





Abstract
C3 glomerulopathy (C3G) is a clinical-pathological entity resulting from dysregulation of the alternative pathway of the complement system (APC) in the fluid phase. The recurrence risk of C3G after kidney transplantation is about 70% with high risk of graft loss. Standard treatment relies on nephroprotection and unspecific immunosuppression but there are currently new molecules that target specifically APC under development. A novel factor B inhibitor, iptacopan, has shown promising results both in native kidney and transplant recurrence cases in a phase II trial.
We present a real-world clinical case of early C3G recurrence after kidney transplantation treated with iptacopan (Novartis MAPs program). Patient was vaccinated for encapsulated bacteria. Iptacopan was initiated 200 mg BID. We also present histological response.
38-year-old male with chronic kidney disease secondary to C3G initially presented with nephrotic syndrome and hematuria at the age of 31y following a respiratory infection. Blood test showed low serum C3 levels and the presence of C3 nephritic factor without pathological genetic alterations. Kidney biopsy confirmed membranoproliferative glomerulonephritis (MPGN) with predominant C3 deposition. He progressed to CKD stage G5 requiring hemodialysis instead of nephroprotection and immunosuppression with corticosteroids and mycophenolate; and addition with cyclophosphamide and rituximab after 19 months from onset.
Five years later, the patient was admitted as first kidney transplant recipient from deceases donor Maastricht-III. Induction therapy included thymoglobulin, and tacrolimus, mycophenolate, and corticosteroids. He experienced delayed graft function requiring hemodialysis. An early biopsy proved C3G recurrence with endocapillary proliferation without C4d deposit and absence of donor specific antibodies. Despite conventional immunosuppression and addition of rituximab and plasma exchange; hemodialysis requirement still be present. So, because C3G pathophysiological base, iptacopan was begun with successful clinical response as he reached hemodialysis discontinuation; and kidney function stabilized after one year of treatment with an estimated glomerular filtration rate about 30 mL/min/1.73 m2.
In the follow-up biopsy 5 months later, deposit of C3 in the glomerulus disappeared compared to the post-transplant recurrence but with persistence of endocapillary and mesangial proliferation (see Fig. 1).
However, interestingly, he experienced a clinical recurrence with acute kidney injury and hematuria after unintentional iptacopan discontinuation, which was resolver after reinitiating and recovering its previous graft function. No infectious complications were observed after one year of treatment with factor B inhibitor.
New molecules under development that specifically target APC (fluid phase) may change the treatment scenario of C3G and its recurrence in kidney transplantation. We expose a real-practice early C3G recurrence after kidney transplantation successfully treated with iptacopan. The patient reached kidney function stabilization and disappearance of C3 deposits on immunofluorescence of the follow-up biopsy, identical results as the phase II clinical trial of iptacopan in C3G. So, we might conclude that iptacopan is an effective and safe option for C3G recurrence after kidney transplantation. But, data from randomized studies are needed in order to confirm the efficacy and safety of new inhibitors of the APC as iptacopan.
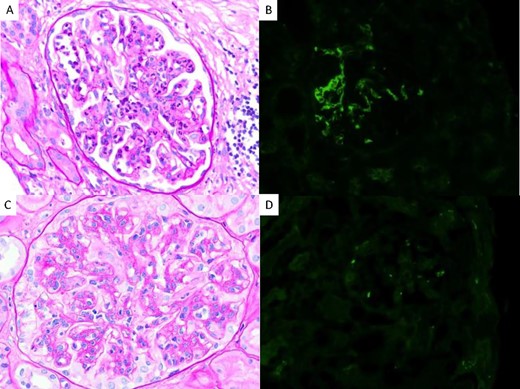
Case 1: kidney transplant biopsies. Superior: first biopsy with C3GP recurrence diagnosis. (A-B) Light microscopic showing endocapilar proliferation (A), periodic acid-Schiff (PAS). (B) Immunofluorescence with strong C3 deposition. Inferior: biopsy control after 5 months of iptacopan beginning. (C-D) Light microscopic with persistent endocapillary proliferation with mesangial proliferation and presence of double contours pattern, PAS. (D) Immunofluorescence with C3 impregnation but no significant deposits. Original magnification, × 100 in A, B, C, D.


{kind=link}
Comments