





INTRODUCTION AND AIMS: Delayed graft function (DGF) continues to pose a significant challenge to the practice of kidney transplantation and has important implications for graft and patient outcomes. Despite advances in transplantation practice, the incidence of DGF has increased, which corresponds to the increasing utilisation of higher risk kidneys from expanded criteria donors (ECD) and donation after circulatory death (DCD). Differences in early graft function between kidney transplant recipients previously managed with either haemodialysis (HD) or peritoneal dialysis are well described. However, only two single-centre studies have compared graft and patient outcomes between extended hour and conventional HD patients, with conflicting results. It is plausible that differences in extravascular fluid volume and haemodynamic parameters could affect allograft function in the early post-transplant period.
METHODS: This retrospective cohort study compared the outcomes of all extended hour (≥24 hours/week) and conventional HD patients transplanted in Australia and New Zealand between 2000 and 2014 and included 4935 patients (378 extended hour HD, 4557 conventional HD). The primary outcome was delayed graft function (DGF), defined as either a spontaneous fall in serum creatinine of less than 10% within 24 hours, or the need for dialysis within 72 hours following transplantation. Secondary outcomes included the requirement for dialysis within 72 hours post-transplant (examined as a binary outcome), acute rejection, estimated glomerular filtration rate at 12 months, death-censored graft failure, all-cause and cardiovascular mortality, and a composite of graft failure and mortality.
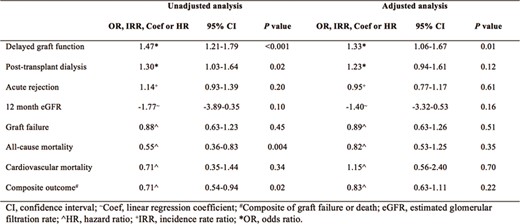
SP631 Figure
CONCLUSIONS: Compared to conventional HD, there was an association between extended hour HD and DGF, although long-term graft and patient outcomes were not different. It is plausible that this association arises due to differences in intravascular volume, haemodynamic parameters, and microcirculatory abnormalities in the early post-transplant period. The physiological benefits of extended hour HD are well described, however when these patients undergo renal transplantation, a potential increase in the risk of DGF may be present.


{kind=link}
Comments