






Abstract
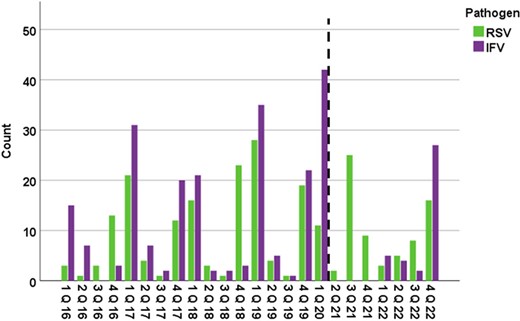
Respiratory viral infections per quarter stratified by viral pathogen.
The dashed line represents the beginning of the COVID-19 era in the USA (March 2020).
Abbreviations: IFV=influenza; Q=quarter; RSV= respiratory syncytial virus.
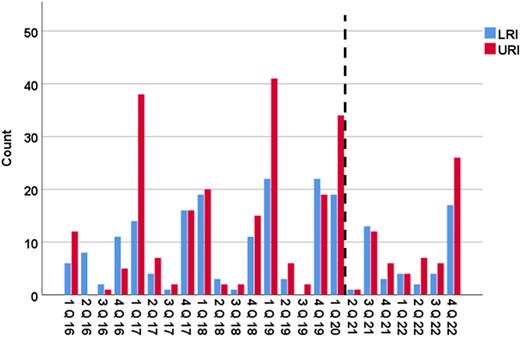
Respiratory viral infections per quarter stratified by site of infection.
The dashed line represents the beginning of the COVID-19 era in the USA (March 2020).
The LRI group includes patients who presented with LRI or progressed from URI to LRI.
Abbreviations: LRI=lower respiratory tract infection; Q=quarter; URI= upper respiratory tract infection
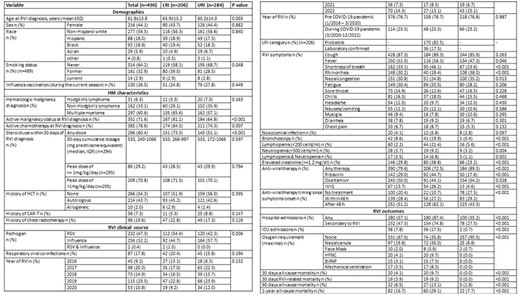
Baseline characteristics and clinical outcomes following respiratory viral infections by site of infection.
Abbreviations: BiPAP= bilevel positive airway pressure; CAR-T= chimeric antigen receptor T-cell therapy; COVID-19=Coronavirus Disease 2019; HCT= hematopoietic stem cell transplantation; HFNC= high-flow nasal cannula; HM= hematologic malignancy; ICU=intensive care unit; IQR= interquartile range; IVIG= Intravenous immunoglobulin; LRI= lower respiratory tract infection; RSV= respiratory syncytial virus; RVI= respiratory virus infection; SD=standard deviation; URI= upper respiratory tract infection.
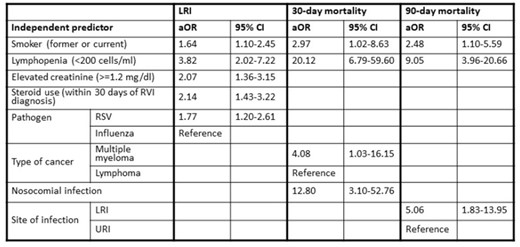
Independent predictors of LRI, 30-day and 90-day mortality by multivariable logistic regression.
Abbreviations: aOR=Adjusted-Odds Ratio; LRI= lower respiratory tract infection; RSV= respiratory syncytial virus; RVI=respiratory tract infection; URI= upper respiratory tract infection; 95% CI= 95% Confidence Interval.
Fareed Khawaja, MBBS, Eurofins Viracor: Grant/Research Support|Symbio: Grant/Research Support Roy F. Chemaly, MD/MPH, AiCuris: Advisor/Consultant|AiCuris: Grant/Research Support|Ansun Pharmaceuticals: Advisor/Consultant|Ansun Pharmaceuticals: Grant/Research Support|Astellas: Advisor/Consultant|Eurofins-Viracor: Grant/Research Support|InflaRX: Advisor/Consultant|Janssen: Advisor/Consultant|Karius: Advisor/Consultant|Karius: Grant/Research Support|Merck/MSD: Advisor/Consultant|Merck/MSD: Grant/Research Support|Moderna: Advisor/Consultant|Oxford Immunotec: Advisor/Consultant|Oxford Immunotec: Grant/Research Support|Roche/Genentech: Advisor/Consultant|Roche/Genentech: Grant/Research Support|Shinogi: Advisor/Consultant|Takeda: Advisor/Consultant|Takeda: Grant/Research Support|Tether: Advisor/Consultant
Author notes
Study Group:
Session: 65. Respiratory Infections - Viral
Thursday, October 17, 2024: 12:15 PM


{kind=link}
Comments