





Abstract
Primary and secondary hyperoxaluria is characterized by significantly elevated urinary oxalate levels, increased risk of kidney stones, nephrocalcinosis, and chronic kidney disease. Patients with enteric hyperoxaluria are especially at high-risk populations. However, identifying hyperoxaluric individuals within these populations remains challenging due to difficulties in obtaining complete urine collections. This study aims to evaluate the diagnostic performance of the urine oxalate/creatinine ratio to improve the screening of hyperoxaluria.
We pooled data from an adult tertiary renal exploration center, including living donors, short bowel syndrome patients, bariatric surgery patients, and individuals with nephrolithiasis or other nephrological issues undergoing 24-hour urine analysis. We assessed the relationship between the urine oxalate/creatinine ratio and 24-hour oxalate excretion. The diagnostic performance of the ratio was analyzed using ROC curves, and an optimal diagnostic threshold was established.
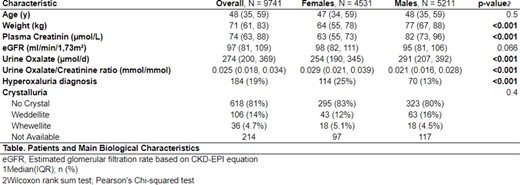
Of the 1485 initially included adult patients reported in Table 1, 37% lacked complete urine collections, resulting in a study population of 974 individuals (453 females, 521 males, median age 48 years, median renal function 97 ml/min/1.73 m²). Nineteen percent had hyperoxaluria, with a higher prevalence in females (25% vs. 13% in males). Median 24-hour oxaluria was 548 (432,740) µmol/d in the diseased group and 244 (188,309) µmol/d in the healthy group. A strong correlation (Spearman's rank correlation rho= 0.8, p < 0.001) was found between the urine oxalate/creatinine ratio and 24-hour oxalate excretion. ROC curves for both genders exhibited similar performance, with an optimal threshold for the entire population yielding an AUC of 0.97 (0.962-0.981). The diagnostic threshold for maximum sensitivity was an oxalate/creatinine ratio of 0.025 mmol/mmol (Sensitivity = 1, Specificity = 0.65, PPV = 0.4, NPV = 1), while for maximum specificity, it was an oxalate/creatinine 0.074 mmol/mmol (Sensitivity= 0.31, Specificity = 1, PPV = 1, NPV = 0.862). The optimal diagnostic threshold chosen by the minimum distance from the left-upper corner was an oxalate/creatinine 0.034 mmol/mmol (Sensitivity= 0.92, Specificity = 0.91, PPV = 0.69, NPV = 0.98) (Fig. 1).
The urine oxalate/creatinine ratio demonstrates excellent diagnostic performance and is efficient in screening hyperoxaluric patients within high-risk populations. However, the positive predictive value is insufficient to be a standalone reliable diagnostic test. Therefore, 24-hour urine oxalate measurement remains necessary for diagnosis.
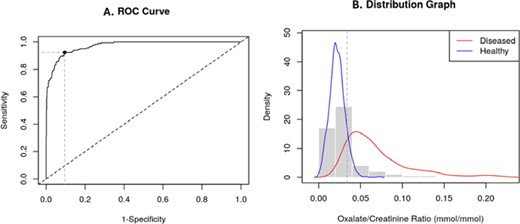
Diagnosis performance of 0.034 mmol/mmol oxalate/creatinine urine ratio. A. ROC curve; B. Distribution graphic.
Patients and main biological characteristics. eGFR, estimated glomerular filtration rate based on CKD-EPI equation; 1. Median (IQR); n (%); 2. Wilcoxon rank sum test, Pearson's Chi-squared test.
Patients and main biological characteristics. eGFR, estimated glomerular filtration rate based on CKD-EPI equation; 1. Median (IQR); n (%); 2. Wilcoxon rank sum test, Pearson's Chi-squared test.


{kind=link}
Comments