





The patient, a 48-year-old man, suddenly presented with severe, sharp low back pain 1 week earlier. On examination, he showed impaired spinal mobility. He had no previous history of gouty arthropathy or kidney disease, a BMI of 22.3 kg/m2 and a lifestyle of alcohol intake. Laboratory tests revealed that his ESR was 14 mm/h (normal range 0–15 mm/h), CRP was 5.5 mg/l (normal range 0–10 mg/l) and serum uric acid was 513 μmol/l (normal range 125–410 μmol/l). MRI T1-weighted coronal image revealed a large intermediate-attenuation mass between the right erector spinae muscles (Fig. 1A). Pathological examination of a lumbar spine lesion showing aggregation of urate crystals (Fig. 1B). A diagnosis of spinal gout with erector spinae muscle entrapment was made [1]. Treatment with steroids combined with colchicine was initiated, leading to a remarkable improvement in laboratory findings and symptoms. Histopathological examination of biopsy can distinguish gout from tuberculosis and tumours. Studies have shown that spinal gout is present in up to 29% of patients with gout, and although axial gout is often asymptomatic, the diagnosis of gout should be considered when there is a sudden onset of acute and severe low back pain regardless of uric acid levels [2].
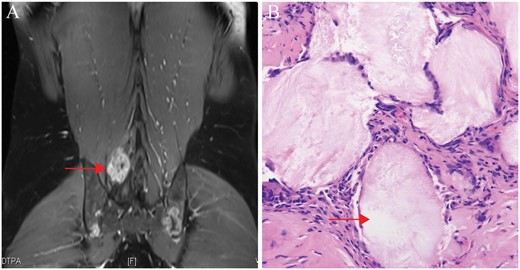
Manifestations of lumbar gout entrapment in the erector spinae muscle
(A, arrow) MRI T1-weighted coronal image revealed a large intermediate-attenuation mass between the right erector spinae muscles. (B, arrow) Pathological examination of a lumbar spine lesion showing aggregation of urate crystals.
Written informed consent was obtained from the patient for publication of this case (including publication of images).
Acknowledgements
G.W. and N.Z. wrote the paper. F.T., Z.W. and J.L. reviewed and edited the manuscript. Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Funding: No specific funding was received from any bodies in the public, commercial or not-for-profit sectors to carry out the work described in this article.
Disclosure statement: The authors have declared no conflicts of interest.
Data availability statement
Data are available on request.

{kind=link}
Comments