





Eosinophilic myocarditis processes three stages including the earliest necrotic stage, the intermediate thrombotic stage and the late fibrotic stage. The classic echocardiographic findings include endomyocardial thickening, ventricular thrombus and posterior mitral leaflet involvement eosinophils. Furthermore, cardiac magnetic resonance delayed gadolinium enhancement imaging is capable of detecting myocardial fibrosis and inflammation. Herein, we reported a case of acute right heart failure and the right ventricular outflow tract obstruction, which was caused by eosinophilic myocarditis complicated with thrombus.
Case presentation
A 30-year-old previously healthy man was referred to our hospital for worsening cough, chest tightness and progressive dyspnea 6 days. A physical exam was remarkable due to a holosystolic murmur over the pulmonary artery, and slightly lower extremity edema. Laboratory examinations showed a white blood cell count of 14.01 G/l with eosinophilia (eosinophilic count: 4.56 G/l), elevated levels of C-reactive protein (53.5 mg/l), D-dimer(2.82 mg/l), IgE (>3208.00 IU/ml) and brain natriuretic peptide (3450 pg/ml). Sinus tachycardia with T-wave inversions and right axis deviation were noted on electrocardiogram. Chest radiograph revealed bilateral pleural effusion and right heart enlargement.
Transthoracic echocardiography disclosed a hypoecho mass of the right ventricular outflow tract (RVOT), which was adjacent to the pulmonary valves (Figure 1a). Marked stenosis of RVOT was evident on Doppler ultrasound with the gradient of 42 mmHg (Figure 1b). The flattened ventricular septum, severe right ventricular dilatation and tricuspid regurgitation with a peak gradient of 67 mmHg were also identified by echocardiography due to the marked stenosis of RVOT. And the patient was noted to have decreased right ventricular systolic function (fractional RV area change: 20%), suggesting right heart failure. Cardiac magnetic resonance imaging was completed for better characterization of the mass seen on echocardiogram (Figure 1c). The mass appearance was consistent with thrombus as it had no enhancement, suggesting lack of vascularity. The delayed gadolinium enhanced images showed subendocardial enhancement of the right ventricle. Finally, the patient underwent an emergency operation of thrombectomy for the RVOT obstruction and right heart failure. During surgery, a dense mass was observed in the RVOT (Figure 1d). On pathological examination, the removed mass was confirmed to be a mixed thrombus (Figure 1e), and the adjacent muscle was infiltrated with a large amount of eosinophil (Figure 1f). A final diagnosis of eosinophilic myocarditis complicated by RVOT thrombus was made. A postoperative echocardiography performed 7 days after surgery revealed normal RVOT with a peak gradient of 5 mmHg, mild right heart enlargement and tricuspid regurgitation and elevated right ventricular systolic function. The patient was discharged from the hospital 10 days after surgery and had an uneventful recovery.
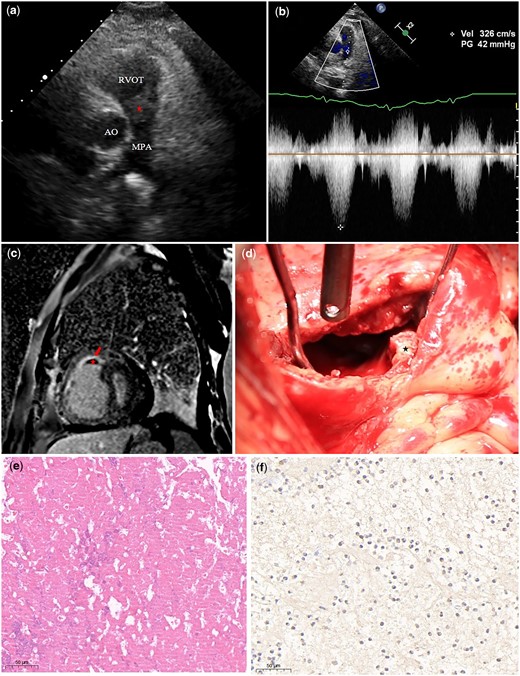
(a) Two-dimensional transthoracic echocardiography shows a hypoechoic mass (asterisk) presenting within the RVOT. (b) Continuous wave Doppler reveals a high velocity jet across the right ventricular outflow tract (obstruction). (c) The delayed gadolinium enhanced CMR images reveal a mass (asterisk) with no enhancement and subendocardial enhancement of the right ventricle (red arrow). (d) Intraoperative image shows a dense mass in RVOT before resection (asterisk). (e) Hematoxylin–eosin stain shows that the mass is composed of trabecular platelets and red blood cell (×20). (f) Immunostaining against the eosinophilic cationic protein confirmed that the adjacent cardiac muscle is infiltrated by a large amount of eosinophil. AO, aorta; MPA, main pulmonary artery; RVOT, right ventricular outflow tract.
Discussion
Eosinophilic myocarditis is a well-known complication in patients with hypereosinophilic syndrome, and it usually processes through three stages.1,2 The earliest acute necrotic stage is generally asymptomatic and diagnosed by biopsy. The intermediate phase is usually accompanied by thrombus formation over the damaged endocardium as seen in our patient, diagnosed by echocardiogram and cardiac magnetic resonance imaging. The late fibrotic stage is defined by the development of subendocardial fibrosis and progressive restrictive cardiomyopathy.3 In our case, the patient experienced clinical heart failure with symptoms of worsening cough, chest tightness and progressive dyspnea due to the obstruction of RVOT thrombus secondary to eosinophilic myocarditis, which has rarely been reported. And cardiac magnetic resonance imaging showed subendocardial delayed gadolinium enhancement, which is a typical finding in eosinophilic myocarditis patients.4 Although pharmacological treatment has been reported as a useful way to treat eosinophilic myocarditis complicated by thrombus,1 surgery excision is a preferred choice in our case because of severe RVOT obstruction and heart failure.
Consent: The patient’s consent for the case report was obtained after well informed.
Conflict of interest. None declared.

{kind=link}