





Abstract
Renal fibrosis is the strongest prognosis predictor of ESRD in chronic kidney disease (CKD), but non-invasive and repeatable imaging markers are missing. Magnetic resonance imaging (MRI) has wide range of applications in renal parenchymal diseases, and diffusional kurtosis imaging (DKI) is a new promising noninvasive method of MRI which can provide more information about non-Gaussian diffusion using a polynomial model. We had successfully used DKI to assess renal fibrosis in IgA nephropathy in our previous work. This study aimed to evaluate the prognostic value of DKI in CKD.
We prospectively enrolled forty-two CKD patients in our study in Jan. 2017. On recruitment, the basic clinical data were documented, and DKI was performed on a clinical 3T MR scanner. Region-of-interest (ROI) measurements were performed to determine apparent diffusion coefficient (ADC), kurtosis (K) and diffusivity (D) of the cortex of the kidneys. We had followed up these patients for 3 years, and collected all the clinical data and outcomes. The prognostic value of DKI metrics and clinical parameters were investigated.
Forty-two patients consisted of 26 males and 16 females with mean age of 41.3±15.4 years. The most common etiology was IgA nephropathy (25/42, 59.5%). At baseline, the mean value of serum creatinine (SCr) was 224.4±156.2μmol/L. Among them, 18 patients had eGFR≥45ml/min and 24 patients had eGFR<45ml/min. According to the etiology and CKD classification, all the patients had received appropriate treatment. Besides supportive treatment and management of CKD complications, 21 patients (50%) had received corticosteroid and/or immunosuppressants treatment. After 36 months follow up, 12 patients had progressed to end stage renal disease (ESRD), and the mean value of SCr of the remaining 30 patients was 153.0±78.8umol/L. The Kaplan-Meyer survival regression showed that the patients with eGFR<45ml/min had worse clinical outcomes (p=0.0006). ROC analysis and Kaplan-Meyer survival regression showed that DKI metrics (K≥0.66 or ADC<1.35) not only predicted severe renal fibrosis, but also had worse clinical outcomes (p=0.01 and p<0.0001) (Figure 1). According to the COX regression analysis, both K (K≥0.66, HR 4.676, 95%CI 1.262-17.325) and ADC (ADC<1.35, HR 13.118, 95%CI 3.499-49.178) values, but not age, gender and eGFR group (cut-off value: 45ml/min), were the independent risk factors for the progression to ESRD.
Renal ADC and K values obtained from DKI showed significant predictive value for the prognosis of CKD, could be a promising non-invasive technique in patients follow-up.
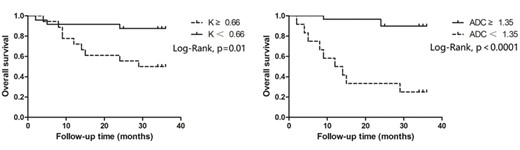
Kaplan-Meyer renal survival curve after 36 months follow-up based on DKI metrics.


{kind=link}
Comments