





Abstract
Cardiopulmonary recirculation (CRP) is one of the most informative instrumental parameters, widely used to predict adverse cardiovascular events in patients on maintenance hemodialysis (HD). CRP calculation is based on two indirectly measured estimates: AVF volume blood flow (Qa) and cardiac output (CO). Large CRP variability may cause underestimation of cardiovascular risk in many HD patients.
We aimed to study the inter- and inner-observer agreement of Qa and CO. As a second step, we studied the changes in Qa, CO and CPR before and after HD.
The prospective study included 88 patients with native AVF. At the first step, we evaluated the inter- and inner-observer agreement of Qa measurement with color duplex ultrasound (Bland–Altman plots, Figure 1A–D). Two specialists with 5–7 years of experience measured Qa twice on brachial artery, twice on fistula vein.
To estimate the maximum relative error in paired measurements we calculated the mean and the absolute mean difference for each pair. Then, the absolute mean difference was divided by mean; the greatest deviations from the average are given in %.
After that, they measured CO twice before HD and once after HD. Ultrafiltration during HD was 1.6 ± 0.34 L.
We observed a good concordance between Qa measurements on brachial artery by one specialist (Figure 1A) and by two specialists (Figure. 1B): deviations were [–13.9%; 13.1%] and [–18.3%; 16.4%], respectively. There was a poor concordance between assessments on brachial artery and fistula vein (Figure 1C), and Qa measurement on fistula vein alone (Figure 1 D). In the latter case, the variance was very high even if measurements were performed by one specialist: deviations were [–37.9%; 39.6%] and [–59.3%; 93.6%], respectively. In all cases, the systematic bias was low, but the deviations were significantly different between measurement methods. The variance of bias increased along with increasing of Qa.
We observed a good concordance between CO assessments made by one specialist and between specialists: deviations were [–12.4%; 12.3%] and [–10.5%; 9.1%], respectively.
The main pitfall of CPR-based cardiovascular risk stratification is that CO changes significantly after HD (Fig. 2A), while Qa values remain relatively stable (Figure 2B): although Qa difference before and after HD is statistically significant, it seems to be modest.
Median CO decrease after HD was 13.4% (26.6% max), while median of Qa decrease was 1.7% (6.1% max).
This leads to a significant increase of CPR value after HD, which can reach 40%(! ) in some patients (absolute increase of 0.11) (Figure. 2C).
CPR value more than 30% is considered to be an indication for Qa reduction. In our cohort, 17% of the patients had CPR >30% before HD and 42% after HD.
Qa assessment should be performed only on brachial artery. There is a significant decrease in CO after HD even if ultrafiltration was moderate, whereas Qa remains relatively stable. This leads to a significant increase of CPR value in some patients after HD. CPR assessment before HD may lead to underestimation of cardiovascular risk. The decision on Qa reduction to decrease CPR should be based on CPR assessment after HD session.
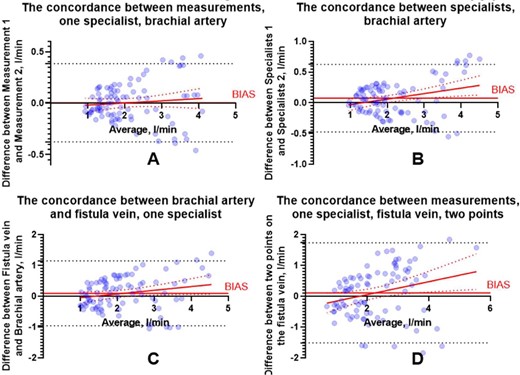
The inter- and inner-observer agreement of AVF volume blood flow (Qa).
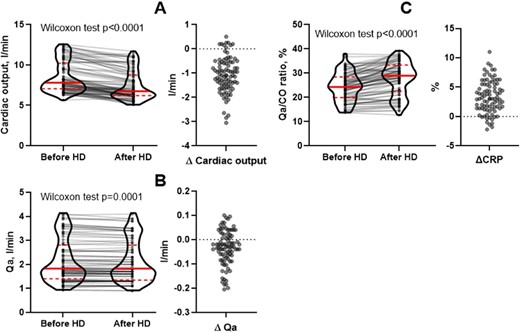
Changes in CO, Qa and Qa/CO ratio (CPR) before and after hemodialysis session.


{kind=link}
Comments