





A 63-year-old woman presented with fever and chest pain. She had been previously diagnosed with IgG4-related sclerosing cholangitis and a pulmonary pseudotumor 10 years earlier. Diagnosis was based on histopathological examination of the biliary tract, showing lymphocytic infiltrates, storiform fibrosis and obliterative phlebitis. As lung involvement resolved with corticosteroid therapy, she was currently under no treatment. On admission, bloodwork revealed elevated C-reactive protein and anaemia. Chest X-ray showed a right pulmonary opacity. Her symptoms persisted despite antibiotics, and she began to have pain in the right cervical region. Point-of-care ultrasound (POCUS) revealed a concentric thickening of the right common carotid wall (1.8 mm; normal <0.9), suggesting an inflammatory origin (Fig. 1A). A FDG-PET showed pathological uptake in right carotid artery and lower right lung (Fig. 1B, C). Further investigations were unremarkable with serum IgG4 levels of 37 mg/dl (normal <135), but presentation was consistent with an IgG4-RD flare. After 6 months receiving oral corticosteroids, complete clinical response was achieved with normalization (0.8 mm) of carotid wall thickness (Fig. 1D) and a significant reduction of uptakes on FDG-PET (Fig. 1E, F).
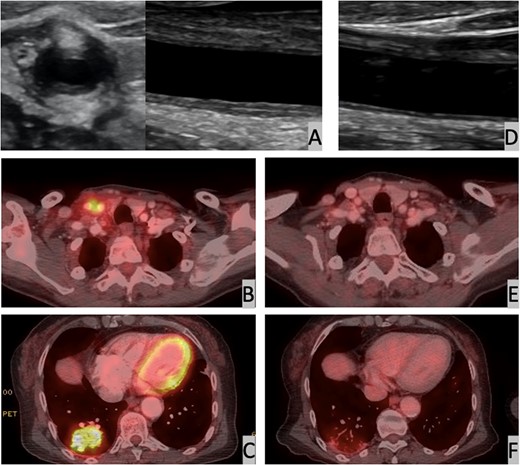
Ultrasound and PET-CT images of the carotid wall and lung
(A) Thickening of the carotid wall (1.8 mm) at clinical presentation. (B) Increased carotid uptake in PET (SULpeak 4.1) at clinical presentation. (C) Increased lung uptake in PET (SULpeak 5.7) at clinical presentation. (D) Normal carotid wall – 0.8 mm – 6 months later. (E) Normal carotid uptake in PET (SULpeak 1.7) 6 months later. (F) Reduced lung uptake in PET (SULpeak 2.1) 6 months later.
The best approach for monitoring the vascular compromise of IgG4-RD remains to be elucidated [1]. Given the positive correlation with clinical evolution and imaging findings in our case, as well as data from fast-track ultrasound approaches evaluating giant-cell arteritis [2], POCUS might be a valuable tool in the follow-up of IgG4-RD involving large vessels.
Informed consent has been obtained from the patient.
Funding: No specific funding was received from any bodies in the public, commercial or not-for-profit sectors to carry out the work described in this article.
Disclosure statement: The authors have declared no conflicts of interest.
Data availability statement
All data are incorporated into the article.

{kind=link}
Comments