





Abstract
We aimed to analyze the outcomes of HD patients with COVID-19 hospitalized in the Moscow region, Russia, and to compare it with those in the general population.
Data were obtained retrospectively from the Moscow region COVID-19 register database, which comprises all hospitalizations with suspected or confirmed COVID-19 between February 2020 and November 2021. A total of 384 327 patients were included; 1 435 of them were ESRD patients.
Among ESRD patients there were 1386 HD patients and 49 kidney graft recipients.
Thus, during the specified period, 48.5% of all prevalent HD patients of the Moscow region and only 7.8% of the graft recipients required hospitalization. Due to a few number of hospital admissions among kidney recipients they were excluded from the further analyses.
We observed typical 4 waves of hospital admissions in the general population, but not in HD patients. In these patients, we noted a peak in December 2020 with a subsequent decrease in February, 2021; then the number of hospitalizations remained stable. The proportion of HD patients was approximately 0.5% of all patients with COVID-19 admitted to hospital. Almost all HD patients with COVID-19 were hospitalized regardless of disease severity.
The mean age of hospitalized HD patients was significantly more than that in the general population: 68.95 ± 13.69 years versus 59.18 ± 17.11 years, P < 0.001. Of note, the mean age of HD patients in Russia is 56.3 ± 11.7 years. The proportion of men among hospitalized HD patients with COVID-19 reached 50.4% versus 43.5% in the general population.
HD was associated with a significant increase in the risk of critical but stable and extremely critical (+ worsened: terminal and clinical death) condition at admission (Figure 1A): RR = 3.36 [95% confidence interval (95% CI) 3.12–3.59], P < 0.001 and RR = 4.83 (95% CI 3.93–5.92), P < 0.001, respectively.
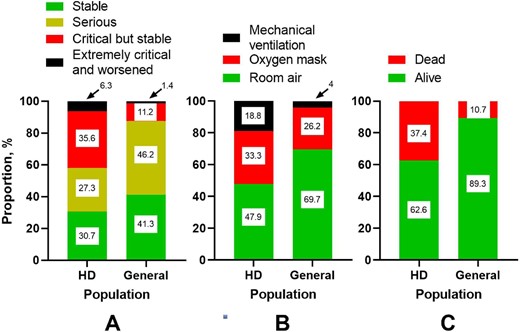
Distribution of HD patients and patients in general population according to their condition upon admission (A), oxygen supplementation requirement (B) and outcome (C).
HD patients were significantly more likely to need for any kind of respiratory support (oxygen mask and mechanical ventilation (MV)) or MV alone (Figure 1B): RR = 1.72 (95% CI 1.63–1.81), P < 0.001 and RR = 4.67 (95% CI 4.18–5.21), P < 0.001, respectively.
HD was associated with a significant increase in the risk of death (Figure 1C): RR = 3.48 (95% CI 3.24–3.72), P < 0.001.
HD significantly increased the risk of death in patients without oxygen support and in patients with need for an oxygen mask (Figure 2A): RR = 3.56 (95% CI 2.97–4.25), P < 0.001 and RR = 2.47 (95% CI 2.18–2.78), P < 0.001, respectively. For patients requiring MV, mortality was >95% in both cohorts: RR = 0.999 (95% CI 0.955–1.01), P = 0.309.
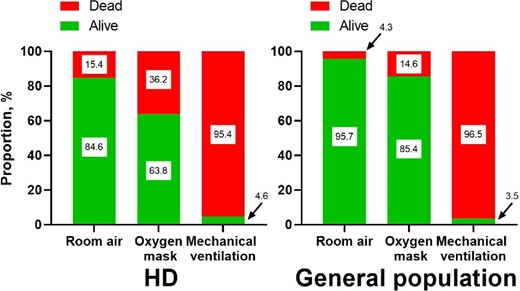
Outcomes in HD patients (on the left) and patients in the general population (on the right) due to respiratory support requirement.
Deceased patients were older than survivors both in HD patients [73 (IQR 65–82) versus 69 (IQR 59–78) years; P < 0.001] and in the general population [72 (IQR 63–82) versus 60 (IQR 48–69) years; P < 0.001], however, the difference between medians was significantly greater in the general population: 13 (95% CI 12–14) versus 5 (95% CI 3–6) years.
Heart and lung diseases increased the risk of death. In the general population concomitant heart diseases worsened the prognosis to a greater extent compared with lung diseases: RR = 2.69 (95% CI 2.64–2.74), P < 0.001 and RR = 1.3 (95% CI 1.26–1.35), P < 0.001, respectively. In HD patients pre-existing lung diseases had a greater impact on the risk of death than heart diseases: RR = 2.02 (95% CI 1.71–2.41), P < 0.001 and RR = 3.05 (95% CI 2.73–3.41), P < 0.001, respectively.
In the multivariate model, significant predictors of death in HD patients were need for MV (OR = 9.81, 95% CI 8.48–17.8; P < 0.001) and lung diseases (OR = 2.92, 95% CI 1.92–5.42; P < 0.001], but not heart diseases, age and gender.
HD patients with COVID-19 have a significantly worse prognosis compared with the general population. The main risk factors for death are need for respiratory support and pre-existing lung diseases.


{kind=link}
Comments