





A 67 year old diabetic woman presented with a three week history of lethargy, general malaise, and episodes of pre-syncope. Past medical history included hypertension, which had been difficult to control. Three months previously, an angiotensin converting enzyme (ACE) inhibitor was prescribed and the dose of atenolol was increased (from 25 mg to 50 mg) in the diabetic outpatient clinic to optimise her blood pressure control. On admission, she looked pale and unwell. Clinical examination revealed signs of congestive heart failure, with a pulse of 30 beats/min (regular) and blood pressure of 104/71 mm Hg. Laboratory investigations revealed a haemoglobin concentration of 101 g/l (normal mean corpuscular volume), urea 37.1 mmol/l, creatinine 422 µmol/l, potassium 5.1 mmol/l, sodium 133 mmol/l, bicarbonate 7 mmol/l. Renal function three months before showed only mild impairment of renal function (urea 11.0 mmol/l, creatinine 155 mmol/l). An electrocardiogram (ECG) showed sinus bradycardia (rate 30 beats/min). Administration of intravenous atropine had little effect on the heart rate. She was treated with intravenous diuretics, renal dose of dopamine (via a central venous line), bicarbonate, and fluid restriction. A temporary pacing wire was inserted into the right ventricle, but failed to capture at 7.5 volts, despite repeated attempts at manipulation in several different positions.
QUESTIONS
What are the possible causes of the renal failure?
What was the likely cause for the sinus bradycardia?
Why did the temporary pacemaker fail to capture?
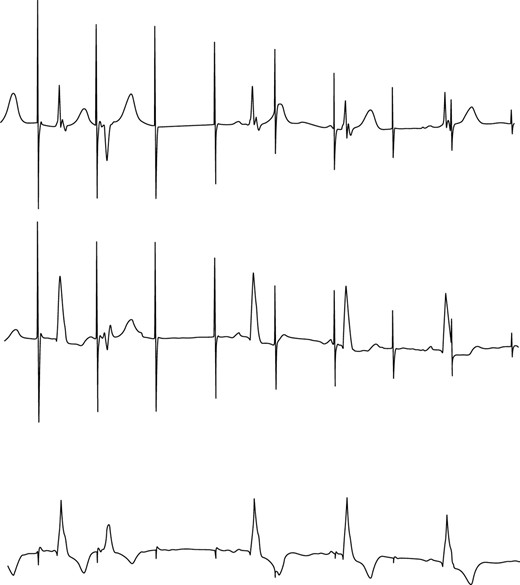
ECG showing failure to capture.

{kind=link}