





Abstract
This study evaluates an integrated care program for chronic kidney disease (CKD), which has demonstrated effectiveness in delaying kidney function decline in the rural population of Thailand. Efficacy of the program was initially established through the ESCORT-1 study, a cluster-randomized controlled trial (doi: 10.1186/s12882-016-0414-4), and further demonstrated the effectiveness by the larger-scale prospective cohort study, ESCORT-2 (doi: 10.1111/nep.13849). The aim of this study is to assess the cost-effectiveness of incorporating this program into Thailand's public health benefit package, with the goal of establishing it as a model for similar rural areas in resource-limited settings.
Following the Thailand's guideline for health technology assessment, a cost-utility analysis utilizing data from the ESCORT studies, local databases, and literatures. The integrated care program was tailored to primary healthcare system by using preexisting workforces. It involved a collaboration between Multi-Disciplinary Care Teams (MDCT) at district hospitals and Community Care Network (CCN) teams at Sub-District Health Centers (SDHC). The MDCT, comprising general practitioners, CKD nurse managers, pharmacists, a nutritionist, and a physical therapist, provided key patient education on diet, medication adherence, exercise, and avoiding certain medications and herbal remedies. The CCN teams, including community nurses and village health volunteers, conducted home visits for health monitoring and lifestyle guidance. Both MDCT and CCN personnel received training in CKD care based on the NKF-K/DOQI and KDIGO Clinical Practice Guidelines. A decision-analytic Markov model and Monte-Carlo simulation were applied to quantify and compare the lifetime costs and quality-adjusted life years (QALY) outcomes of the intervention and conventional-care from a societal perspective considering both direct and indirect costs. The analysis included extensive sensitivity analyses, incorporating a probabilistic model and scenario-analyses based on patient ages, CKD stages, and varying program efficacy. Additionally, a budget impact analysis from the payer's perspective assessed the financial impact and affordability over a five-year period.
The integrated care program was found to dominate conventional care. The results indicated an incremental cost-effectiveness of (-)278,000 Thai Baht (∼7,267 EUR) per QALY for the base case analysis. Probabilistic analysis demonstrated consistent outcomes, with the integrated care program being cost-effective at almost 100% of the time during analysis at the 160,000 Thai Baht (∼4,182 EUR) willingness-to-pay threshold (Fig. 1). These results are driven by significant cost savings due to reduced time and overall costs in dialysis before death. The program is most cost-effective when provided early to patients, in terms of both age and CKD stages (Fig. 2). The budget impact analysis showed that introducing the intervention could save the payer 184 billion Thai Baht (4.76 billion EUR) over five years. (The exchange rate; 1 Thai Baht = 38.26 EUR)
The integrated care program for patients with stage 3-4 CKD is cost-effective and suitable for inclusion in Thailand's health benefit package, mainly due to its significant cost savings and enhanced health outcomes. The program's design, focusing on sustainability and feasibility by utilizing existing workforces, positions it as a viable model for similar economic and healthcare contexts, especially in resource-limited countries.
![Results of the probabilistic sensitivity analysis simulation in a cost-effectiveness plane (vertical axis = incremental cost [Thai baht], horizontal axis = incremental QALY gained [years], and red line represent the 160,000 Thai Baht (∼4,182 EUR) willingness-to-pay threshold) [1 Thai baht = 38.26 EUR].](https://oup.silverchair-cdn.com/oup/backfile/Content_public/Journal/ndt/39/Supplement_1/10.1093_ndt_gfae069.715/2/m_gfae069_0715_1381fig1.jpeg?Expires=1748689331&Signature=4CLn7~TM7pL-V1kZRRHEaV9dLgfJYJirqGlqOQ-CFxir~RxlKXdu38bxU2TLyLo3v-sJIKi6QKAuOvAGqeyY7rbyWnQFF4bEzRiEYjUdKoDMdgCmk57IgBpuCy9z7xZZ0JZ7AUzTGA3TCYAXdGapNDXBzcLyUJACx6-A8pEv8exr7ZHaRcZHn4bacEq99S7z0VeDnf3MxGf5DLeAM92sE1DHQay31gXfC0-Isb0BtpRgBRTwvKz3y-idn04F1nJY6OA3Aw1JoaXYOBIrag8bv8AtZMIrXqDjmBas0EgZNQLHT60v1nPnynVqI1qUDi~w0BOGzfberYjvLAzqBue30w__&Key-Pair-Id=APKAIE5G5CRDK6RD3PGA)
Results of the probabilistic sensitivity analysis simulation in a cost-effectiveness plane (vertical axis = incremental cost [Thai baht], horizontal axis = incremental QALY gained [years], and red line represent the 160,000 Thai Baht (∼4,182 EUR) willingness-to-pay threshold) [1 Thai baht = 38.26 EUR].
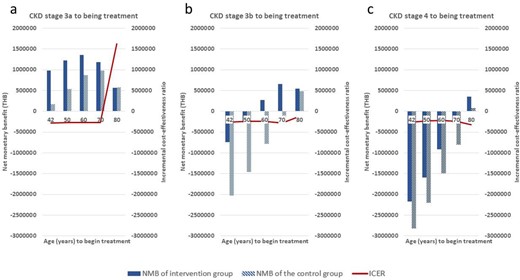
Scenario analysis when treatment begins in (a) CKD stage 3a, (b) stage 3b, and (c) stage 4; Horizontal axis: patient's age; Left axis/Bar chart = Net monetary benefit (THB; 1 THB = 38.26 EUR), Right axis/Red line = Incremental cost-effectiveness ratio.


{kind=link}
Comments