






Abstract


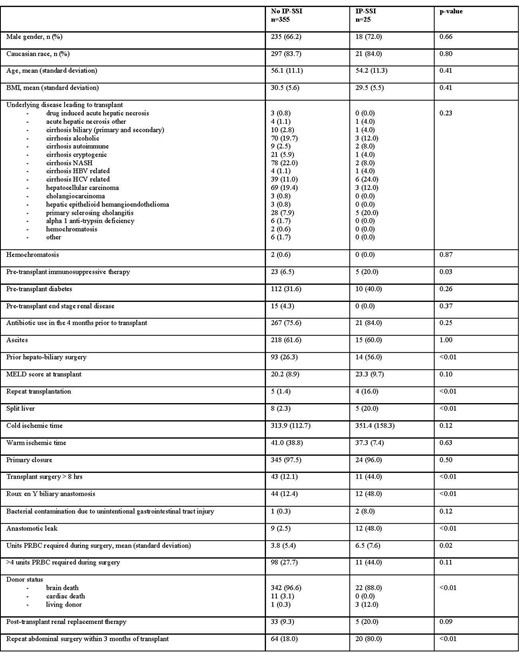
Baseline characteristics of adult patients who underwent a single liver transplant at Duke University Hospital in the period 1 Jan 2015 - 31 Dec 2019 stratified by the diagnosis of invasive primary surgical site infection (IP-SSI) within 90 days of transplant surgery. BMI, body mass index; HBV, hepatitis b virus; HCV, hepatitis c virus; MELD, model for end-stage liver disease; NASH, non-alcoholic steatohepatitis; PRBC, packed red blood cells

The overall IP-SSI rate in our cohort is low compared to published literature supporting effectiveness of current antimicrobial prophylaxis. In this setting, factors that portend risk for IP-SSI are related to the surgical procedures, thus are not easily modifiable. Patients with repeat transplantation, Roux-en-Y biliary anastomosis, anastomotic leak, and repeat abdominal surgery within 3 months of transplantation must be monitored closely for development of IP-SSI. However, the appropriateness of current prophylaxis regimens should be further evaluated given the high prevalence of drug-resistant pathogens causing breakthrough IP-SSI.
Matt Harris, PharmD, MHS, wolters kluer: Advisor/Consultant Barbara D. Alexander, MD, F2G Pharmaceuticals: Advisor/Consultant|HealthTrackRx: Advisor/Consultant|HealthTrackRx: Board Member|Leadiaint: Grant/Research Support|Merck: Advisor/Consultant|Scynexis: Grant/Research Support|Thermofisher: Advisor/Consultant
Author notes
Session: 145. HAI: Surgical Site Infections
Friday, October 13, 2023: 12:15 PM


{kind=link}
Comments