





Abstract
In this systematic literature review and meta-analysis, we aimed to investigate the impact of cigarette smoking on the prevalence and incidence of psoriasis and psoriatic arthritis (PsA).
We performed a systematic literature review using the MEDLINE, EMBASE and Cochrane Central Register databases. The literature included publications from January 1980 to July 2019. The studies that provided clear information on the number of patients with ever smoking data were included in the meta-analysis.
The systematic literature review identified 52 and 24 articles for the prevalence of smoking in psoriasis and PsA, respectively. Of these, 16 articles on psoriasis and three and four (general population and psoriasis, respectively) articles on PsA met the criteria and were included in the meta-analysis. The prevalence of ever smoking was increased in psoriasis compared with the general population (OR: 1.84; 95% CI: 1.4, 2.3). For PsA the prevalence of ever smoking was reduced in psoriasis patients (OR: 0.70; 95% CI: 0.60, 0.81), but not changed compared with the general population (OR: 1.10; 95% CI: 0.92, 1.32).
This meta-analysis showed that ever smoking increases the risk of psoriasis in the general population, but may reduce the risk of PsA in psoriasis patients. The latter may be also due to the collider effect. Whether smoking cessation neutralizes the risk of developing psoriasis requires a well-defined smoking data collection for the past history and this is currently unavailable in the literature.
Smoking is higher in psoriasis patients compared with the general population.
There is decreased prevalence of smoking in psoriatic arthritis patients compared with psoriasis.
Differences across studies can be multifactorial, such as heterogeneity of psoriatic arthritis study design and collider bias.
Introduction
Psoriasis is a chronic, inflammatory, autoimmune skin disease, affecting 2–4% of the general population [1]. Various studies suggest that cigarette smoking may trigger the development of psoriasis through oxidative, inflammatory and genetic mechanisms, and a meta-analysis including publications up to 2013 indicated an association between psoriasis, current smoking and former smoking [2, 3].
Psoriatic arthritis (PsA) is a progressive, destructive, complex inflammatory arthritis that develops in up to one-third of patients with psoriasis [4]. The evidence of the association between smoking and the development of PsA among psoriasis patients is unclear and controversial. Some studies detected an inverse association whereas others found a positive association or no effect between smoking and the development of PsA [5–10].
In this systematic review and meta-analysis, we aimed to investigate the impact of cigarette smoking on the prevalence of psoriasis and PsA in the general population as well as the development of PsA among psoriasis patients.
Methods
Search and selection strategy
A systematic literature review was performed using a predefined PICO (population, intervention, comparator and outcome) strategy on MEDLINE, EMBASE and Cochrane Central Register databases, and details regarding the search strategy are given in Supplementary material, ‘Search strategy’, available at Rheumatology online. Additionally, the references of all included articles were manually scanned. To be eligible for inclusion, studies had to meet the following criteria: case–control, cross-sectional and cohort study design with assessment of the effect of smoking on psoriasis or PsA development in comparison with a control group, with case numbers (percentages) given in detail for each group. We excluded articles with incomplete data, reporting bias, duplication, case reports, review articles, consensus reports and languages other than English. The literature was screened from January 1980 to July 2019 for PsA. For psoriasis, the search was performed from June 2013 to July 2019 as another meta-analysis was published by Armstrong et al. on psoriasis, using the same methodology for the data from January 1980 to June 2013 [3]. The studies that were identified through that meta-analysis were included in our analysis and tables.
Since there may be difficulties in measuring smoking, meta-analysis was only performed on ever smoking. To be included in the meta-analysis, studies had to have full data for smoking with number of cases and clear data on ever smoking. For articles that had missing data on the latter, the corresponding authors were contacted by e-mail. Studies that were captured through literature review but failed to be included in the meta-analysis are presented in Tables 1 and 2. When multiple papers were identified using the same cohort, only studies with the highest number of patients were included. The study protocol was registered with the International Prospective Register of Systematic Reviews (PROSPERO: CRD42019140491).
Psoriasis and prevalence of smoking
| Study | Sample size, n | Number of patients who smoke, n | Measure of association, OR (95% CI) | |||
|---|---|---|---|---|---|---|
| Psoriasis | No psoriasis | Psoriasis | No psoriasis | Multivariatea | Univariateb | |
| Goolam Mahyoodeen (2019) [11] | 103 | 98 | Ever smoker: 61 | Ever smoker: 26 | Ever smoker: 3.87 (1.97, 7.63) | Ever smoker: 4.02 (2.22, 7.30) |
| Ferguson (2019) [12] | 5069 | 489 728 |
|
|
| |
| Shalom (2018) [13] | 118 680 | 118 680 | Ever smoker: 45 469 | Ever smoker: 41 044 | Ever smoker: 1.17 (1.16, 1.19) | |
| Alhomoud (2017) [14] | 100 | 100 | 48 | 36 | Smoker: 1.64 (0.93, 2.89) | |
| Atas (2017) [15] | 33 | 27 | 30 | 10 | Ever smoker: 148 (4.2, 5141) | Ever smoker: 17.00 (4.11, 70.39) |
| Chandravathi (2017) [16] | 150 | 50 | 30 | 3 | Smoker: 3.91 (1.14, 13.45) | |
| Girisha (2017) [17] | 156 | 156 | 65 | 53 | Smoker: 1.38 (0.87, 2.19) | |
| Koku Aksu (2016) [18] | 300 | 177 |
|
|
|
|
| Yousefzadeh (2017) [19] | 138 | 138 | Current smoker: 50 | Current smoker: 45 | Current smoker: 1.17 (0.71, 1.93) | |
| Zink (2017)c [20] | 102 | NR | 49% | 30% | NRd | |
| Meziane (2016) [21] | 150 | 300 | 27 | 28 | Smoker: 1.4 (0.2, 11) | Smoker: 2.13 (1.20, 3.77) |
| Cohen (2016)c [22] | 351 | 12031 | Ever smoker: 57.5% | Ever smoker: 44.10% | NRd | |
| Farshchian (2015) [23] | 55 | 55 | 32 | 9 | Smoker: 2.20 (1.1, 3.2) | Smoker: 7.11 (2.91, 17.36) |
| Irimie (2015) [24] | 142 | 167 | Current smoker: 36 | Current smoker: 31 | Current smoker: 1.49 (0.86, 2.56) | |
| Owczarczyk-Saczonek (2015) [25] | 62 | 861 | Female: 9 Male: 20 | Female: 101Male: 149 | Smoker: 2.14 (1.27, 3.61) | |
| Parisi (2015) [26] | 47 390 | 200 433 |
|
|
| |
| Takeshita (2015) [27] | 1321 | 11 959 |
|
|
| |
| Helmick (2015)c [28] | 275 | 10 401 |
|
|
| NRd |
| Gonzaga (2015)c [29] | 129 | 5472 | Tobacco use: 3.30% | Tobacco use: 22% | NRd | |
| Dowlatshahi (2013) [30] | 267 | 8009 | Current smoker: 85 | Current smoker: 1773 | Current smoker: 1.64 (1.26, 2.14) | |
| Halimi (2014) [31] | 53 | 55 | 23 | 11 | Smoker: 3.03 (1.30, 7.14) | Smoker: 3.06 (1.30, 7.21) |
| Kokpol (2014) [32] | 199 | 199 |
|
|
| |
| Ma (2014) [33] | 291 | 445 | 107 | 73 | Smoker: 2.96 (2.09, 4.08) | Smoker: 2.96 (2.09, 4.18) |
| Behrooz Shokouhi (2014) [34] | 47 | 42 | 16 | 19 | Smoker: 1.60 (0.68, 3.77) | Smoker: 0.62 (0.26,1.47) |
| Tseng (2013) [35] | 184 | 324 |
|
|
|
|
| Van der Voort (2014)c [36] | 118 | 2174 |
|
|
| NRd |
| Jensen (2013)c [37] | 238 | 3136 | Current smoker: 24.4% | Current smoker: 22.4% | NRd | |
| Armesto (2012)e [38] | 661 | 661 | 232 | 190 | Smoker: 1.34 (1.06, 1.69) | |
| Shapiro (2012)e [39] | 1079 | 1079 | Current smoker: 234 | Current smoker: 174 | Current smoker: 1.38 (1.10, 1.73) | Current smoker: 1.44 (1.16, 1.79) |
| Armstrong (2011)e [40] | 805 | 2098 |
|
|
|
|
| Al-Mutairi (2010)e [41] | 1484 | 1141 |
|
|
| |
| Gerdes (2010)e [42] | 1097 | 6963 | 509 | 2295 | Current smoker: 2.05 (1.77, 2.39) | Current smoker: 1.76 (1.55, 2.0) |
| Takahashi (2010)c,e [43] | 151 | 154 | NR | NR | NRd | |
| Driessen (2009)e [44] | 107 | 396 |
|
|
| |
| Jankovic (2009)e [45] | 110 | 200 |
|
|
| |
| Jin (2009)e [46] | 178 | 178 | 57 | 31 | Smoker: 2.07 (1.12, 3.82) | Smoker: 2.23 (1.36, 0.68) |
| Wolk (2009)e [47] | 373 | 373 | 82 | 138 | Current smoker: 1.7 (1.1, 2.6) | Current smoker: 0.48 (0.35, 0.66) |
| Wolkenstein (2009)e [48] | 350 | 1058 |
|
| Current smoker: 1.46 (1.11, 1.94) |
|
| Xiao (2009)e [49] | Mild Ps: 1619 Severe Ps: 1473 | 1521 |
| 241 |
|
|
| Bo (2008)c,e [50] | 1144 | 17 600 | Current smoker: 4739 Former smoker: 5581 | NR |
| NRd |
| Naldi (2008)e [51] | 560 | 690 | Ever smoker: 357 | Ever smoker: 350 | Ever smoker: 1.8 (1.3, 2.7) | Ever smoker: 1.71 (1.36, 2.15) |
| Cohen (2007)e [52] | 340 | 6643 | 118 | 1648 | 1.61 (1.28, 2.03) | |
| Gelfand (2006)e [53] | 130 976 | 556 995 | 36 701 | 438 299 | Current smoker: 1.31 (1.29, 1.34) | Current smoker: 0.11 (0.10, 0.11) |
| Sommer (2006)e [54] | 581 | 1044 | 264 | 219 | Smoker: 3.14 (2.52, 3.91) | |
| Herron (2005)e [55] | 557 | 4080 | 205 | 530 | Smoker: 3.90 (3.21, 4.74) | |
| Naldi (2005)e [56] | 550 | 690 |
|
|
|
|
| Zheng (2004)e [57] | 189 | 333 | Male: 53Female: 0 | Male: 49Female: 2 | Male smoker: 2.62 (1.53, 4.49) | Male smoker: 2.37 (1.53, 3.68) |
| Zhang (2002)e [58] | 789 | 789 | Male: 215Female: 9 | Male: 126Female: 5 | Ever smoker male: 2.33 (1.74, 3.11)Ever smoker female: 1.86 (0.56, 6.43) |
|
| Naldi (1999)e [59] | 404 | 616 |
|
|
|
|
| Poikolainen (1994)c,e [60] | 55 | 108 | NR | NR |
| NRd |
| Mills (1992)e [61] | 108 | 108 | Current smoker: 49 | Current smoker: 25 | Current smoker: 2.79 (1.55, 5.02) | |
| Naldi (1992)e [62] | 215 | 267 |
|
|
|
|
| Study | Sample size, n | Number of patients who smoke, n | Measure of association, OR (95% CI) | |||
|---|---|---|---|---|---|---|
| Psoriasis | No psoriasis | Psoriasis | No psoriasis | Multivariatea | Univariateb | |
| Goolam Mahyoodeen (2019) [11] | 103 | 98 | Ever smoker: 61 | Ever smoker: 26 | Ever smoker: 3.87 (1.97, 7.63) | Ever smoker: 4.02 (2.22, 7.30) |
| Ferguson (2019) [12] | 5069 | 489 728 |
|
|
| |
| Shalom (2018) [13] | 118 680 | 118 680 | Ever smoker: 45 469 | Ever smoker: 41 044 | Ever smoker: 1.17 (1.16, 1.19) | |
| Alhomoud (2017) [14] | 100 | 100 | 48 | 36 | Smoker: 1.64 (0.93, 2.89) | |
| Atas (2017) [15] | 33 | 27 | 30 | 10 | Ever smoker: 148 (4.2, 5141) | Ever smoker: 17.00 (4.11, 70.39) |
| Chandravathi (2017) [16] | 150 | 50 | 30 | 3 | Smoker: 3.91 (1.14, 13.45) | |
| Girisha (2017) [17] | 156 | 156 | 65 | 53 | Smoker: 1.38 (0.87, 2.19) | |
| Koku Aksu (2016) [18] | 300 | 177 |
|
|
|
|
| Yousefzadeh (2017) [19] | 138 | 138 | Current smoker: 50 | Current smoker: 45 | Current smoker: 1.17 (0.71, 1.93) | |
| Zink (2017)c [20] | 102 | NR | 49% | 30% | NRd | |
| Meziane (2016) [21] | 150 | 300 | 27 | 28 | Smoker: 1.4 (0.2, 11) | Smoker: 2.13 (1.20, 3.77) |
| Cohen (2016)c [22] | 351 | 12031 | Ever smoker: 57.5% | Ever smoker: 44.10% | NRd | |
| Farshchian (2015) [23] | 55 | 55 | 32 | 9 | Smoker: 2.20 (1.1, 3.2) | Smoker: 7.11 (2.91, 17.36) |
| Irimie (2015) [24] | 142 | 167 | Current smoker: 36 | Current smoker: 31 | Current smoker: 1.49 (0.86, 2.56) | |
| Owczarczyk-Saczonek (2015) [25] | 62 | 861 | Female: 9 Male: 20 | Female: 101Male: 149 | Smoker: 2.14 (1.27, 3.61) | |
| Parisi (2015) [26] | 47 390 | 200 433 |
|
|
| |
| Takeshita (2015) [27] | 1321 | 11 959 |
|
|
| |
| Helmick (2015)c [28] | 275 | 10 401 |
|
|
| NRd |
| Gonzaga (2015)c [29] | 129 | 5472 | Tobacco use: 3.30% | Tobacco use: 22% | NRd | |
| Dowlatshahi (2013) [30] | 267 | 8009 | Current smoker: 85 | Current smoker: 1773 | Current smoker: 1.64 (1.26, 2.14) | |
| Halimi (2014) [31] | 53 | 55 | 23 | 11 | Smoker: 3.03 (1.30, 7.14) | Smoker: 3.06 (1.30, 7.21) |
| Kokpol (2014) [32] | 199 | 199 |
|
|
| |
| Ma (2014) [33] | 291 | 445 | 107 | 73 | Smoker: 2.96 (2.09, 4.08) | Smoker: 2.96 (2.09, 4.18) |
| Behrooz Shokouhi (2014) [34] | 47 | 42 | 16 | 19 | Smoker: 1.60 (0.68, 3.77) | Smoker: 0.62 (0.26,1.47) |
| Tseng (2013) [35] | 184 | 324 |
|
|
|
|
| Van der Voort (2014)c [36] | 118 | 2174 |
|
|
| NRd |
| Jensen (2013)c [37] | 238 | 3136 | Current smoker: 24.4% | Current smoker: 22.4% | NRd | |
| Armesto (2012)e [38] | 661 | 661 | 232 | 190 | Smoker: 1.34 (1.06, 1.69) | |
| Shapiro (2012)e [39] | 1079 | 1079 | Current smoker: 234 | Current smoker: 174 | Current smoker: 1.38 (1.10, 1.73) | Current smoker: 1.44 (1.16, 1.79) |
| Armstrong (2011)e [40] | 805 | 2098 |
|
|
|
|
| Al-Mutairi (2010)e [41] | 1484 | 1141 |
|
|
| |
| Gerdes (2010)e [42] | 1097 | 6963 | 509 | 2295 | Current smoker: 2.05 (1.77, 2.39) | Current smoker: 1.76 (1.55, 2.0) |
| Takahashi (2010)c,e [43] | 151 | 154 | NR | NR | NRd | |
| Driessen (2009)e [44] | 107 | 396 |
|
|
| |
| Jankovic (2009)e [45] | 110 | 200 |
|
|
| |
| Jin (2009)e [46] | 178 | 178 | 57 | 31 | Smoker: 2.07 (1.12, 3.82) | Smoker: 2.23 (1.36, 0.68) |
| Wolk (2009)e [47] | 373 | 373 | 82 | 138 | Current smoker: 1.7 (1.1, 2.6) | Current smoker: 0.48 (0.35, 0.66) |
| Wolkenstein (2009)e [48] | 350 | 1058 |
|
| Current smoker: 1.46 (1.11, 1.94) |
|
| Xiao (2009)e [49] | Mild Ps: 1619 Severe Ps: 1473 | 1521 |
| 241 |
|
|
| Bo (2008)c,e [50] | 1144 | 17 600 | Current smoker: 4739 Former smoker: 5581 | NR |
| NRd |
| Naldi (2008)e [51] | 560 | 690 | Ever smoker: 357 | Ever smoker: 350 | Ever smoker: 1.8 (1.3, 2.7) | Ever smoker: 1.71 (1.36, 2.15) |
| Cohen (2007)e [52] | 340 | 6643 | 118 | 1648 | 1.61 (1.28, 2.03) | |
| Gelfand (2006)e [53] | 130 976 | 556 995 | 36 701 | 438 299 | Current smoker: 1.31 (1.29, 1.34) | Current smoker: 0.11 (0.10, 0.11) |
| Sommer (2006)e [54] | 581 | 1044 | 264 | 219 | Smoker: 3.14 (2.52, 3.91) | |
| Herron (2005)e [55] | 557 | 4080 | 205 | 530 | Smoker: 3.90 (3.21, 4.74) | |
| Naldi (2005)e [56] | 550 | 690 |
|
|
|
|
| Zheng (2004)e [57] | 189 | 333 | Male: 53Female: 0 | Male: 49Female: 2 | Male smoker: 2.62 (1.53, 4.49) | Male smoker: 2.37 (1.53, 3.68) |
| Zhang (2002)e [58] | 789 | 789 | Male: 215Female: 9 | Male: 126Female: 5 | Ever smoker male: 2.33 (1.74, 3.11)Ever smoker female: 1.86 (0.56, 6.43) |
|
| Naldi (1999)e [59] | 404 | 616 |
|
|
|
|
| Poikolainen (1994)c,e [60] | 55 | 108 | NR | NR |
| NRd |
| Mills (1992)e [61] | 108 | 108 | Current smoker: 49 | Current smoker: 25 | Current smoker: 2.79 (1.55, 5.02) | |
| Naldi (1992)e [62] | 215 | 267 |
|
|
|
|
OR (95% CI) numbers that were given in the articles.
OR (95% CI) numbers were calculated by investigators from given results.
Articles that gave only percentages.
Due to insufficient data, the OR could not be calculated.
Studies that were included from the meta-analysis by Armstrong et al. Identified numbers were extracted from full texts. NR: not reported; OR: odds ratio; Ps: psoriasis.
Psoriasis and prevalence of smoking
| Study | Sample size, n | Number of patients who smoke, n | Measure of association, OR (95% CI) | |||
|---|---|---|---|---|---|---|
| Psoriasis | No psoriasis | Psoriasis | No psoriasis | Multivariatea | Univariateb | |
| Goolam Mahyoodeen (2019) [11] | 103 | 98 | Ever smoker: 61 | Ever smoker: 26 | Ever smoker: 3.87 (1.97, 7.63) | Ever smoker: 4.02 (2.22, 7.30) |
| Ferguson (2019) [12] | 5069 | 489 728 |
|
|
| |
| Shalom (2018) [13] | 118 680 | 118 680 | Ever smoker: 45 469 | Ever smoker: 41 044 | Ever smoker: 1.17 (1.16, 1.19) | |
| Alhomoud (2017) [14] | 100 | 100 | 48 | 36 | Smoker: 1.64 (0.93, 2.89) | |
| Atas (2017) [15] | 33 | 27 | 30 | 10 | Ever smoker: 148 (4.2, 5141) | Ever smoker: 17.00 (4.11, 70.39) |
| Chandravathi (2017) [16] | 150 | 50 | 30 | 3 | Smoker: 3.91 (1.14, 13.45) | |
| Girisha (2017) [17] | 156 | 156 | 65 | 53 | Smoker: 1.38 (0.87, 2.19) | |
| Koku Aksu (2016) [18] | 300 | 177 |
|
|
|
|
| Yousefzadeh (2017) [19] | 138 | 138 | Current smoker: 50 | Current smoker: 45 | Current smoker: 1.17 (0.71, 1.93) | |
| Zink (2017)c [20] | 102 | NR | 49% | 30% | NRd | |
| Meziane (2016) [21] | 150 | 300 | 27 | 28 | Smoker: 1.4 (0.2, 11) | Smoker: 2.13 (1.20, 3.77) |
| Cohen (2016)c [22] | 351 | 12031 | Ever smoker: 57.5% | Ever smoker: 44.10% | NRd | |
| Farshchian (2015) [23] | 55 | 55 | 32 | 9 | Smoker: 2.20 (1.1, 3.2) | Smoker: 7.11 (2.91, 17.36) |
| Irimie (2015) [24] | 142 | 167 | Current smoker: 36 | Current smoker: 31 | Current smoker: 1.49 (0.86, 2.56) | |
| Owczarczyk-Saczonek (2015) [25] | 62 | 861 | Female: 9 Male: 20 | Female: 101Male: 149 | Smoker: 2.14 (1.27, 3.61) | |
| Parisi (2015) [26] | 47 390 | 200 433 |
|
|
| |
| Takeshita (2015) [27] | 1321 | 11 959 |
|
|
| |
| Helmick (2015)c [28] | 275 | 10 401 |
|
|
| NRd |
| Gonzaga (2015)c [29] | 129 | 5472 | Tobacco use: 3.30% | Tobacco use: 22% | NRd | |
| Dowlatshahi (2013) [30] | 267 | 8009 | Current smoker: 85 | Current smoker: 1773 | Current smoker: 1.64 (1.26, 2.14) | |
| Halimi (2014) [31] | 53 | 55 | 23 | 11 | Smoker: 3.03 (1.30, 7.14) | Smoker: 3.06 (1.30, 7.21) |
| Kokpol (2014) [32] | 199 | 199 |
|
|
| |
| Ma (2014) [33] | 291 | 445 | 107 | 73 | Smoker: 2.96 (2.09, 4.08) | Smoker: 2.96 (2.09, 4.18) |
| Behrooz Shokouhi (2014) [34] | 47 | 42 | 16 | 19 | Smoker: 1.60 (0.68, 3.77) | Smoker: 0.62 (0.26,1.47) |
| Tseng (2013) [35] | 184 | 324 |
|
|
|
|
| Van der Voort (2014)c [36] | 118 | 2174 |
|
|
| NRd |
| Jensen (2013)c [37] | 238 | 3136 | Current smoker: 24.4% | Current smoker: 22.4% | NRd | |
| Armesto (2012)e [38] | 661 | 661 | 232 | 190 | Smoker: 1.34 (1.06, 1.69) | |
| Shapiro (2012)e [39] | 1079 | 1079 | Current smoker: 234 | Current smoker: 174 | Current smoker: 1.38 (1.10, 1.73) | Current smoker: 1.44 (1.16, 1.79) |
| Armstrong (2011)e [40] | 805 | 2098 |
|
|
|
|
| Al-Mutairi (2010)e [41] | 1484 | 1141 |
|
|
| |
| Gerdes (2010)e [42] | 1097 | 6963 | 509 | 2295 | Current smoker: 2.05 (1.77, 2.39) | Current smoker: 1.76 (1.55, 2.0) |
| Takahashi (2010)c,e [43] | 151 | 154 | NR | NR | NRd | |
| Driessen (2009)e [44] | 107 | 396 |
|
|
| |
| Jankovic (2009)e [45] | 110 | 200 |
|
|
| |
| Jin (2009)e [46] | 178 | 178 | 57 | 31 | Smoker: 2.07 (1.12, 3.82) | Smoker: 2.23 (1.36, 0.68) |
| Wolk (2009)e [47] | 373 | 373 | 82 | 138 | Current smoker: 1.7 (1.1, 2.6) | Current smoker: 0.48 (0.35, 0.66) |
| Wolkenstein (2009)e [48] | 350 | 1058 |
|
| Current smoker: 1.46 (1.11, 1.94) |
|
| Xiao (2009)e [49] | Mild Ps: 1619 Severe Ps: 1473 | 1521 |
| 241 |
|
|
| Bo (2008)c,e [50] | 1144 | 17 600 | Current smoker: 4739 Former smoker: 5581 | NR |
| NRd |
| Naldi (2008)e [51] | 560 | 690 | Ever smoker: 357 | Ever smoker: 350 | Ever smoker: 1.8 (1.3, 2.7) | Ever smoker: 1.71 (1.36, 2.15) |
| Cohen (2007)e [52] | 340 | 6643 | 118 | 1648 | 1.61 (1.28, 2.03) | |
| Gelfand (2006)e [53] | 130 976 | 556 995 | 36 701 | 438 299 | Current smoker: 1.31 (1.29, 1.34) | Current smoker: 0.11 (0.10, 0.11) |
| Sommer (2006)e [54] | 581 | 1044 | 264 | 219 | Smoker: 3.14 (2.52, 3.91) | |
| Herron (2005)e [55] | 557 | 4080 | 205 | 530 | Smoker: 3.90 (3.21, 4.74) | |
| Naldi (2005)e [56] | 550 | 690 |
|
|
|
|
| Zheng (2004)e [57] | 189 | 333 | Male: 53Female: 0 | Male: 49Female: 2 | Male smoker: 2.62 (1.53, 4.49) | Male smoker: 2.37 (1.53, 3.68) |
| Zhang (2002)e [58] | 789 | 789 | Male: 215Female: 9 | Male: 126Female: 5 | Ever smoker male: 2.33 (1.74, 3.11)Ever smoker female: 1.86 (0.56, 6.43) |
|
| Naldi (1999)e [59] | 404 | 616 |
|
|
|
|
| Poikolainen (1994)c,e [60] | 55 | 108 | NR | NR |
| NRd |
| Mills (1992)e [61] | 108 | 108 | Current smoker: 49 | Current smoker: 25 | Current smoker: 2.79 (1.55, 5.02) | |
| Naldi (1992)e [62] | 215 | 267 |
|
|
|
|
| Study | Sample size, n | Number of patients who smoke, n | Measure of association, OR (95% CI) | |||
|---|---|---|---|---|---|---|
| Psoriasis | No psoriasis | Psoriasis | No psoriasis | Multivariatea | Univariateb | |
| Goolam Mahyoodeen (2019) [11] | 103 | 98 | Ever smoker: 61 | Ever smoker: 26 | Ever smoker: 3.87 (1.97, 7.63) | Ever smoker: 4.02 (2.22, 7.30) |
| Ferguson (2019) [12] | 5069 | 489 728 |
|
|
| |
| Shalom (2018) [13] | 118 680 | 118 680 | Ever smoker: 45 469 | Ever smoker: 41 044 | Ever smoker: 1.17 (1.16, 1.19) | |
| Alhomoud (2017) [14] | 100 | 100 | 48 | 36 | Smoker: 1.64 (0.93, 2.89) | |
| Atas (2017) [15] | 33 | 27 | 30 | 10 | Ever smoker: 148 (4.2, 5141) | Ever smoker: 17.00 (4.11, 70.39) |
| Chandravathi (2017) [16] | 150 | 50 | 30 | 3 | Smoker: 3.91 (1.14, 13.45) | |
| Girisha (2017) [17] | 156 | 156 | 65 | 53 | Smoker: 1.38 (0.87, 2.19) | |
| Koku Aksu (2016) [18] | 300 | 177 |
|
|
|
|
| Yousefzadeh (2017) [19] | 138 | 138 | Current smoker: 50 | Current smoker: 45 | Current smoker: 1.17 (0.71, 1.93) | |
| Zink (2017)c [20] | 102 | NR | 49% | 30% | NRd | |
| Meziane (2016) [21] | 150 | 300 | 27 | 28 | Smoker: 1.4 (0.2, 11) | Smoker: 2.13 (1.20, 3.77) |
| Cohen (2016)c [22] | 351 | 12031 | Ever smoker: 57.5% | Ever smoker: 44.10% | NRd | |
| Farshchian (2015) [23] | 55 | 55 | 32 | 9 | Smoker: 2.20 (1.1, 3.2) | Smoker: 7.11 (2.91, 17.36) |
| Irimie (2015) [24] | 142 | 167 | Current smoker: 36 | Current smoker: 31 | Current smoker: 1.49 (0.86, 2.56) | |
| Owczarczyk-Saczonek (2015) [25] | 62 | 861 | Female: 9 Male: 20 | Female: 101Male: 149 | Smoker: 2.14 (1.27, 3.61) | |
| Parisi (2015) [26] | 47 390 | 200 433 |
|
|
| |
| Takeshita (2015) [27] | 1321 | 11 959 |
|
|
| |
| Helmick (2015)c [28] | 275 | 10 401 |
|
|
| NRd |
| Gonzaga (2015)c [29] | 129 | 5472 | Tobacco use: 3.30% | Tobacco use: 22% | NRd | |
| Dowlatshahi (2013) [30] | 267 | 8009 | Current smoker: 85 | Current smoker: 1773 | Current smoker: 1.64 (1.26, 2.14) | |
| Halimi (2014) [31] | 53 | 55 | 23 | 11 | Smoker: 3.03 (1.30, 7.14) | Smoker: 3.06 (1.30, 7.21) |
| Kokpol (2014) [32] | 199 | 199 |
|
|
| |
| Ma (2014) [33] | 291 | 445 | 107 | 73 | Smoker: 2.96 (2.09, 4.08) | Smoker: 2.96 (2.09, 4.18) |
| Behrooz Shokouhi (2014) [34] | 47 | 42 | 16 | 19 | Smoker: 1.60 (0.68, 3.77) | Smoker: 0.62 (0.26,1.47) |
| Tseng (2013) [35] | 184 | 324 |
|
|
|
|
| Van der Voort (2014)c [36] | 118 | 2174 |
|
|
| NRd |
| Jensen (2013)c [37] | 238 | 3136 | Current smoker: 24.4% | Current smoker: 22.4% | NRd | |
| Armesto (2012)e [38] | 661 | 661 | 232 | 190 | Smoker: 1.34 (1.06, 1.69) | |
| Shapiro (2012)e [39] | 1079 | 1079 | Current smoker: 234 | Current smoker: 174 | Current smoker: 1.38 (1.10, 1.73) | Current smoker: 1.44 (1.16, 1.79) |
| Armstrong (2011)e [40] | 805 | 2098 |
|
|
|
|
| Al-Mutairi (2010)e [41] | 1484 | 1141 |
|
|
| |
| Gerdes (2010)e [42] | 1097 | 6963 | 509 | 2295 | Current smoker: 2.05 (1.77, 2.39) | Current smoker: 1.76 (1.55, 2.0) |
| Takahashi (2010)c,e [43] | 151 | 154 | NR | NR | NRd | |
| Driessen (2009)e [44] | 107 | 396 |
|
|
| |
| Jankovic (2009)e [45] | 110 | 200 |
|
|
| |
| Jin (2009)e [46] | 178 | 178 | 57 | 31 | Smoker: 2.07 (1.12, 3.82) | Smoker: 2.23 (1.36, 0.68) |
| Wolk (2009)e [47] | 373 | 373 | 82 | 138 | Current smoker: 1.7 (1.1, 2.6) | Current smoker: 0.48 (0.35, 0.66) |
| Wolkenstein (2009)e [48] | 350 | 1058 |
|
| Current smoker: 1.46 (1.11, 1.94) |
|
| Xiao (2009)e [49] | Mild Ps: 1619 Severe Ps: 1473 | 1521 |
| 241 |
|
|
| Bo (2008)c,e [50] | 1144 | 17 600 | Current smoker: 4739 Former smoker: 5581 | NR |
| NRd |
| Naldi (2008)e [51] | 560 | 690 | Ever smoker: 357 | Ever smoker: 350 | Ever smoker: 1.8 (1.3, 2.7) | Ever smoker: 1.71 (1.36, 2.15) |
| Cohen (2007)e [52] | 340 | 6643 | 118 | 1648 | 1.61 (1.28, 2.03) | |
| Gelfand (2006)e [53] | 130 976 | 556 995 | 36 701 | 438 299 | Current smoker: 1.31 (1.29, 1.34) | Current smoker: 0.11 (0.10, 0.11) |
| Sommer (2006)e [54] | 581 | 1044 | 264 | 219 | Smoker: 3.14 (2.52, 3.91) | |
| Herron (2005)e [55] | 557 | 4080 | 205 | 530 | Smoker: 3.90 (3.21, 4.74) | |
| Naldi (2005)e [56] | 550 | 690 |
|
|
|
|
| Zheng (2004)e [57] | 189 | 333 | Male: 53Female: 0 | Male: 49Female: 2 | Male smoker: 2.62 (1.53, 4.49) | Male smoker: 2.37 (1.53, 3.68) |
| Zhang (2002)e [58] | 789 | 789 | Male: 215Female: 9 | Male: 126Female: 5 | Ever smoker male: 2.33 (1.74, 3.11)Ever smoker female: 1.86 (0.56, 6.43) |
|
| Naldi (1999)e [59] | 404 | 616 |
|
|
|
|
| Poikolainen (1994)c,e [60] | 55 | 108 | NR | NR |
| NRd |
| Mills (1992)e [61] | 108 | 108 | Current smoker: 49 | Current smoker: 25 | Current smoker: 2.79 (1.55, 5.02) | |
| Naldi (1992)e [62] | 215 | 267 |
|
|
|
|
OR (95% CI) numbers that were given in the articles.
OR (95% CI) numbers were calculated by investigators from given results.
Articles that gave only percentages.
Due to insufficient data, the OR could not be calculated.
Studies that were included from the meta-analysis by Armstrong et al. Identified numbers were extracted from full texts. NR: not reported; OR: odds ratio; Ps: psoriasis.
PsA and prevalence of smoking
| Study | Control group information | Sample size (n) | Number of smokers (n) | Measure of association, OR (95% CI) | |||
|---|---|---|---|---|---|---|---|
| PsA | No PsA | PsA | No PsA | Multivariatea | Univariateb | ||
| Ferguson (2019) [12] | General population and psoriasis | 904 |
|
|
|
| |
| Kaine (2019) [63] | General population | 14.900 | 35.037 | 826 | 1.399 | Smoker: 1.41 (1.2922, 1.5415) | |
| Kibari (2019) [64] | General population | 3161 | 31 610 | Ever smoker: 904 | Ever smoker: 8742 | Ever smoker: 1.05 (0.97, 1.14) | Ever smoker: 1.05 (0.97, 1.14) |
| Yan (2019) [65] | Psoriasis | 128 | 107 | 44 | 35 | Smoker: 1.077 (0.62, 1.85) | |
| Gulati (2018) [66] | General population | 151 | 755 | 62 | 215 | Current smoker: 1.74 (1.21, 2.50) | |
| Yan (2018) [67] | Psoriasis | 175 | 497 | 6 | 30 | Smoker: 0.29 (0.06, 1.01) | Smoker: 0.52 (0.21, 1.27) |
| Queiro (2019)c [68] | Non-inflammatory rheumatic and skin problems | 340 | 600 | Current smoker: 26% | Current smoker: 21% | Smoker: 1.4 (1.0‐1.8) | NSd |
| Ibanez-Bosh (2017) [69] | General population | 53 | 53 |
|
|
| |
| Tsuruta (2017) [70] | Psoriasis | 55 | 276 | Ever smoker: 24 | Ever smoker: 113 | Ever smoker: 1.12 (0.62, 2.00) | |
| Wibetoe (2017) [71] | RA, AxSpA | 721 |
| Current smoker: 126 |
|
| |
| Krajewska- Włodarczyk (2018)c [72] | Psoriasis | 44 | 51 | Current smoker: 18% | Current smoker: 10% | NSd | |
| Gulati (2016) [73] | General population | 338 | 50 468 | Current smoker: 76 | Current smoker: 8270 | Current smoker: 1.4801 (1.15, 1.9128) | |
| Nas (2015)c [74] | Psoriasis and RA | 173 | Psoriasis: 67RA: 138 | Current smoker: 35.30% | Psoriasis current smoker: 31.3%RA current: 10.1% | NSd | |
| Papagoras (2014)c [75] | AS and Healthy population | 56 | Healthy population: 71AS: 56 | Current smoker: 28.60% | Healthy population current smoker: 18.30%AS current: 60.7% | NSd | |
| Bhole (2012)c [76] | Psoriasis, RA, andGeneral population | 644 | Psoriasis: 448 RA: 350 General population: 115 787 | Ever smoker: 44% | Ever smoker Psoriasis: 48%RA: 60%General population: NR | NSd | |
| Velez (2012)c [77] | Psoriasis | 107 | 161 | Ever smoker: 31.80% | Ever smoker: 39.20% | NSd | |
| Eder (2012) [7] | Psoriasis | 728 | 404 |
|
|
|
|
| Eder (2011) [78] | Psoriasis | 159 | 159 | Ever smoker: 64 | Ever smoker: 89 |
| Ever smoker: 0.52 (0.33, 0.82) |
| Husted (2011)c [79] | Psoriasis | 611 | 449 | Current smoker: 12% | Current smoker: 24.40% | NSd | |
| Tey (2010) [10] | Psoriasis | 134 | 266 |
|
| Current: 0.81 (0.50, 1.32) | |
| Tam (2008) [80] | General population | 82 | 82 | Current smoker: 8 | Current smoker: 0 | Current smoker: 18.82 (1.06, 331.81) | |
| Tam (2008) [81] | General population | 102 | 82 | Current smoker: 9 | Current smoker: 8 | Current smoker: 0.90 (0.33, 2.4336) | |
| Kimhi (2007) [82] | General population | 47 | 100 | 16 | 28 | Smoker: 1.32 (0.63, 2.79) | |
| Pattison (2007) [6] | Psoriasis | 98 | 163 | Ever smoker: 57 | Ever smoker: 102 | Ever smoker: 0.68 (0.39,1.17) | Ever smoker: 0.83 (0.50, 1.39) |
| Study | Control group information | Sample size (n) | Number of smokers (n) | Measure of association, OR (95% CI) | |||
|---|---|---|---|---|---|---|---|
| PsA | No PsA | PsA | No PsA | Multivariatea | Univariateb | ||
| Ferguson (2019) [12] | General population and psoriasis | 904 |
|
|
|
| |
| Kaine (2019) [63] | General population | 14.900 | 35.037 | 826 | 1.399 | Smoker: 1.41 (1.2922, 1.5415) | |
| Kibari (2019) [64] | General population | 3161 | 31 610 | Ever smoker: 904 | Ever smoker: 8742 | Ever smoker: 1.05 (0.97, 1.14) | Ever smoker: 1.05 (0.97, 1.14) |
| Yan (2019) [65] | Psoriasis | 128 | 107 | 44 | 35 | Smoker: 1.077 (0.62, 1.85) | |
| Gulati (2018) [66] | General population | 151 | 755 | 62 | 215 | Current smoker: 1.74 (1.21, 2.50) | |
| Yan (2018) [67] | Psoriasis | 175 | 497 | 6 | 30 | Smoker: 0.29 (0.06, 1.01) | Smoker: 0.52 (0.21, 1.27) |
| Queiro (2019)c [68] | Non-inflammatory rheumatic and skin problems | 340 | 600 | Current smoker: 26% | Current smoker: 21% | Smoker: 1.4 (1.0‐1.8) | NSd |
| Ibanez-Bosh (2017) [69] | General population | 53 | 53 |
|
|
| |
| Tsuruta (2017) [70] | Psoriasis | 55 | 276 | Ever smoker: 24 | Ever smoker: 113 | Ever smoker: 1.12 (0.62, 2.00) | |
| Wibetoe (2017) [71] | RA, AxSpA | 721 |
| Current smoker: 126 |
|
| |
| Krajewska- Włodarczyk (2018)c [72] | Psoriasis | 44 | 51 | Current smoker: 18% | Current smoker: 10% | NSd | |
| Gulati (2016) [73] | General population | 338 | 50 468 | Current smoker: 76 | Current smoker: 8270 | Current smoker: 1.4801 (1.15, 1.9128) | |
| Nas (2015)c [74] | Psoriasis and RA | 173 | Psoriasis: 67RA: 138 | Current smoker: 35.30% | Psoriasis current smoker: 31.3%RA current: 10.1% | NSd | |
| Papagoras (2014)c [75] | AS and Healthy population | 56 | Healthy population: 71AS: 56 | Current smoker: 28.60% | Healthy population current smoker: 18.30%AS current: 60.7% | NSd | |
| Bhole (2012)c [76] | Psoriasis, RA, andGeneral population | 644 | Psoriasis: 448 RA: 350 General population: 115 787 | Ever smoker: 44% | Ever smoker Psoriasis: 48%RA: 60%General population: NR | NSd | |
| Velez (2012)c [77] | Psoriasis | 107 | 161 | Ever smoker: 31.80% | Ever smoker: 39.20% | NSd | |
| Eder (2012) [7] | Psoriasis | 728 | 404 |
|
|
|
|
| Eder (2011) [78] | Psoriasis | 159 | 159 | Ever smoker: 64 | Ever smoker: 89 |
| Ever smoker: 0.52 (0.33, 0.82) |
| Husted (2011)c [79] | Psoriasis | 611 | 449 | Current smoker: 12% | Current smoker: 24.40% | NSd | |
| Tey (2010) [10] | Psoriasis | 134 | 266 |
|
| Current: 0.81 (0.50, 1.32) | |
| Tam (2008) [80] | General population | 82 | 82 | Current smoker: 8 | Current smoker: 0 | Current smoker: 18.82 (1.06, 331.81) | |
| Tam (2008) [81] | General population | 102 | 82 | Current smoker: 9 | Current smoker: 8 | Current smoker: 0.90 (0.33, 2.4336) | |
| Kimhi (2007) [82] | General population | 47 | 100 | 16 | 28 | Smoker: 1.32 (0.63, 2.79) | |
| Pattison (2007) [6] | Psoriasis | 98 | 163 | Ever smoker: 57 | Ever smoker: 102 | Ever smoker: 0.68 (0.39,1.17) | Ever smoker: 0.83 (0.50, 1.39) |
OR (95% CI) numbers that were given in the articles.
OR (95% CI) numbers were calculated by investigators from given results.
Articles that gave only percentages.
Due to insufficient data, the OR could not be calculated. AS: ankylosing spondylitis; AxSpA: axial spondylartritis; NS: not specified; OR: odds ratio; PsA: Psoriatic arthritis; RA: rheumatoid arthritis.
PsA and prevalence of smoking
| Study | Control group information | Sample size (n) | Number of smokers (n) | Measure of association, OR (95% CI) | |||
|---|---|---|---|---|---|---|---|
| PsA | No PsA | PsA | No PsA | Multivariatea | Univariateb | ||
| Ferguson (2019) [12] | General population and psoriasis | 904 |
|
|
|
| |
| Kaine (2019) [63] | General population | 14.900 | 35.037 | 826 | 1.399 | Smoker: 1.41 (1.2922, 1.5415) | |
| Kibari (2019) [64] | General population | 3161 | 31 610 | Ever smoker: 904 | Ever smoker: 8742 | Ever smoker: 1.05 (0.97, 1.14) | Ever smoker: 1.05 (0.97, 1.14) |
| Yan (2019) [65] | Psoriasis | 128 | 107 | 44 | 35 | Smoker: 1.077 (0.62, 1.85) | |
| Gulati (2018) [66] | General population | 151 | 755 | 62 | 215 | Current smoker: 1.74 (1.21, 2.50) | |
| Yan (2018) [67] | Psoriasis | 175 | 497 | 6 | 30 | Smoker: 0.29 (0.06, 1.01) | Smoker: 0.52 (0.21, 1.27) |
| Queiro (2019)c [68] | Non-inflammatory rheumatic and skin problems | 340 | 600 | Current smoker: 26% | Current smoker: 21% | Smoker: 1.4 (1.0‐1.8) | NSd |
| Ibanez-Bosh (2017) [69] | General population | 53 | 53 |
|
|
| |
| Tsuruta (2017) [70] | Psoriasis | 55 | 276 | Ever smoker: 24 | Ever smoker: 113 | Ever smoker: 1.12 (0.62, 2.00) | |
| Wibetoe (2017) [71] | RA, AxSpA | 721 |
| Current smoker: 126 |
|
| |
| Krajewska- Włodarczyk (2018)c [72] | Psoriasis | 44 | 51 | Current smoker: 18% | Current smoker: 10% | NSd | |
| Gulati (2016) [73] | General population | 338 | 50 468 | Current smoker: 76 | Current smoker: 8270 | Current smoker: 1.4801 (1.15, 1.9128) | |
| Nas (2015)c [74] | Psoriasis and RA | 173 | Psoriasis: 67RA: 138 | Current smoker: 35.30% | Psoriasis current smoker: 31.3%RA current: 10.1% | NSd | |
| Papagoras (2014)c [75] | AS and Healthy population | 56 | Healthy population: 71AS: 56 | Current smoker: 28.60% | Healthy population current smoker: 18.30%AS current: 60.7% | NSd | |
| Bhole (2012)c [76] | Psoriasis, RA, andGeneral population | 644 | Psoriasis: 448 RA: 350 General population: 115 787 | Ever smoker: 44% | Ever smoker Psoriasis: 48%RA: 60%General population: NR | NSd | |
| Velez (2012)c [77] | Psoriasis | 107 | 161 | Ever smoker: 31.80% | Ever smoker: 39.20% | NSd | |
| Eder (2012) [7] | Psoriasis | 728 | 404 |
|
|
|
|
| Eder (2011) [78] | Psoriasis | 159 | 159 | Ever smoker: 64 | Ever smoker: 89 |
| Ever smoker: 0.52 (0.33, 0.82) |
| Husted (2011)c [79] | Psoriasis | 611 | 449 | Current smoker: 12% | Current smoker: 24.40% | NSd | |
| Tey (2010) [10] | Psoriasis | 134 | 266 |
|
| Current: 0.81 (0.50, 1.32) | |
| Tam (2008) [80] | General population | 82 | 82 | Current smoker: 8 | Current smoker: 0 | Current smoker: 18.82 (1.06, 331.81) | |
| Tam (2008) [81] | General population | 102 | 82 | Current smoker: 9 | Current smoker: 8 | Current smoker: 0.90 (0.33, 2.4336) | |
| Kimhi (2007) [82] | General population | 47 | 100 | 16 | 28 | Smoker: 1.32 (0.63, 2.79) | |
| Pattison (2007) [6] | Psoriasis | 98 | 163 | Ever smoker: 57 | Ever smoker: 102 | Ever smoker: 0.68 (0.39,1.17) | Ever smoker: 0.83 (0.50, 1.39) |
| Study | Control group information | Sample size (n) | Number of smokers (n) | Measure of association, OR (95% CI) | |||
|---|---|---|---|---|---|---|---|
| PsA | No PsA | PsA | No PsA | Multivariatea | Univariateb | ||
| Ferguson (2019) [12] | General population and psoriasis | 904 |
|
|
|
| |
| Kaine (2019) [63] | General population | 14.900 | 35.037 | 826 | 1.399 | Smoker: 1.41 (1.2922, 1.5415) | |
| Kibari (2019) [64] | General population | 3161 | 31 610 | Ever smoker: 904 | Ever smoker: 8742 | Ever smoker: 1.05 (0.97, 1.14) | Ever smoker: 1.05 (0.97, 1.14) |
| Yan (2019) [65] | Psoriasis | 128 | 107 | 44 | 35 | Smoker: 1.077 (0.62, 1.85) | |
| Gulati (2018) [66] | General population | 151 | 755 | 62 | 215 | Current smoker: 1.74 (1.21, 2.50) | |
| Yan (2018) [67] | Psoriasis | 175 | 497 | 6 | 30 | Smoker: 0.29 (0.06, 1.01) | Smoker: 0.52 (0.21, 1.27) |
| Queiro (2019)c [68] | Non-inflammatory rheumatic and skin problems | 340 | 600 | Current smoker: 26% | Current smoker: 21% | Smoker: 1.4 (1.0‐1.8) | NSd |
| Ibanez-Bosh (2017) [69] | General population | 53 | 53 |
|
|
| |
| Tsuruta (2017) [70] | Psoriasis | 55 | 276 | Ever smoker: 24 | Ever smoker: 113 | Ever smoker: 1.12 (0.62, 2.00) | |
| Wibetoe (2017) [71] | RA, AxSpA | 721 |
| Current smoker: 126 |
|
| |
| Krajewska- Włodarczyk (2018)c [72] | Psoriasis | 44 | 51 | Current smoker: 18% | Current smoker: 10% | NSd | |
| Gulati (2016) [73] | General population | 338 | 50 468 | Current smoker: 76 | Current smoker: 8270 | Current smoker: 1.4801 (1.15, 1.9128) | |
| Nas (2015)c [74] | Psoriasis and RA | 173 | Psoriasis: 67RA: 138 | Current smoker: 35.30% | Psoriasis current smoker: 31.3%RA current: 10.1% | NSd | |
| Papagoras (2014)c [75] | AS and Healthy population | 56 | Healthy population: 71AS: 56 | Current smoker: 28.60% | Healthy population current smoker: 18.30%AS current: 60.7% | NSd | |
| Bhole (2012)c [76] | Psoriasis, RA, andGeneral population | 644 | Psoriasis: 448 RA: 350 General population: 115 787 | Ever smoker: 44% | Ever smoker Psoriasis: 48%RA: 60%General population: NR | NSd | |
| Velez (2012)c [77] | Psoriasis | 107 | 161 | Ever smoker: 31.80% | Ever smoker: 39.20% | NSd | |
| Eder (2012) [7] | Psoriasis | 728 | 404 |
|
|
|
|
| Eder (2011) [78] | Psoriasis | 159 | 159 | Ever smoker: 64 | Ever smoker: 89 |
| Ever smoker: 0.52 (0.33, 0.82) |
| Husted (2011)c [79] | Psoriasis | 611 | 449 | Current smoker: 12% | Current smoker: 24.40% | NSd | |
| Tey (2010) [10] | Psoriasis | 134 | 266 |
|
| Current: 0.81 (0.50, 1.32) | |
| Tam (2008) [80] | General population | 82 | 82 | Current smoker: 8 | Current smoker: 0 | Current smoker: 18.82 (1.06, 331.81) | |
| Tam (2008) [81] | General population | 102 | 82 | Current smoker: 9 | Current smoker: 8 | Current smoker: 0.90 (0.33, 2.4336) | |
| Kimhi (2007) [82] | General population | 47 | 100 | 16 | 28 | Smoker: 1.32 (0.63, 2.79) | |
| Pattison (2007) [6] | Psoriasis | 98 | 163 | Ever smoker: 57 | Ever smoker: 102 | Ever smoker: 0.68 (0.39,1.17) | Ever smoker: 0.83 (0.50, 1.39) |
OR (95% CI) numbers that were given in the articles.
OR (95% CI) numbers were calculated by investigators from given results.
Articles that gave only percentages.
Due to insufficient data, the OR could not be calculated. AS: ankylosing spondylitis; AxSpA: axial spondylartritis; NS: not specified; OR: odds ratio; PsA: Psoriatic arthritis; RA: rheumatoid arthritis.
General data extraction
The titles and abstracts were independently screened by two reviewers (U.G.G, G.A.). All abstracts with a discrepancy were carried to a full-text review. The full texts were reviewed independently by the same investigators. Any disagreement at this stage was resolved by the third investigator (S.Z.A). Articles that did not fulfill the inclusion criteria were identified and the reason for exclusion was documented. The control group for the psoriasis arm was subjects without psoriasis. For PsA two control groups were identified, (i) psoriasis and (ii) the general population. The following data were extracted: publication year, study period, country, study design, number of cases and controls, age, gender, and measure of association (univariate and multivariate). The number of both cases and controls was obtained from full texts and odds ratios were calculated by two reviewers independently.
Quality assessment
The National Heart, Lung and Blood Institute of the National Institutes of Health (NIH) tool for quality assessment of Observational Cohort and Cross-Sectional Studies were used to assess the quality of all included studies [83]. The studies were divided into three groups as fair, poor and good by two reviewers independently and the disputes were evaluated by the third reviewer.
Meta-analytic methods
The odds ratios (ORs) and 95% CI for the dichotomous outcome of interest were computed by using a random effects method. All computation was performed with the software Comprehensive Meta-Analysis Version 3.3.070 (Biostat, Inc., Englewood, NJ, USA). Statistical heterogeneity was tested by the Q-test (χ2) and I2 statistic. An I2 value ranges from 0 to 100% and the highest values represents strong heterogeneity [84]. A funnel plot was not utilized to assess the bias of publication since it is suggested to have low power for detecting asymmetry with good accuracy if the number of included studies is below 10, which was the case with our meta-analysis. P-values lower than 0.05 were considered significant [85].
Results
The initial literature search identified 884 psoriasis and 791 PsA articles. After reviewing all abstracts and full texts, 27 and 24 articles met the inclusion criteria for prevalence of psoriasis and PsA, respectively (Supplementary Figs S1 and S2, available at Rheumatology online). Four additional articles were identified with manual scanning of references for PsA. In addition, 25 articles that were identified by Armstrong et al.’s previous meta-analysis were included. For the prevalence of smoking in psoriasis and PsA, the results of 52 and 24 articles are given in Tables 1 and 2, respectively. Of these, 16 articles on psoriasis and three to four (general population and psoriasis) articles on PsA had given clear data on ever smoking and therefore were included in the meta-analysis.
For the incidence of psoriasis and PsA, our search identified one and three studies, respectively, and these were combined with the three studies identified by Armstrong et al. on incident psoriasis (Table 3) [3].
Smoking and incident psoriasis and PsA
| Study | Country | Study population | Study design and period | Smoking ascertainment | Sample size | Smokers that developed PSA or psoriasis | Non-smokers that developed PSA or psoriasis | Measure of association (95% CI) |
|---|---|---|---|---|---|---|---|---|
| Dai (2019) [86] | China | Psoriasis | Prospective cohort, 2001–2015 | NHIS database |
|
|
|
|
| Li (2012) [87] | USA | Psoriasis |
| Questionnaire |
|
| 1124 |
|
| Huerta (2007) [88] | UK | Psoriasis | Prospective cohort, nested case–control analysis, 1996–1997 | OXMIS/read |
| Patients without psoriasis who smoke: 2008 | Patients with psoriasis who smoke: 1013 |
|
| Setty (2007) [89] | USA | Psoriasis | Prospective cohort, 1991–2005 | Questionnaire |
| Current: 131 Former: 262 | 494 |
|
| Nguyen (2018) [8] | UK | PsA | Population-based cohort, 1995–2015 | Medical records |
|
|
|
|
| Li (2012) [9] | USA | PsA | Longitudinal cohort, 1991–2005 | Questionnaire |
|
| Never smoker: 76 |
|
| Green (2020) [90] | PsA | Cohort, 1998–2014 | NR |
| 758 | 644 |
|
| Study | Country | Study population | Study design and period | Smoking ascertainment | Sample size | Smokers that developed PSA or psoriasis | Non-smokers that developed PSA or psoriasis | Measure of association (95% CI) |
|---|---|---|---|---|---|---|---|---|
| Dai (2019) [86] | China | Psoriasis | Prospective cohort, 2001–2015 | NHIS database |
|
|
|
|
| Li (2012) [87] | USA | Psoriasis |
| Questionnaire |
|
| 1124 |
|
| Huerta (2007) [88] | UK | Psoriasis | Prospective cohort, nested case–control analysis, 1996–1997 | OXMIS/read |
| Patients without psoriasis who smoke: 2008 | Patients with psoriasis who smoke: 1013 |
|
| Setty (2007) [89] | USA | Psoriasis | Prospective cohort, 1991–2005 | Questionnaire |
| Current: 131 Former: 262 | 494 |
|
| Nguyen (2018) [8] | UK | PsA | Population-based cohort, 1995–2015 | Medical records |
|
|
|
|
| Li (2012) [9] | USA | PsA | Longitudinal cohort, 1991–2005 | Questionnaire |
|
| Never smoker: 76 |
|
| Green (2020) [90] | PsA | Cohort, 1998–2014 | NR |
| 758 | 644 |
|
HR: hazard ratio; NHIS: The National Health Interview Survey;NR: not reported; OR: odds ratio; OXMIS: The Oxford Medical Information System; PsA: psoriatic arthritis; RR: risk ratio.
Smoking and incident psoriasis and PsA
| Study | Country | Study population | Study design and period | Smoking ascertainment | Sample size | Smokers that developed PSA or psoriasis | Non-smokers that developed PSA or psoriasis | Measure of association (95% CI) |
|---|---|---|---|---|---|---|---|---|
| Dai (2019) [86] | China | Psoriasis | Prospective cohort, 2001–2015 | NHIS database |
|
|
|
|
| Li (2012) [87] | USA | Psoriasis |
| Questionnaire |
|
| 1124 |
|
| Huerta (2007) [88] | UK | Psoriasis | Prospective cohort, nested case–control analysis, 1996–1997 | OXMIS/read |
| Patients without psoriasis who smoke: 2008 | Patients with psoriasis who smoke: 1013 |
|
| Setty (2007) [89] | USA | Psoriasis | Prospective cohort, 1991–2005 | Questionnaire |
| Current: 131 Former: 262 | 494 |
|
| Nguyen (2018) [8] | UK | PsA | Population-based cohort, 1995–2015 | Medical records |
|
|
|
|
| Li (2012) [9] | USA | PsA | Longitudinal cohort, 1991–2005 | Questionnaire |
|
| Never smoker: 76 |
|
| Green (2020) [90] | PsA | Cohort, 1998–2014 | NR |
| 758 | 644 |
|
| Study | Country | Study population | Study design and period | Smoking ascertainment | Sample size | Smokers that developed PSA or psoriasis | Non-smokers that developed PSA or psoriasis | Measure of association (95% CI) |
|---|---|---|---|---|---|---|---|---|
| Dai (2019) [86] | China | Psoriasis | Prospective cohort, 2001–2015 | NHIS database |
|
|
|
|
| Li (2012) [87] | USA | Psoriasis |
| Questionnaire |
|
| 1124 |
|
| Huerta (2007) [88] | UK | Psoriasis | Prospective cohort, nested case–control analysis, 1996–1997 | OXMIS/read |
| Patients without psoriasis who smoke: 2008 | Patients with psoriasis who smoke: 1013 |
|
| Setty (2007) [89] | USA | Psoriasis | Prospective cohort, 1991–2005 | Questionnaire |
| Current: 131 Former: 262 | 494 |
|
| Nguyen (2018) [8] | UK | PsA | Population-based cohort, 1995–2015 | Medical records |
|
|
|
|
| Li (2012) [9] | USA | PsA | Longitudinal cohort, 1991–2005 | Questionnaire |
|
| Never smoker: 76 |
|
| Green (2020) [90] | PsA | Cohort, 1998–2014 | NR |
| 758 | 644 |
|
HR: hazard ratio; NHIS: The National Health Interview Survey;NR: not reported; OR: odds ratio; OXMIS: The Oxford Medical Information System; PsA: psoriatic arthritis; RR: risk ratio.
The prevalence of psoriasis in the general population according to smoking status
The details of the studies on the risk of psoriasis in the general population are given in Table 1 and Supplementary Table S1, available at Rheumatology online. The majority of the studies revealed an increased risk of psoriasis among smokers, both for current smoking (15/26) and ever smoking (15/19). There were only two studies that found a reduced risk. In the meta-analysis, 16 articles were included, with 177 484 psoriasis cases and 827 997 controls, which suggested an increased prevalence of psoriasis among ever smokers (OR: 1.84; 95% CI: 1.4, 2.3) (Fig. 1).
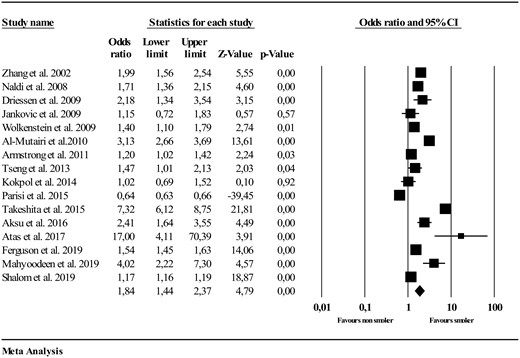
Ever smoking in psoriasis (in comparison with general population)
Smoking and incident psoriasis
Four studies that looked at the effect of incidence of psoriasis among smokers suggested an increased risk of psoriasis (Table 3). Both current and former smoking was found to be a risk factor in the majority of those studies other than one study by Dai et al. in which former smoking was not a risk factor in a multivariate adjusted analysis [86].
The prevalence of psoriatic arthritis in the psoriasis population according to smoking status
The details of the 13 studies on the prevalence of PsA in the psoriasis population are given in Table 2 and Supplementary Table S2, available at Rheumatology online. Six of these studies found a reduced risk of PsA among smokers in the psoriasis patients.
To evaluate the effect of ever smoking on PsA in psoriasis, four articles were included in the meta-analysis with 1785 cases and 5912 controls. Prevalence of PsA was reduced in this group (OR: 0.70; 95% CI: 0.60, 0.81) (Fig. 2).
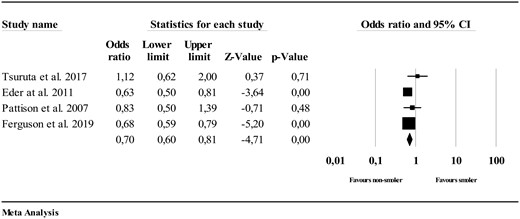
Ever smoking in psoriatic arthritis (in comparison with psoriasis)
The prevalence of psoriatic arthritis in the general population according to smoking status
Twelve studies evaluated the effect of smoking on the risk of PsA within the general population and details are given in Table 2 and Supplementary Table S2 available at Rheumatology online. Half of the studies (6/12) detected an increased risk within the general population.
Three studies were included in the meta-analysis on 4118 and 521 391 controls, which suggested no association between ever smoking and prevalence of PsA compared with the general population (OR: 1.10; 95% CI: 0.92, 1.32) (Fig. 3).
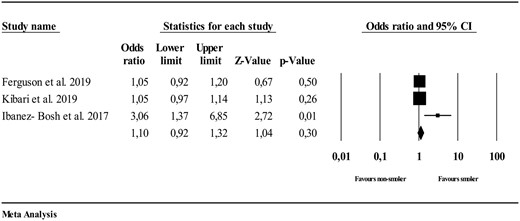
Ever smoking in psoriatic arthritis (in comparison with general population)
Smoking and incident psoriatic arthritis
A total of three publications assessed the relation between smoking and the risk of incident PsA (Table 3). Nguyen et al. showed 1.2- to 1.3-fold increased risk of incident PsA with smoking in the general population [8]. However, current smoking was found to be protective from PsA in the psoriasis population. Li et al. identified increased risk of incident PsA among past or current smokers in the general population [9]. The risk of PsA in psoriasis cases was also linked to smoking intensity and duration, which could only be shown in the heavy smoking group (in current smokers with 15 or more cigarettes per day, with duration of 25 years or more, or 20 or more pack-years). In the third study, Green et al. did not find any significant association in either past or current smoker groups compared with the non-smoking psoriasis population [90].
Quality assessment
In 52 studies in psoriasis, 10 articles were rated as ‘poor’, 27 articles as ‘fair’ and 15 articles as ‘good’. In the 24 studies evaluating in PsA, seven studies were rated as ‘poor’, nine as ‘fair’ and eight as ‘good’ (Supplementary Tables S3–S5, available at Rheumatology online).
Discussion
In this systematic review and meta-analysis, we evaluated the relationship between smoking and psoriasis and PsA. Our results suggest that the prevalence of ever smoking is higher in psoriasis patients compared with the general population. There are biochemical changes associated with smoking such as increase in free radicals activating mitogen-activated protein kinase, nuclear factor κB, and the Janus kinase–signal transducer and activator of transcription pathways [2]. Nicotine also activates the release of various cytokines such as IL-2, IL-12, TNF and granulocyte-macrophage colony-stimulating factor, as well as the stimulation of pathological angiogenesis through overexpression of vascular endothelial growth factor, which may all contribute to the risk of psoriasis [2, 91].
On the other hand, the data on the risk of PsA in psoriasis patients is contradictory. An inverse association between PsA development and smoking in psoriasis is found in a few studies. In Pattison et al.’s study, smokers had ∼50% reduced risk for PsA in psoriasis [6]. Eder et al. also found a reduced risk with smoking and PsA in the psoriasis patients who were HLA-C*06-negative [7]. In a large cohort representative of the UK general population, smoking was negatively associated with PsA among patients with psoriasis [8]. However Tey et al. found no association and Li et al. found that smoking had an increased risk of PsA among patients with psoriasis [9, 10]. Our meta-analysis found that ever smoking is associated with a lower prevalence of PsA among psoriasis. Although the reason for this paradox is not fully understood, there are some potential biological mechanisms. Smoking increases lipid peroxidation and modifies the immune response. It has been proposed that low levels of carbon monoxide in smokers inhibit the expression of pro-inflammatory cytokines (TNF-α, IL-1β, IL-8) and increase IL-10, which was hypothesized to be the reason for a better disease activity among smokers with ulcerative colitis [92]. A similar mechanism may play a role in the development of PsA. Another explanation is that nicotine may be inhibiting intracellular pro-inflammatory pathways through activating α7 nicotinic acetylcholine receptors, which are present in synoviocytes, macrophages and fibroblasts [93, 94].
In addition to these biological pathways to explain this paradox, there are also methodological concerns. The effect of smoking on the development of PsA in the psoriasis group involves a selection bias by definition for including patients who already have been exposed to the increased risk by smoking. To be able to understand the true effect of smoking on the risk of PsA in psoriasis, an inception cohort of psoriasis patients who never smoked needs to be followed prospectively and groups should be compared according to their smoking habits after the onset of psoriasis. Any other connections between psoriasis and PsA are affected by the collider effect, and the risk related to smoking can be misleading.
Alternatively, it is assumed that smokers have a more sedentary life, which may lead to less mechanical stress on the entheses. This may, in theory, lead to a reduced risk of PsA since mechanical loading on the entheses has been demonstrated to be important for the development of SpA [95]. Another potential mechanism can be the effect of smoking on the microbiota by changing the oral flora [96, 97].
It is challenging to evaluate the relationship between the disease and duration and/or intensity of smoking as these are hard to measure. The cessation of smoking may also be relevant as the effect of smoking may be reduced over time. Information on ex-smoking as well as intensity is not clearly reported in the majority of the publications. For that reason, we have summarized all the literature in our tables, but only performed the meta-analysis when ‘ever’-smoking data were clearly provided.
Our study has some limitations. Although the number of articles identified was high for a systemic literature review, only a small group of studies have clearly given numbers on current vs ex-smoking data, which reduced our sample size in the meta-analyses. In addition we evaluated some studies as poor or fair according to quality assessment, but we could not perform a subgroup analysis due to low number of articles and sample size.
In summary our systemic literature review and meta-analysis suggest an increased prevalence of smoking in psoriasis, whereas the prevalence decreases among PsA patients compared with the psoriasis population. Whether smoking cessation neutralizes the risk of developing psoriasis requires a well-defined smoking data collection for past history and this is currently unavailable in the literature.
Funding: No specific funding was received from any funding bodies in the public, commercial or not-for-profit sectors to carry out the work described in this manuscript.
Disclosure statement: The authors have declared no conflicts of interest.
Supplementary data
Supplementary data are available at Rheumatology online.
References
National Heart, Lung, and Blood Institute. Study quality assessment tools. https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (14 April 2020, date last accessed).
Higgins JPT, Green S (editors).

{kind=link}
{kind=link}
{kind=link}
Comments