






Abstract
Outcomes for patients with lower-grade gliomas (LrGGs) continue to improve with advances in molecular characterization and treatment. However, cognitive sequela from the tumor and its treatment leave a significant impact on health-related quality of life for these patients. Several factors affect each patient’s cognition, such as tumor location, treatment, medication, and comorbidities. However, impairments of processing speed, attention, concentration, working memory, and executive function are common across LrGG patients. Cognitive rehabilitation strategies, well established in traumatic brain injury and stroke populations, are based on neural plasticity and functional reorganization. Adapting these strategies for implementation in patients with brain tumors is an active area of research. This article provides an overview of cognitive domains commonly impaired in LrGG patients and evidence for the use of cognitive rehabilitation strategies to address these impairments with the goal of improving health-related quality of life in this patient population.
Survival for patients with lower-grade diffuse gliomas (LrGGs)–grades II and III—is improving, with a median survival of 5 to 15 years1–5 depending on molecular subtype.6,7 However, these tumors and their related treatments often lead to significant objective and subjective cognitive impairments8–13 that negatively affect patients’ health-related quality of life (HRQOL).14 The reported prevalence of cognitive impairments in LrGG varies widely.15 At presentation, before any treatment (including surgery), 31% to 75% of patients report cognitive impairments11,16 and these are more common with dominant hemispheric lesions.17 Though some cognitive recovery usually occurs within 3 to 6 months of surgery,18–20 19% to 83% of LrGG patients remain impaired or decline further.11,15,21,22
The mechanisms of cognitive impairment in brain tumors, including LrGGs, are multifactorial (Figure 1). The impact of the tumor and its associated treatments can lead to the functional disruption of distributed cognitive networks.10,23–27 Tumor biology, extent of edema, tumor volume, and higher grade have been linked to brain tumor–related cognitive impairment.8,10,11 Isocitrate dehydrogenase mutation, a feature commonly seen in LrGG, correlates with fewer cognitive deficits at presentation and slower lesion momentum over time.10 Standard adjuvant tumor treatments, such as radiotherapy and chemotherapy, are associated with diminished cognition. Radiotherapy affects both the cerebral vasculature and white-matter tracts contributing to demyelination, thickening of vessel walls, focal mineralization, and coagulative necrosis.25 These changes have been linked to cognitive decline that may continue to evolve several years after radiotherapy.28,29 Chemotherapy also has neurotoxic effects on cognition through development of acute and chronic encephalopathy.25,30 In a rodent study of temozolomide, a commonly used alkylating agent in glioma treatment, neurogenesis in the hippocampus was decreased with a negative impact on memory encoding and learning.31 Use of steroid or pain medications, high seizure burden, and several antiepileptic drugs may also exacerbate cognitive inefficiencies.25,32,33

Factors that influence cognitive impairment in lower-grade glioma (LrGG) patients.
Cognitive rehabilitation is considered a well-established treatment to address cognitive impairments in many neurologic diseases such as traumatic brain injury (TBI), multiple sclerosis, and stroke.34–37 Cognitive rehabilitation “is a systematically applied set of medical and therapeutic services designed to improve cognitive functioning and participation in activities that may be affected by difficulties in one or more cognitive domains.” 38 Further, these services are designed to enhance cognitive abilities, particularly as it relates to improving functional independence and HRQOL.36,38 Cognitive rehabilitation is based on principles of neural plasticity and functional reorganization39,40 with 2 main underlying mechanisms: 1) retraining and 2) functional compensation.35,41–43 Retraining strengthens impaired cognitive skills through repeatedly practicing cognitive tasks,44 whereas functional compensation focuses on honing strategies to modify the environment and/or one’s approach to achieve a goal.41,45 These 2 interventional approaches are often combined,46–49 with compensation being particularly appropriate for treating persistent cognitive impairments.35,36,50
Cognitive rehabilitation typically is informed by neuropsychological assessment and implemented in 3 phases: 1) Acquisition—education about cognitive vulnerabilities and strengths, and beginning to learn possible compensatory strategies; 2) Application—applying learned compensatory strategies in stages toward mastery; and 3) Adaptation—applying prior learned skills with enhanced complexity to aid functional improvement (Figure 2).36,51 Cognitive rehabilitation strategies are increasingly being investigated and applied in brain tumor patients, particularly in LrGG patients with improving survival.
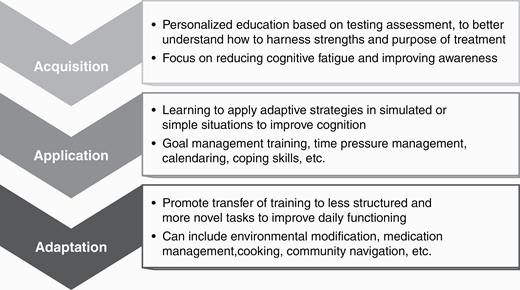
The “Triple A” Model of Cognitive Rehab: 1, Acquisition; 2, Application; and 3, Adaptation.
Common Domains of Cognitive Impairment and Related Cognitive Rehabilitation Strategies in Lower-Grade Glioma Patients
The prevalence of cognitive impairment in LrGG varies across affected domains, particularly those reliant on distributed functional networks and intact white-matter tracts, rather than highly localized cognitive skills.52 LrGG patients commonly demonstrate cognitive impairments in attention and concentration,52,53 processing speed,14,21,52 learning and memory,14,54 and executive functions.14,20,21,53 Recent studies of cognitive rehabilitation strategies to address these impairments have demonstrated feasibility and efficacy in patients with brain tumors (Table 1).35,36,46–50,55–60 However, there are limited studies in LrGG patients alone because most studies include a mixture of low- and high-grade gliomas, as well as meningiomas and metastatic lesions.55,56 The following is an overview of the most common cognitive impairments and related rehabilitation strategies used in brain tumors with an emphasis on data relevant to patients with LrGG. Though we focus on improvement in the targeted cognitive domain, studies support improvements across multiple cognitive domains after rehabilitation, as reflected in Table 1.48 We also discuss practical considerations for implementation.
Cognitive Rehabilitation Studies in Gliomas
| Reference | Study design and intervention | Targeted cognitive domain(s) | Outcome | Sample | |
|---|---|---|---|---|---|
| Combined cognitive retraining and compensation strategies | Gehring et al, 200947 | RCT in lower-grade gliomas | Attention, executive functioning, learning, and memory | At 6 mo: improved attention, verbal memory, and mental fatigue | Total = 140 |
| Intervention: 2 h weekly for 6 sessions including iPad app | Low-grade glioma = 117 | ||||
| Control: wait-list | Anaplastic glioma = 23 | ||||
| van der Linden et al, 201848 | Feasibility RCT in postoperative primary brain tumors | Attention, executive functioning, learning, and memory | Feasibility: 54% met feasibility criteria defined as ≥ 80% completion of retraining and compensation strategies | Total = 13 | |
| Intervention: 3 h weekly for 10 sessions using iPad | Low-grade glioma = 4 | ||||
| Control: wait-list | Meningioma = 7 | ||||
| Other = 2 | |||||
| Zucchella et al, 201349 | RCT in primary brain tumors postoperatively | Orientation, attention, memory, and executive functioning | At 1 mo: improved verbal memory, visual attention | Total = 53 | |
| Intervention: 4 h weekly for 16 sessions | Low-grade glioma = 7 | ||||
| Control: usual care without cognitive training | High-grade glioma = 25 | ||||
| Meningioma = 16 | |||||
| Other = 5 | |||||
| Compensation strategies | Hassler et al, 201059 | Pilot study in glioblastomas and anaplastic gliomas | Perception, concentration, attention, verbal learning and memory, retentiveness, and creativity | At 12 wk: improved verbal learning | Total = 11 |
| Intervention: 10 group sessions of 90 min of compensation (holistic mnemonic training) | Glioblastoma = 7 | ||||
| Anaplastic glioma = 4 | |||||
| Locke et al, 200860 | Primary brain tumors undergoing radiation with caregivers | Executive functioning, learning and memory | At 3 mo: 88% patients using strategies at least once per wk | Total = 13 | |
| Intervention: 50 min daily for 6 sessions of cognitive rehabilitation and problem-solving therapy intervention | Glioma = 11 | ||||
| Control: usual care without cognitive training | Meningioma = 2 | ||||
| Miotto et al, 201361 | Pilot study in untreated primary frontal lobe tumors | Verbal learning and memory, working memory, executive functioning | At 30 min: improved verbal memory | Total = 21 | |
| Intervention: 30 min of strategic semantic organizational training | Glioma = 12 | ||||
| Meningioma = 9 | |||||
| Miotto et al, 201462 | Pilot study in low-grade glioma of left frontal lobe | Verbal learning and memory | At 30 min: improved verbal memory | Total = 9 | |
| Intervention: 30 min of strategic semantic organizational training | Low-grade glioma = 9 | ||||
| Control: matched healthy volunteers | |||||
| Richard et al, 201957 | Pilot RCT in brain tumors | Executive and related attention, memory, and behavioral impairments | At 4 mo: improved HRQOL, executive function, processing speed | Total = 25 | |
| Intervention: 2 h weekly for 8 sessions (GMT or BHP) | Low-grade glioma = 8 | ||||
| Control: wait-list | High-grade glioma = 6 | ||||
| Meningioma = 7 | |||||
| Other = 4 | |||||
| Cognitive retraining | Maschio et al, 201546 | Pilot study in brain tumors | Memory, attention, visuospatial functions, language, and reasoning | Immediately and at 6 mo: improved attention, memory, and verbal fluency | Total = 16 |
| Intervention: 1 h weekly retraining for 10 sessions | Low-grade glioma = 5 | ||||
| Anaplastic glioma = 4 | |||||
| Glioblastoma = 2 | |||||
| Meningioma = 2 | |||||
| Metastases = 3 | |||||
| Yang et al, 201458 | RCT VR for retraining in brain tumors | Attention, learning, and memory | At 1 mo: improved attention, memory, and visual motor coordination, visual learning, and memory | Total = 38 | |
| Intervention: 1.5 h weekly VR retraining and 1 h weekly computer-assisted cognitive rehabilitation for 4 wks | Astrocytoma = 2 | ||||
| Control: 2.5 h weekly of computer-assisted cognitive rehabilitation for 4 wk | Glioblastoma = 5 | ||||
| Meningioma = 10 | |||||
| Metastasis = 6 | |||||
| Other = 15 |
| Reference | Study design and intervention | Targeted cognitive domain(s) | Outcome | Sample | |
|---|---|---|---|---|---|
| Combined cognitive retraining and compensation strategies | Gehring et al, 200947 | RCT in lower-grade gliomas | Attention, executive functioning, learning, and memory | At 6 mo: improved attention, verbal memory, and mental fatigue | Total = 140 |
| Intervention: 2 h weekly for 6 sessions including iPad app | Low-grade glioma = 117 | ||||
| Control: wait-list | Anaplastic glioma = 23 | ||||
| van der Linden et al, 201848 | Feasibility RCT in postoperative primary brain tumors | Attention, executive functioning, learning, and memory | Feasibility: 54% met feasibility criteria defined as ≥ 80% completion of retraining and compensation strategies | Total = 13 | |
| Intervention: 3 h weekly for 10 sessions using iPad | Low-grade glioma = 4 | ||||
| Control: wait-list | Meningioma = 7 | ||||
| Other = 2 | |||||
| Zucchella et al, 201349 | RCT in primary brain tumors postoperatively | Orientation, attention, memory, and executive functioning | At 1 mo: improved verbal memory, visual attention | Total = 53 | |
| Intervention: 4 h weekly for 16 sessions | Low-grade glioma = 7 | ||||
| Control: usual care without cognitive training | High-grade glioma = 25 | ||||
| Meningioma = 16 | |||||
| Other = 5 | |||||
| Compensation strategies | Hassler et al, 201059 | Pilot study in glioblastomas and anaplastic gliomas | Perception, concentration, attention, verbal learning and memory, retentiveness, and creativity | At 12 wk: improved verbal learning | Total = 11 |
| Intervention: 10 group sessions of 90 min of compensation (holistic mnemonic training) | Glioblastoma = 7 | ||||
| Anaplastic glioma = 4 | |||||
| Locke et al, 200860 | Primary brain tumors undergoing radiation with caregivers | Executive functioning, learning and memory | At 3 mo: 88% patients using strategies at least once per wk | Total = 13 | |
| Intervention: 50 min daily for 6 sessions of cognitive rehabilitation and problem-solving therapy intervention | Glioma = 11 | ||||
| Control: usual care without cognitive training | Meningioma = 2 | ||||
| Miotto et al, 201361 | Pilot study in untreated primary frontal lobe tumors | Verbal learning and memory, working memory, executive functioning | At 30 min: improved verbal memory | Total = 21 | |
| Intervention: 30 min of strategic semantic organizational training | Glioma = 12 | ||||
| Meningioma = 9 | |||||
| Miotto et al, 201462 | Pilot study in low-grade glioma of left frontal lobe | Verbal learning and memory | At 30 min: improved verbal memory | Total = 9 | |
| Intervention: 30 min of strategic semantic organizational training | Low-grade glioma = 9 | ||||
| Control: matched healthy volunteers | |||||
| Richard et al, 201957 | Pilot RCT in brain tumors | Executive and related attention, memory, and behavioral impairments | At 4 mo: improved HRQOL, executive function, processing speed | Total = 25 | |
| Intervention: 2 h weekly for 8 sessions (GMT or BHP) | Low-grade glioma = 8 | ||||
| Control: wait-list | High-grade glioma = 6 | ||||
| Meningioma = 7 | |||||
| Other = 4 | |||||
| Cognitive retraining | Maschio et al, 201546 | Pilot study in brain tumors | Memory, attention, visuospatial functions, language, and reasoning | Immediately and at 6 mo: improved attention, memory, and verbal fluency | Total = 16 |
| Intervention: 1 h weekly retraining for 10 sessions | Low-grade glioma = 5 | ||||
| Anaplastic glioma = 4 | |||||
| Glioblastoma = 2 | |||||
| Meningioma = 2 | |||||
| Metastases = 3 | |||||
| Yang et al, 201458 | RCT VR for retraining in brain tumors | Attention, learning, and memory | At 1 mo: improved attention, memory, and visual motor coordination, visual learning, and memory | Total = 38 | |
| Intervention: 1.5 h weekly VR retraining and 1 h weekly computer-assisted cognitive rehabilitation for 4 wks | Astrocytoma = 2 | ||||
| Control: 2.5 h weekly of computer-assisted cognitive rehabilitation for 4 wk | Glioblastoma = 5 | ||||
| Meningioma = 10 | |||||
| Metastasis = 6 | |||||
| Other = 15 |
Abbreviations: BHP, Brain Health Program; GMT, Goal Management Training; HRQOL, health related quality of life; RCT, randomized controlled trial; VR, virtual reality.
Cognitive Rehabilitation Studies in Gliomas
| Reference | Study design and intervention | Targeted cognitive domain(s) | Outcome | Sample | |
|---|---|---|---|---|---|
| Combined cognitive retraining and compensation strategies | Gehring et al, 200947 | RCT in lower-grade gliomas | Attention, executive functioning, learning, and memory | At 6 mo: improved attention, verbal memory, and mental fatigue | Total = 140 |
| Intervention: 2 h weekly for 6 sessions including iPad app | Low-grade glioma = 117 | ||||
| Control: wait-list | Anaplastic glioma = 23 | ||||
| van der Linden et al, 201848 | Feasibility RCT in postoperative primary brain tumors | Attention, executive functioning, learning, and memory | Feasibility: 54% met feasibility criteria defined as ≥ 80% completion of retraining and compensation strategies | Total = 13 | |
| Intervention: 3 h weekly for 10 sessions using iPad | Low-grade glioma = 4 | ||||
| Control: wait-list | Meningioma = 7 | ||||
| Other = 2 | |||||
| Zucchella et al, 201349 | RCT in primary brain tumors postoperatively | Orientation, attention, memory, and executive functioning | At 1 mo: improved verbal memory, visual attention | Total = 53 | |
| Intervention: 4 h weekly for 16 sessions | Low-grade glioma = 7 | ||||
| Control: usual care without cognitive training | High-grade glioma = 25 | ||||
| Meningioma = 16 | |||||
| Other = 5 | |||||
| Compensation strategies | Hassler et al, 201059 | Pilot study in glioblastomas and anaplastic gliomas | Perception, concentration, attention, verbal learning and memory, retentiveness, and creativity | At 12 wk: improved verbal learning | Total = 11 |
| Intervention: 10 group sessions of 90 min of compensation (holistic mnemonic training) | Glioblastoma = 7 | ||||
| Anaplastic glioma = 4 | |||||
| Locke et al, 200860 | Primary brain tumors undergoing radiation with caregivers | Executive functioning, learning and memory | At 3 mo: 88% patients using strategies at least once per wk | Total = 13 | |
| Intervention: 50 min daily for 6 sessions of cognitive rehabilitation and problem-solving therapy intervention | Glioma = 11 | ||||
| Control: usual care without cognitive training | Meningioma = 2 | ||||
| Miotto et al, 201361 | Pilot study in untreated primary frontal lobe tumors | Verbal learning and memory, working memory, executive functioning | At 30 min: improved verbal memory | Total = 21 | |
| Intervention: 30 min of strategic semantic organizational training | Glioma = 12 | ||||
| Meningioma = 9 | |||||
| Miotto et al, 201462 | Pilot study in low-grade glioma of left frontal lobe | Verbal learning and memory | At 30 min: improved verbal memory | Total = 9 | |
| Intervention: 30 min of strategic semantic organizational training | Low-grade glioma = 9 | ||||
| Control: matched healthy volunteers | |||||
| Richard et al, 201957 | Pilot RCT in brain tumors | Executive and related attention, memory, and behavioral impairments | At 4 mo: improved HRQOL, executive function, processing speed | Total = 25 | |
| Intervention: 2 h weekly for 8 sessions (GMT or BHP) | Low-grade glioma = 8 | ||||
| Control: wait-list | High-grade glioma = 6 | ||||
| Meningioma = 7 | |||||
| Other = 4 | |||||
| Cognitive retraining | Maschio et al, 201546 | Pilot study in brain tumors | Memory, attention, visuospatial functions, language, and reasoning | Immediately and at 6 mo: improved attention, memory, and verbal fluency | Total = 16 |
| Intervention: 1 h weekly retraining for 10 sessions | Low-grade glioma = 5 | ||||
| Anaplastic glioma = 4 | |||||
| Glioblastoma = 2 | |||||
| Meningioma = 2 | |||||
| Metastases = 3 | |||||
| Yang et al, 201458 | RCT VR for retraining in brain tumors | Attention, learning, and memory | At 1 mo: improved attention, memory, and visual motor coordination, visual learning, and memory | Total = 38 | |
| Intervention: 1.5 h weekly VR retraining and 1 h weekly computer-assisted cognitive rehabilitation for 4 wks | Astrocytoma = 2 | ||||
| Control: 2.5 h weekly of computer-assisted cognitive rehabilitation for 4 wk | Glioblastoma = 5 | ||||
| Meningioma = 10 | |||||
| Metastasis = 6 | |||||
| Other = 15 |
| Reference | Study design and intervention | Targeted cognitive domain(s) | Outcome | Sample | |
|---|---|---|---|---|---|
| Combined cognitive retraining and compensation strategies | Gehring et al, 200947 | RCT in lower-grade gliomas | Attention, executive functioning, learning, and memory | At 6 mo: improved attention, verbal memory, and mental fatigue | Total = 140 |
| Intervention: 2 h weekly for 6 sessions including iPad app | Low-grade glioma = 117 | ||||
| Control: wait-list | Anaplastic glioma = 23 | ||||
| van der Linden et al, 201848 | Feasibility RCT in postoperative primary brain tumors | Attention, executive functioning, learning, and memory | Feasibility: 54% met feasibility criteria defined as ≥ 80% completion of retraining and compensation strategies | Total = 13 | |
| Intervention: 3 h weekly for 10 sessions using iPad | Low-grade glioma = 4 | ||||
| Control: wait-list | Meningioma = 7 | ||||
| Other = 2 | |||||
| Zucchella et al, 201349 | RCT in primary brain tumors postoperatively | Orientation, attention, memory, and executive functioning | At 1 mo: improved verbal memory, visual attention | Total = 53 | |
| Intervention: 4 h weekly for 16 sessions | Low-grade glioma = 7 | ||||
| Control: usual care without cognitive training | High-grade glioma = 25 | ||||
| Meningioma = 16 | |||||
| Other = 5 | |||||
| Compensation strategies | Hassler et al, 201059 | Pilot study in glioblastomas and anaplastic gliomas | Perception, concentration, attention, verbal learning and memory, retentiveness, and creativity | At 12 wk: improved verbal learning | Total = 11 |
| Intervention: 10 group sessions of 90 min of compensation (holistic mnemonic training) | Glioblastoma = 7 | ||||
| Anaplastic glioma = 4 | |||||
| Locke et al, 200860 | Primary brain tumors undergoing radiation with caregivers | Executive functioning, learning and memory | At 3 mo: 88% patients using strategies at least once per wk | Total = 13 | |
| Intervention: 50 min daily for 6 sessions of cognitive rehabilitation and problem-solving therapy intervention | Glioma = 11 | ||||
| Control: usual care without cognitive training | Meningioma = 2 | ||||
| Miotto et al, 201361 | Pilot study in untreated primary frontal lobe tumors | Verbal learning and memory, working memory, executive functioning | At 30 min: improved verbal memory | Total = 21 | |
| Intervention: 30 min of strategic semantic organizational training | Glioma = 12 | ||||
| Meningioma = 9 | |||||
| Miotto et al, 201462 | Pilot study in low-grade glioma of left frontal lobe | Verbal learning and memory | At 30 min: improved verbal memory | Total = 9 | |
| Intervention: 30 min of strategic semantic organizational training | Low-grade glioma = 9 | ||||
| Control: matched healthy volunteers | |||||
| Richard et al, 201957 | Pilot RCT in brain tumors | Executive and related attention, memory, and behavioral impairments | At 4 mo: improved HRQOL, executive function, processing speed | Total = 25 | |
| Intervention: 2 h weekly for 8 sessions (GMT or BHP) | Low-grade glioma = 8 | ||||
| Control: wait-list | High-grade glioma = 6 | ||||
| Meningioma = 7 | |||||
| Other = 4 | |||||
| Cognitive retraining | Maschio et al, 201546 | Pilot study in brain tumors | Memory, attention, visuospatial functions, language, and reasoning | Immediately and at 6 mo: improved attention, memory, and verbal fluency | Total = 16 |
| Intervention: 1 h weekly retraining for 10 sessions | Low-grade glioma = 5 | ||||
| Anaplastic glioma = 4 | |||||
| Glioblastoma = 2 | |||||
| Meningioma = 2 | |||||
| Metastases = 3 | |||||
| Yang et al, 201458 | RCT VR for retraining in brain tumors | Attention, learning, and memory | At 1 mo: improved attention, memory, and visual motor coordination, visual learning, and memory | Total = 38 | |
| Intervention: 1.5 h weekly VR retraining and 1 h weekly computer-assisted cognitive rehabilitation for 4 wks | Astrocytoma = 2 | ||||
| Control: 2.5 h weekly of computer-assisted cognitive rehabilitation for 4 wk | Glioblastoma = 5 | ||||
| Meningioma = 10 | |||||
| Metastasis = 6 | |||||
| Other = 15 |
Abbreviations: BHP, Brain Health Program; GMT, Goal Management Training; HRQOL, health related quality of life; RCT, randomized controlled trial; VR, virtual reality.
Attention/Concentration
A majority of everyday functions rely on one’s ability to direct, divide, and sustain attention to aid task completion.63 Attentional abilities interact with many other cognitive domains, and improvements in attention can increase overall cognitive processing.64 Selective attention, or the ability to focus on chosen stimuli while ignoring distractions, is often susceptible to effects of brain disorders, including tumors.63,65 Other aspects of attention, such as sustaining a state of mental concentration over a period of time and/or dividing attention between tasks, are also more challenging following brain disease or injury.63
Attention often declines after glioma surgery,17 and though there is evidence suggesting improvement by 3 to 6 months,9 deficits persist and recovery to presurgical baselines can be tenuous. A variety of treatments and other issues common to brain tumor patients negatively affect attention and concentration, including radiotherapy. A study of low-grade glioma patients treated with radiotherapy vs not found a significant decline in attention with a mean follow-up of 12 years after diagnosis.66 Some antiepileptic drugs are associated with impairments in attention.67 Fatigue and low mood, reported in 42% of low-grade glioma patients following surgery,13 can also contribute to diminished arousal and vigilance, which are needed for attentional focus.68,69
To address attentional issues, emerging studies in brain tumor populations support a combination of cognitive retraining and compensatory strategy training,35,36,70–72 such as fatigue management, relaxation strategies, and pacing education, along with focus on self-awareness and problem solving to reduce attentional lapses.36,73,74 Several studies have demonstrated feasibility with cognitive retraining and compensatory strategy training in LrGG patients with positive cognitive outcomes.47,48 A randomized controlled trial of 6 weekly cognitive rehabilitation sessions (2 hours of combined retraining and compensatory strategy training) vs a waiting-list control group in LrGG demonstrated improvements in brief attention (and verbal memory) at 6 months post intervention.47 Attention-retraining techniques in this study focused on sustained, selective, alternating, and divided attention, whereas compensatory strategy training (didactic and experiential learning) focused on cognitive education, improving awareness, and relaxation strategies.47 An additional study of combined retraining and compensatory strategies in patients with high- and low-grade glioma and meningioma after surgery found significant improvements in visual attention (and verbal memory) at 1 month post intervention compared to a control group.49 The compensatory strategies in the latter study were modeled after work by Cicerone et al35 with metacognitive training (see “Executive Functioning” for more details) and education to improve self-awareness and management of attentional lapses.
In clinical practice, the multidimensional nature of attentional impairments, often identified during neuropsychological testing, necessitates a tailored interventional approach.36,64 Attentional arousal and focus may be addressed by reducing environmental distractors, self-cuing to aid focus, and working in well-lit environments,73,74 whereas difficulty in divided attention is commonly addressed by focusing on sufficient time for response, developing organizational strategies, and doing one task at a time.35,36
Processing Speed
Processing speed usually refers to the speed at which cognitive operations can be performed,75 and is thought of as an interaction between specific cognitive skills, reaction speed, and stimulus transmission.76 Cognitive skills that are more automatic require less processing speed for execution,77 whereas novel and difficult cognitive tasks require higher concerted effort, and thus produce slower processing speed times.76 When processing is slow, completion of tasks in a satisfactory way becomes more challenging.78 Higher-order or more complex tasks, such as abstraction or integration of information, are especially difficult with slower processing as several sources of information are needed simultaneously.78 Processing speed is highly vulnerable to brain injury76 and is seen frequently in LrGG patients.67 Primary brain tumor patients frequently describe mental slowness,79,80 which can lead to frustration when they are unable to keep up with the pace of task demands (eg, conversations and watching television).36,72 Processing speed impairments are particularly associated with damage to cerebral white matter and subcortical systems, as commonly seen in LrGG and from treatment such as radiation.79,80 Certain antiepileptic drugs33 and comorbid psychiatric conditions76,78 may also reduce processing speed.
Rehabilitation strategies to address processing speed impairments focus on compensatory strategy training, including preplanning, problem solving, and improving awareness to more effectively cope with time pressure demands. These strategy training strategies are well established in TBI and stroke, and may be applicable for use with LrGG.36,47,72,81 Clinically, a time pressure management strategy training is commonly used to improve awareness and restructure problem solving before and during a task to reduce time pressure demands.36,72,81 Time pressure management training builds awareness of how slowed thinking negatively affects daily functioning, and emphasizes the importance of performing one task at a time and preplanning to reduce in-the-moment pressure demands. For example, when driving to a new place, patients would be encouraged to study the route in advance, prepare their belongings, and consider setting an alarm to ensure a timely departure. Then during driving, they would focus on keeping ample distance between cars, turning off the radio, and minimizing conversation. If they become overwhelmed they could pull over, use relaxation strategies, and rereview their route when they are calmer. Elements of this approach were integrated into Gehring’s cognitive rehabilitation study with LrGG with an overall positive study benefit.47
Learning and Memory
Memory is a not a single operation, but rather consists of several systems dependent on intact functioning of various cognitive domains.63,82 The impact of neurological insult on memory depends on factors such as anatomical location, treatment, and disease course.69 Patients with left hemispheric gliomas were shown to be more impaired in immediate and delayed verbal recall vs those with intraventricular and posterior fossa tumors prior to surgery.54 Memory impairment is also seen in gliomas involving the thalamus, frontal, and temporal lobes.54 Postoperatively, diminished memory functioning is common in LrGG, with verbal memory impairments noted in 40% to 60% of patients with low-grade gliomas following awake surgery.13 Attention and working memory, which are essential in learning and remembering new information, are vulnerable to impairment following radiotherapy.63,66,83 High fraction dose, in particular, is associated with reduced learning and long-term memory storage capacity.67 Further, chemotherapy may affect hippocampal neurogenesis and learning of new information.31
Rehabilitation interventions focused on memory impairments tend to be broad, given the complexity of memory processes.82,84 Notably, executive impairments also interrupt strategic encoding and memory retrieval85 and are commonly incorporated into memory strategy training.36 A study in brain tumor patients (56% of whom had LrGGs), of 10-week cognitive retraining with exercises in memory, attention, visuospatial functions, language, and reasoning, found immediate improvements in attention, memory, and verbal fluency that were sustained at 6-month follow-up.46 Virtual reality cognitive retraining was also shown in brain tumors (5% of patients with low-grade gliomas) to improve attention, memory, and visual-motor coordination.58
Clinically, it is important to account for the nature and severity of the patient’s memory impairments to guide the rehabilitation approach. Internal memory strategies focus on mentally manipulating information to aid recall (eg, mnemonics, grouping, and semantic categorization), whereas external memory strategies focus on organizational prosthetics.84,86,87 Studies of patients with prefrontal brain tumors after 30 minutes of internal strategy training (semantic categorization) found significantly improved memory with increased contralateral activation seen on functional MRI.61,62 Another study demonstrated improvements in verbal memory in high-grade gliomas after 10 weeks of internal strategy training (mnemonics).59 External memory aids such as written lists, calendaring, labeling, designated places for items, increasing daily structure, notebooks and planners, and alarms show promise for LrGG.47
Executive Functioning
Executive impairments can affect the ability to form and execute goal-directed behavior,88–91 problem solving, and self-monitoring, and can lead to significant negative functional impact.63,89,91,92 Impairments in executive functioning—such as disorganization, cognitive inflexibility, and difficulty planning and multitasking—are particularly common in glioma patients. A meta-analysis of cognitive functioning in 313 glioma patients found postsurgical improvements in complex attention, language, and verbal memory, whereas executive function declined immediately after resection and persisted at 6 months.20
From a rehabilitation perspective, there is emerging evidence for improving executive functioning using metacognitive rehabilitation strategies. Metacognitive training focuses on improving awareness, self-monitoring, and attentional control to more effectively perform daily tasks.93–95 A systematic review in TBI found the greatest improvement when metacognitive approaches were combined with systematic problem-solving interventions,37 and this combination is a promising strategy for managing executive dysfunction in brain tumor populations as well.35,36
A study of patients with primary brain tumors (including 32% low- and 24% high-grade gliomas) found significant improvements in executive functioning using 8-week compensatory metacognitive strategy training combined with brain tumor education, compared to education alone.57 The training and education included exercises for improving awareness of dysexecutive symptoms, monitoring cognitive problems, and applying learned strategies to day-to-day activities. Significant between-group effects were noted at the 4-month posttreatment follow-up, though no immediate posttreatment effects were noted.57 An additional study of patients with primary brain tumors (including LrGG) found that 88% reported problem-solving strategies as helpful and continued to use the intervention 3 months after treatment.60
In clinical practice, compensatory strategy training focused on improving organization and problem solving is often helpful. Routinizing daily tasks,49 linking naturally behaviors together (eg, taking medications with meals), systematic problem solving,57 and optimizing existing organizational strategies47 hold promise for brain tumor patients.36,64,96,97
Language
Patients with gliomas located in the dominant hemisphere often perform worse on cognitive measures of language, verbal learning, and verbal intelligence.98 However, slowed and incoherent speech may also be present in patients with tumors located in the nondominant hemisphere.99 In a study of presumed LrGG patients with dominant-hemisphere tumors, performance was worse on tests of lexical retrieval (object naming and verbal fluency), whereas no impairments in language were found for those with nondominant tumors.100 Although advanced surgical techniques (ie, intraoperative mapping and monitoring) are leading to increased language preservation,22 full recovery from aphasia after resection may not be achieved for all LrGG patients.
In clinical practice, cognitive rehabilitation strategies for general populations with aphasia often focus on improvement in conversational skills, reading comprehension, and language formation.64,101,102 Anomia (a common linguistic complaint among high- and low-grade glioma patients17) is commonly addressed via compensatory strategy training focused on verbal circumlocution, paced speech, associative cuing, and semantic feature analysis (although efficacy is unclear in LrGG).35,103,104 Environmental interventions, such as supportive communication strategy training for caregivers to improve HRQOL by managing expectations and perceptions, have clear support in TBI and stroke, but have yet to be studied in brain tumor populations.105,106
Practical Clinical Considerations
In alignment with the UK National Institutes of Clinical Excellence guidelines for supportive care for adults living with cancer, the rehabilitation needs of patients should be assessed from a multidisciplinary perspective at key points in the disease course.107 This model also has emerging evidence for effectiveness and feasibility in the management of patients with high- and low-grade gliomas.108–110 A prospective, randomized study of 6 to 8 weeks of intensive ambulatory multidisciplinary rehabilitation vs a wait-list control group of brain tumor patients demonstrated improvements in self-care at 3 months.110 Improvements were also noted in psychosocial interactions, communication, and cognitive abilities (problem solving, memory), which were maintained at 6 months.110
For clinicians and health care professionals working with these patients, considering systematic cognitive screening and actively managing comorbidities that exacerbate cognitive issues are important first steps. By asking patients (and caregivers) early and often about neuropsychological and behavioral changes and related distress, cognitive needs are more likely to be detected early and better managed. A referral to neuropsychology and thorough neuropsychological assessment in patients with suspected cognitive impairment are crucial to identify undertreated neuropsychological symptoms and inform rehabilitation treatment planning. There are no current consensus guidelines about the optimal timing for cognitive intervention in glioma patients. However, given the multiple factors that affect cognition (see Figure 1), cognitive rehabilitation should be considered during periods of psychiatric and medical stability, and after recovery from intensive treatments, such as radiation.56 Cognitive rehabilitation aims to reduce the gap between patients’ demands and abilities by applying the principles and strategies discussed earlier, to learn new ways to achieve their desired goals (Figure 3).
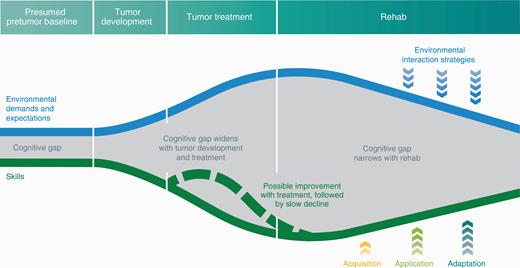
Schema of Longitudinal Trajectory of Cognitive Impairment Across Disease Trajectory.
The blue line represents environmental demands and expectations such as work, school, and family responsibilities. The green line depicts the patient’s current cognitive skills such as attention/concentration, processing speed, memory, and executive functioning. The gray space between environmental demands and cognitive skills is the cognitive gap. The gap is narrow at “Presumed pretumor baseline” because the patient is well equipped with cognitive skills to manage his or her environmental demands and expectations. During “Tumor development,” the gap widens as skills decline and demands increase. The gap widens further with “Tumor treatment” given that the impact of surgery, radiotherapy, and chemotherapy on cognitive skills and environmental demand increases with factors such as returning to work after treatment. The dotted green line reflects natural recovery of cognitive skills after surgery. With “Rehab,” the gap is narrowed by improving cognitive skills using the Triple A model. Concurrently, environmental demands and expectations are decreased through environmental interaction strategies such as work accommodation, school accommodation, and managing family and patient performance expectations.
Additional factors such as higher seizure burden, certain antiepileptic drugs,33 steroids, and pain medications25,32 may also negatively affect mood and cognitive function. Consideration should be given to alternative antiepileptic drugs and/or referral to psychiatry when appropriate. Sleep issues and fatigue also exacerbate cognitive symptoms, and identifying and treating underlying causes (such as sleep apnea), and discussing sleep hygiene, emotional stressors, exercise, self-pacing education, and pharmacologic management should also be considered.68 Referrals to other care partners such as psychiatry/psychology, speech language pathology, and occupational therapy help to comanage cognitive and emotional symptoms.
Conclusion
As advances in molecular characterization and improvement in treatment extend survival for LrGG patients, increasing attention is being paid to cognitive outcomes and their effect on HRQOL. Impairments in attention, processing speed, learning and memory, executive functioning, and language, commonly experienced by patients with LrGG, often reduce their HRQOL. Results of emerging research of cognitive rehabilitation hold promise for addressing these concerns in LrGG, though there are a number of limitations. Establishing the natural history of cognition over the LrGG disease trajectory is challenged by methodological variability in the literature with a lack of uniform cognitive test batteries, difficulty with study attrition, and smaller sample sizes of heterogeneous histologies captured at varying time points.20 As neuro-oncology moves toward an integrated diagnosis of molecular characterization with histology, there are even fewer data establishing these trajectories among molecular subtypes.
The efficacy and generalizability of cognitive rehabilitation strategies are also confounded by variability in test batteries and assessment intervals, lack of control groups, and limited data from randomized trials.111 These limitations complicate our ability to develop a consensus regarding the cognitive needs and related treatments for brain tumor patients, and optimizing timing for intervention.111 Recently published guidelines for standardizing neuropsychological endpoints across cancer,112 including neuro-oncology,113 highlight the importance of addressing these issues and provide foundational work for investigating cognitive rehabilitation approaches in LrGG. Establishing more prospective data to optimize cognitive rehabilitation strategies and the timing of intervention (including strategies for network-based impairments) aligns with the increasing focus on cancer survivorship (including the development of survivorship care plans in neuro-oncology).114 Current challenges to implementation include a scarcity of qualified rehabilitation providers, lack of awareness about the role of cognitive rehabilitation, payer source issues, and underdetection and treatment of compounding mood and cognitive issues. Future considerations include systematic cognitive screening and development of novel telehealth interventions to increase access to care. To this end, we and others are exploring novel cognitive rehabilitation approaches using technology and self-monitoring tools to address some of these barriers (NCT03948490).
Funding
This work was supported by the LoGlio Collective [to all authors]; the Sheri Sobrato Brisson Brain Cancer Fund [to C.W.J., S.C, and S.H.J.]; the Robert Wood Johnson Foundation [grant number 74259 to S.H.J.]; and the National Institute of Neurological Disorders and Stroke [grant number K08 110919-01 to S.H.J.]
Acknowledgments
The authors thank N. Sirivansanti and K. Probst for their artistic support.
Conflict of interest statement. None declared.

{kind=link}
{kind=link}
{kind=link}