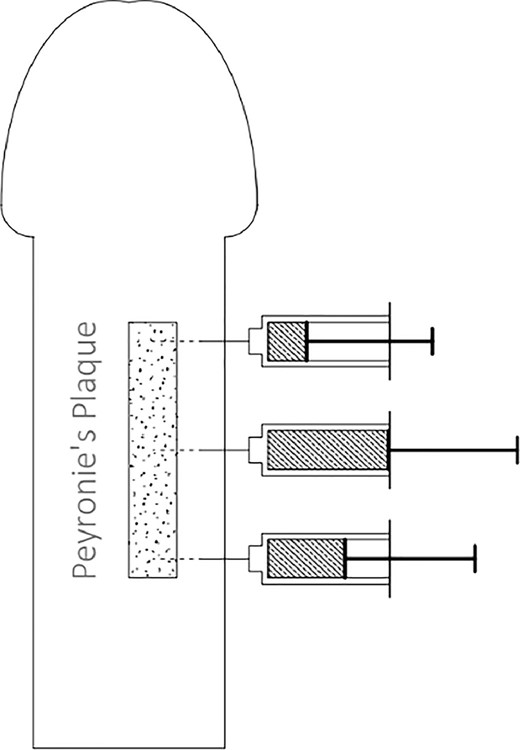
CCH injection method.
The stretching and modeling protocol was made by the patient at home:
During drug treatment, patients try to gently straighten the erect penis by slightly bending the penis in the opposite direction to the curve while maintaining the straightest position possible for 30. They should feel no discomfort no pain. They must repeat this operation once a day.
Stretching exercises with a flaccid penis consists of gradually stretching the flaccid penis for 60 seconds each time they go to the bathroom (5–6 times a day). With one hand at the base of the penis and the other at the tip, gently stretch the penis away from the body. Avoid doing these exercises on the day of the injection.
After 3 weeks of treatment, the patient is recommended to use the penile extender (AndroPenisAndromedical.S.L. Madrid, Spain). Begin by placing it with a flaccid penis, for an hour. Subsequently, it will increase the application time until using it between 6 and 8 hours a day for 3 months. Never use it while sleeping.
All patients were instructed to avoid sexual intercourse for 1 week after each injection and were informed about the importance of following the exercises at home. This was verified at each visit.
Treatment emergent adverse events were also collected in the medical consultation.
All data were collected and analyzed with the software program SPSS, version 23.
Results
Thirteen patients met the inclusion criteria, accepted to participate and were included in the study. All of them completed the treatment with the new protocol as planned. They were followed up to 6 months after the treatment ended.
The mean age of patients was 56.1 years (range 45–73), the duration of the PD was 38 months (range 14–66).
Erectile dysfunction was present in 3 patients (23%) but all of them were able achieve penetrative intercourse with the help of medication. Two patients without erectile dysfunction were unable to have sexual intercourse due to angulation of the penis.
The mean penile curvature at baseline was 49.2° (range 40–60°)
The measurements of length, girth of the penis and length of the plaque are shown in the Table 1 .
Measurements of length, girth of the penis and length of the plate before and after treatment
| Previous | Later | Difference | ||||
|---|---|---|---|---|---|---|
| Mean | Range | Mean | Range | Mean | Range | |
| Length of the penis | 10.6 | (7.9–13.5) | 10.71 | (8.2–13.5) | 0.13 | (−0.3 to 0.7) |
| Grith of the penis | 2.9 | (1.62–5.60) | 3.13 | (1.9–5.2) | 0.23 | (−0.4 to 0.8) |
| Length of the plaque | 2.7 | (1–5) | 2.14 | (1–3.4) | −0.92 | (−2.2 to 0) |
| Previous | Later | Difference | ||||
|---|---|---|---|---|---|---|
| Mean | Range | Mean | Range | Mean | Range | |
| Length of the penis | 10.6 | (7.9–13.5) | 10.71 | (8.2–13.5) | 0.13 | (−0.3 to 0.7) |
| Grith of the penis | 2.9 | (1.62–5.60) | 3.13 | (1.9–5.2) | 0.23 | (−0.4 to 0.8) |
| Length of the plaque | 2.7 | (1–5) | 2.14 | (1–3.4) | −0.92 | (−2.2 to 0) |
Measurements of length, girth of the penis and length of the plate before and after treatment
| Previous | Later | Difference | ||||
|---|---|---|---|---|---|---|
| Mean | Range | Mean | Range | Mean | Range | |
| Length of the penis | 10.6 | (7.9–13.5) | 10.71 | (8.2–13.5) | 0.13 | (−0.3 to 0.7) |
| Grith of the penis | 2.9 | (1.62–5.60) | 3.13 | (1.9–5.2) | 0.23 | (−0.4 to 0.8) |
| Length of the plaque | 2.7 | (1–5) | 2.14 | (1–3.4) | −0.92 | (−2.2 to 0) |
| Previous | Later | Difference | ||||
|---|---|---|---|---|---|---|
| Mean | Range | Mean | Range | Mean | Range | |
| Length of the penis | 10.6 | (7.9–13.5) | 10.71 | (8.2–13.5) | 0.13 | (−0.3 to 0.7) |
| Grith of the penis | 2.9 | (1.62–5.60) | 3.13 | (1.9–5.2) | 0.23 | (−0.4 to 0.8) |
| Length of the plaque | 2.7 | (1–5) | 2.14 | (1–3.4) | −0.92 | (−2.2 to 0) |
The types of curvature recorded were in the dorsal or lateral direction (Figure 2 ).
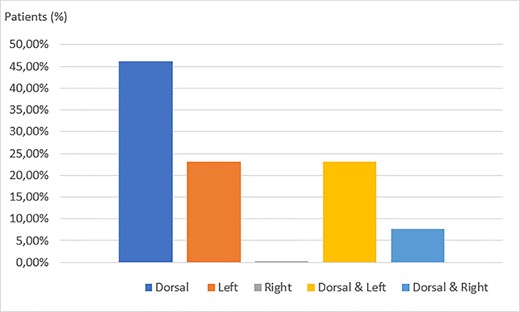
Curvature direction at the baseline.
On ultrasound, the interface between the tunica albuginea and the Buck´s fascia was present in 8 patients at baseline.
Ten patients (76.9%) had an improvement in the angle of curvature by a mean of 19° (range 0–35°) from baseline treatment. The final mean curvature was 30.2° (range 10–60°).
There was an improvement in the IIEF questionnaire of +2 points on average (range 1–7) and in the PDQ where we obtained an improvement of −4.7 points on average (range: −8 to 0)
After treatment, one patient lost the interface between the tunica albuginea and the Buck’s fascia
Adverse effects are shown in Table 2 . In no case there were systemic adverse events. No corporeal rupture or other Clavien Dindo II-III complications.
Adverse events occurring with each Xiapex injection
| Adverse event | First injection | Second injection | Third injection |
|---|---|---|---|
| Ecchymosis | 3 | 7 | 4 |
| Swelling | 5 | 11 | 7 |
| Pain | 2 | 4 | 1 |
| Glands sensitivity decreased | 0 | 1 | 3 |
| Blisters on the skin | 0 | 0 | 1 |
| Great bruises | 0 | 0 | 2 |
| Adverse event | First injection | Second injection | Third injection |
|---|---|---|---|
| Ecchymosis | 3 | 7 | 4 |
| Swelling | 5 | 11 | 7 |
| Pain | 2 | 4 | 1 |
| Glands sensitivity decreased | 0 | 1 | 3 |
| Blisters on the skin | 0 | 0 | 1 |
| Great bruises | 0 | 0 | 2 |
Adverse events occurring with each Xiapex injection
| Adverse event | First injection | Second injection | Third injection |
|---|---|---|---|
| Ecchymosis | 3 | 7 | 4 |
| Swelling | 5 | 11 | 7 |
| Pain | 2 | 4 | 1 |
| Glands sensitivity decreased | 0 | 1 | 3 |
| Blisters on the skin | 0 | 0 | 1 |
| Great bruises | 0 | 0 | 2 |
| Adverse event | First injection | Second injection | Third injection |
|---|---|---|---|
| Ecchymosis | 3 | 7 | 4 |
| Swelling | 5 | 11 | 7 |
| Pain | 2 | 4 | 1 |
| Glands sensitivity decreased | 0 | 1 | 3 |
| Blisters on the skin | 0 | 0 | 1 |
| Great bruises | 0 | 0 | 2 |
Discussion
Intralesional CCH is the only pharmacological therapy specifically approved for the treatment of PD. CCH is composed of collagenases formed by the bacteria C histolyticum that selectively destroy collagen in EP plaques without causing systemic toxicity or interaction with other drugs.
Its efficacy has been proven through two multinational phase III, double-blind, randomized, and placebo-controlled studies: IMPRESS I and II7,9
They included men with stable disease for more than 12 months and a dorsal or lateral curvature of ≥30° and ≤90°. Men with a completely calcified plaque were excluded. The protocol consists of 4 cycles of 2 injections of 0.58 mg CCH, 24–72 hours apart. Each cycle is spaced at least 6 weeks apart. As results they obtained 17°or 34% curvature reduction compared to 9.3°, 18.2% in the control group (P ≤ 0.0001) and an improvement in patient's symptom scores: PDQ.
Subsequently, a large open-label clinical trial was performed using the same protocol and primary end-points as the IMPRESS trial, obtaining comparable results.8
In order to reduce costs and duration of treatment, Ralph's working group designed a modified shortened protocol in which 0.9 mg of CCH is injected at intervals of 4 weeks for 3 cycles. They add home modeling, stretching and vacuum device daily, obtaining results comparable with previous protocols. Our results show a reduction of curvature and an improvement in the PDQ, comparable to those previously published.10
Nevertheless, adverse effects caused by injection of CCH reached 84.2% of participants in the largest series. These are usually localized to the penis, are mild and of short duration, such as swelling, bruising and penile pain among the most frequent. Serious adverse event that requires intervention such as large hematomas or ruptured corpora cavernosa are infrequent.7
It highlights that the injection of the whole vial of Xiapex (0.9 mg) compared to the half injection (0.58 mg) produces a higher percentage of ecchymosis and hematoma.10 In our series, we found similar percentages of local side effects to those described in the modified shortened protocol by Raheem et al. Additionally, by reducing the number of injections and doses, we decrease the probability of encountering serious adverse effects.
We observed that patients who present calcification of the plaque or absence of the interface between the tunica albuginea and Buck's fascia in the ultrasound examination prior to treatment obtain worse results. However, it is only an observed trend and we cannot guarantee that it is free of biases. Larger studies would be required to verify whether this fact could act as a predictor of response.
Following the lines of the shortened protocol of Raheem et al, we decrease the number of injections and visits from patients, who perform modeling maneuvers at home. With this protocol, we have managed to reduce the global treatment time while maintaining similar results.
In addition, we have been able to verify that despite increasing the intensity of the treatment by reducing the interval between doses to one week, there are no large differences in adverse effects or results. We believe that by performing a shorter and more intense treatment, we gain patient adherence and motivation to perform the maneuvers at home modeling exercises.
However, the main drawbacks of our work are that it is performed only in a hospital and we still have a small sample in order to extrapolate our results.
Conclusions
CCH is an effective and safe non-invasive treatment for patients with PD and t non-ventral curvatures, between 30-90 degrees and in a stable phase of the disease.
This work demonstrates the safety of CCH in the treatment of PD using a more intense protocol. Likewise, these initial data can be the basis for planning larger studies to also demonstrate the efficacy of this new protocol.
Statement Of Authorship
M.T.M.-S. and C.F.-P. conceived and performed the work. M.T.M.-S. and A.M.-M. wrote the manuscript. C.F.P. reviewed and F.L.-C.-P. and M.A.-M. supervised the work.
Funding None.
References
Author notes
Conflict of Interest: The authors report no conflicts of interest.

{kind=link}
{kind=link}