





Abstract
Cardiovascular disease (CVD) remains the leading cause of morbidity and death in end-stage renal disease (ESRD) patients. Thus, the accumulation of oxalate due to ESRD can increase the risk of CVD. Also, the ability of fecal oxalate-degrading activity (ODA) to reduce plasma oxalate levels has been discussed. On the other hand, despite a key role of atherogenic dyslipidemia in the development of CVD, only a few studies have shown a potential role of microbiota in the regulation of blood lipid profiles in the general population. However, at present, there is a general lack of research on this topic in dialysis patients.
The present study aimed to investigate the association between oxalate-degrading activity (ODA) in fecal microbiota and blood lipid profiles in ESRD patients.
We represented the data of a cross-sectional pilot study examining ODA in fecal microbiota, plasma oxalate concentration (POx) and blood lipid profile markers in 32 ESRD patients. Among the patients, there were 21 hemodialysis (HD) patients and 11 peritoneal dialysis (PD) patients. The average age of the patients was 52.5 [39; 65] years.
The redoximetric titration with KMnO4 was adopted to evaluate total ODA in fecal microbiota. The results were expressed in % oxalate degradation per 0.01 g of feces. The blood lipid spectrum was determined in all patients: total cholesterol level (TC), high (HDL), low (LDL) and very low (VLDL) density cholesterol, triglycerides (TG) and atherogenic index of plasma (AIP).
The median (Me) and interquartile ranges [Q25; Q75] were calculated using the nonparametric Kruskal-Wallis test. The Spearman test was used for the correlation analysis. Chi-square tests were used for comparison of 2 proportions. All statistical analyses were performed using MedCalc.
Dyslipidemia defined as an increase in atherogenic lipoprotein fractions and inhibition of HDL cholesterol was identified in 13/32 (40.6%) ESRD patients. Negative ODA in fecal microbiota (≤ 0 % /0.01 g) was observed in 14/32 (43.7%) patients. Among them, there were 5/21 (23.8%) HD patients and 7/11 (63.6%) PD patients (χ2=3.9, p=0.04).
Significantly lower ODA in fecal microbiota was observed in the patients with atherogenic dyslipidemia in comparison with dyslipidemia-free patients (-5.0 [-8.7; 3.7] vs 3.0 [0.5; 9] %/0.01 g of feces, p=0.02) (Fig. 1). Less ODA in fecal microbiota was, higher levels of TG (r=-0.5, p=0.004) (Fig. 2), VLDL (r=-0.34, p=0.05) (Fig. 3) and, accordingly, AIP (r=-0.38, p=0.03) (Fig. 4) occurred.
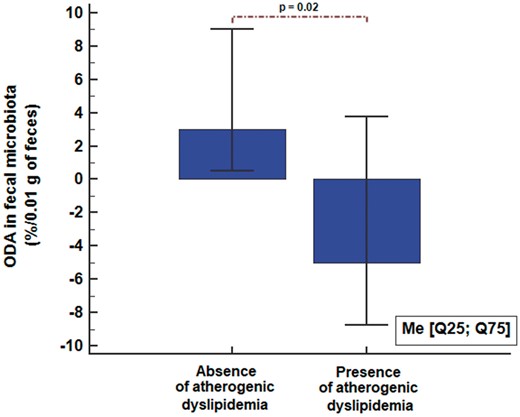
Figure 1: ODA in fecal microbiota in dialysis patients according to atherogenic dyslipidemia status.
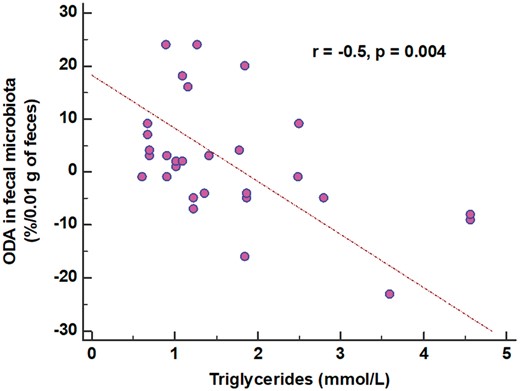
Figure 2: The association between ODA and triglycerides.
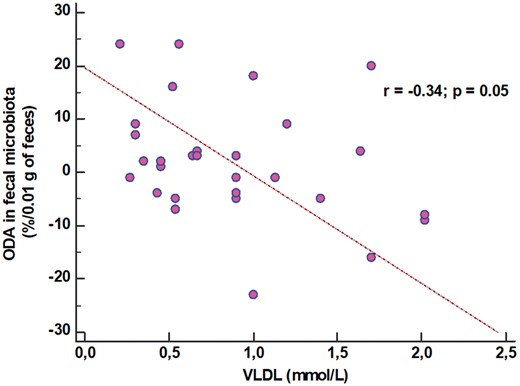
Figure 3: The association between ODA and very-low-density lipoproteins.
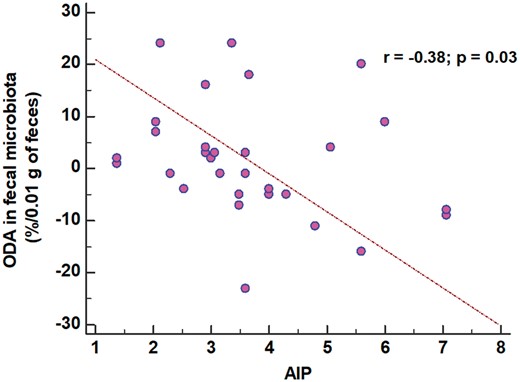
Figure 4: The association between ODA and the atherogenic index of plasma.
The results of our study have provided preliminary evidence on the fact that a decrease in total ODA in fecal microbiota is associated with atherogenic dyslipidemia. Further studies are needed to determine the role of fecal ODA in the formation of dyslipidemia.


{kind=link}
Comments