





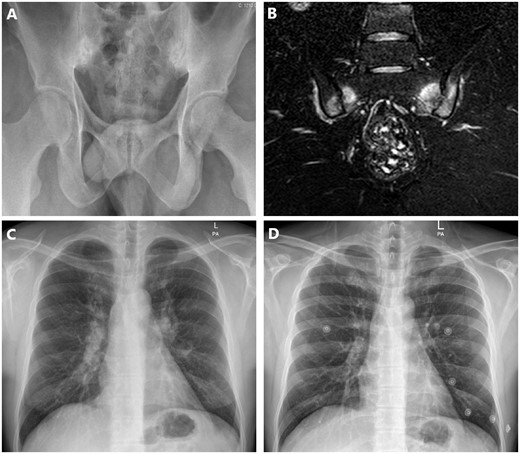
A 35-year-old man presented with a 2-year history of low back pain. The pain was inflammatory in nature, with early morning stiffness of >1 h. The patient’s personal and family past medical history was unremarkable. He had poor response to NSAIDs. Plain radiography of the spine was normal, however pelvic radiograph showed sclerosis and irregularities of sacroiliac joints suggesting grade 3 sacroiliitis (Fig. 1A). MRI revealed findings of bone oedema at the bilateral sacral and iliac wings (Fig. 1B). The laboratory investigation showed an ESR of 48 mm/h, CRP of 28 mg/l, serum angiotensin-converting enzyme of 162 U/l and HLA-B27 was negative. Chest X-ray showed increased density and enlargement of both hilums (Fig. 1C). PET‐CT imaging detected increased involvement of fluorodeoxyglucose ((Standardized uptake value) SUVmax: 12.8) in bilateral hilar lymphadenopathies and biopsy revealed non-caseified granulomatous inflammation. The diagnosis of sarcoidosis-associated sacroiliitis was established, and adalimumab was started for patient. Significant clinical improvement of his inflammatory back pain was seen within 3 months, and radiologic improvement of lung was achieved in a year (Fig. 1D).
Sacroiliitis in sarcoidosis mimicking ankylosing spondylitis
(A) Pelvic radiograph showing sacroiliitis. (B) MRI showing bone oedema at the bilateral sacral and iliac wings. (C) X-ray of lung showing increased density and enlargement of both hilums. (D) Radiologic improvement of lung after treatment.
Sarcoidosis may mimic rheumatic diseases and/or coexist with them. In small cohort studies, performed in sarcoidosis patients, it was reported that about 6–14.2% of these patients had radiographic sacroiliitis [1].
Funding: No specific funding was received from any funding bodies in the public, commercial or not-for-profit sectors to carry out the work described in this manuscript.
Disclosure statement: The authors have declared no conflicts of interest.

{kind=link}
Comments