





Abstract
Spontaneous Renal Artery Dissection (SRAD) is a rare and often unrecognized clinical entity, which only accounts for 1-2% of all arterial dissections. Due to its rarity, it may be difficult to diagnose and treat.
All patients affected by SRAD and admitted in our Unit in the last year were included.
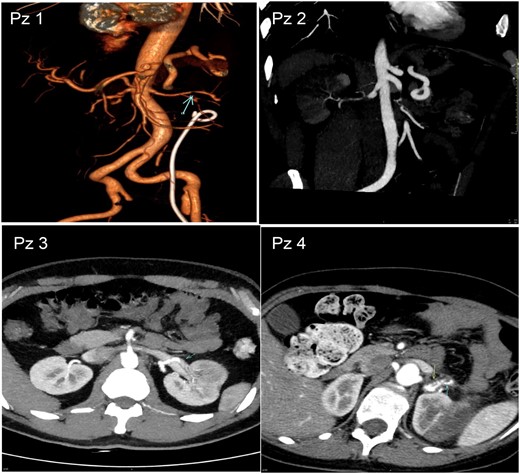
Five patients presented with renal infarction due to SRAD were admitted in our Unit in 2020. Patient Characheristics are shown in Table 1. At onset, all suffered from abdominal pain and high blood pressure. In all patients renal function was normal. Abdomen computed tomography angiography (CTA) was diagnostic in all patients (Figure 1). They were treated with antihypertensive drugs and systemic anticoagulation followed by oral anticoagulants. At 3 month-follow-up, all patients became normotensive and partial or total renal artery recanalization were found (Figure 2).

Abdominal CTA of 4 patients with SRAD at onset
Abdominal CTA of 4 patients with SRAD after therapy
Patient Characteristics at onset.
| Patient | Sex | Age (years) | Blood Pressure (mmHg) | SRAD | Comobidities | Cerebral MRI/CT |
|---|---|---|---|---|---|---|
| 1 | F | 61 | 150/100 | Left segmental branch anterior inferior and Right renal artery | Kidney stones | negative |
| 2 | M | 49 | 150/90 | Right renal artery | Severe cardiovascular familiarity, GIST | negative |
| 3 | M | 39 | 140/90 | Left segmental antero-inferior renal artery | Severe cardiovascular familiarity, OFP ostium II | negative |
| 4 | F | 51 | 145/85 | Left renal artery | Dolicocolon | Carotid-oftalmic aneurism |
| 5 | M | 50 | 150/100 | Right and left renal artery | Family history for tumors | negative |
| Patient | Sex | Age (years) | Blood Pressure (mmHg) | SRAD | Comobidities | Cerebral MRI/CT |
|---|---|---|---|---|---|---|
| 1 | F | 61 | 150/100 | Left segmental branch anterior inferior and Right renal artery | Kidney stones | negative |
| 2 | M | 49 | 150/90 | Right renal artery | Severe cardiovascular familiarity, GIST | negative |
| 3 | M | 39 | 140/90 | Left segmental antero-inferior renal artery | Severe cardiovascular familiarity, OFP ostium II | negative |
| 4 | F | 51 | 145/85 | Left renal artery | Dolicocolon | Carotid-oftalmic aneurism |
| 5 | M | 50 | 150/100 | Right and left renal artery | Family history for tumors | negative |
Patient Characteristics at onset.
| Patient | Sex | Age (years) | Blood Pressure (mmHg) | SRAD | Comobidities | Cerebral MRI/CT |
|---|---|---|---|---|---|---|
| 1 | F | 61 | 150/100 | Left segmental branch anterior inferior and Right renal artery | Kidney stones | negative |
| 2 | M | 49 | 150/90 | Right renal artery | Severe cardiovascular familiarity, GIST | negative |
| 3 | M | 39 | 140/90 | Left segmental antero-inferior renal artery | Severe cardiovascular familiarity, OFP ostium II | negative |
| 4 | F | 51 | 145/85 | Left renal artery | Dolicocolon | Carotid-oftalmic aneurism |
| 5 | M | 50 | 150/100 | Right and left renal artery | Family history for tumors | negative |
| Patient | Sex | Age (years) | Blood Pressure (mmHg) | SRAD | Comobidities | Cerebral MRI/CT |
|---|---|---|---|---|---|---|
| 1 | F | 61 | 150/100 | Left segmental branch anterior inferior and Right renal artery | Kidney stones | negative |
| 2 | M | 49 | 150/90 | Right renal artery | Severe cardiovascular familiarity, GIST | negative |
| 3 | M | 39 | 140/90 | Left segmental antero-inferior renal artery | Severe cardiovascular familiarity, OFP ostium II | negative |
| 4 | F | 51 | 145/85 | Left renal artery | Dolicocolon | Carotid-oftalmic aneurism |
| 5 | M | 50 | 150/100 | Right and left renal artery | Family history for tumors | negative |
In our experience, SRAD seems to be not very rare in young and healthy patients with minimal comorbidities. Abdomen CTA is one of the “gold standard” non invasive diagnostic method. In patient treated with conservative medical therapy renal outcome is favourable. More studies are necessary to find underlying causes.


{kind=link}
Comments