





INTRODUCTION AND AIMS:Background: Previous studies have shown that the survival of patients with lupus nephritis (LN) who are transplanted with respect to non-diabetic controls have superimposable results.Objective: The aims was to evaluated the survival of lupus patients transplanted in our center, and determine risk factors of mortality and graft loss.
METHODS: Study cohort, case-control (1:2) in patients with CKD secondary LN who received a kidney transplant (n = 32) in the Malaga area (between 1985 and 2010). The controls (n = 64) were matched by age, sex and period of transplant patients. We analyzed graft survival and patient, and risk factors compared with long-term transplant patients without LN.
RESULTS: The analyzed variables between groups were not different, only the most frequent cause of donor death was approached statistical significance: stroke in LN and head injury in controls (p = 0.05). 45% of the population lost the graft, primarily due to chronic kidney disease 53.5%, followed by vascular thrombosis 16.3% (p = 0.57). Censored graft losses occurred 63% in patients transplanted before 2000, whereas this occurred in 20% of which were made from 2000, p <0.000. Censored graft survival was superimposable between groups throughout the follow-up, as well as the survival of patients. About Cox regression, only acute rejection was associated with a twofold increased risk of graft loss.
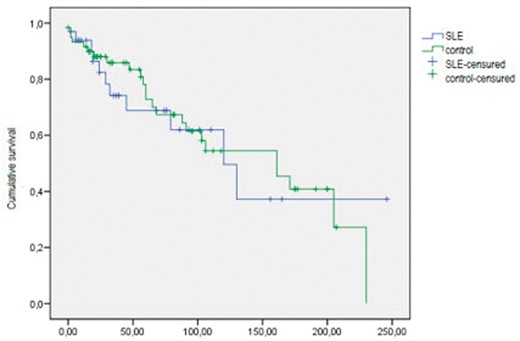
SP765 Figure


{kind=link}
Comments