





ABSTRACT
Optimizing training load (TL) and sleep is essential to maximize physical performance and prevent musculoskeletal injuries (MSKIs) for Canadian forces recruits during the 10-week basic military qualification (BMQ) course. The purpose of this study was to assess the TL, sleep duration, the occurrence of MSKIs during the BMQ, and the operation fitness performance during the BMQ.
Forty Canadian recruits, eight females and 32 males, (age 24 ± 5 years; height 176.4 ± 10.4 cm), were monitored with an accelerometer (GENEActiv) on their wrist between weeks 1 and 9 to evaluate the TL and sleep duration. During weeks 2 and 10, the recruits completed an operational fitness evaluation. Injury surveillance was performed over 10 weeks.
TL intensity was significantly different (P = 0.0001) from week to week. The weekly average total time of moderate and vigorous physical activity was 189.7 ± 48.1 min and 44.7 ± 15.2 min, respectively. The average sleep duration was 5.4 ± 0.4 h per night and decreased to 4.2 h ± 0.4 during field exercises. A significant difference in sleep duration was observed between recruits with and without a MSKI. The recruits accumulated a total of 95 days under medical restrictions with an average of 3.8 consecutive days. The VO2peak estimated from the Fitness for Operational Requirements of Canadian Armed Forces Employment job–based simulation test significantly improved from weeks 2 to 10 (pre, 47.1 ± 6.3; post: 50.2 ± 5.8; P = 0.001).
TL is of high magnitude and varies from week to week. The reported mean sleep duration per week may perhaps negatively impact the occurrence of MSKI. No significant improvement was detected in operational fitness by the end of the BMQ.
INTRODUCTION
Members of the Canadian Armed Forces (CAF) are subject to the principle of Universality of Service. This principle states that CAF members are required to perform general military duties, and common defense and security duties, in addition to the tasks required by their specific trade.1 The Basic Military Qualification (BMQ) is a series of mandatory courses taught at the Canadian Force Leaderships and Recruits School (CFLRS) during 10 weeks, which adhere to the CAF principles. Among the general military tasks taught during the BMQ, many are intrinsic physical demands, and recruits are expected to meet a standard by the end of the qualification.
The BMQ is designed to challenge enrolled civilians to develop fundamental skills and knowledge for employment in the CAF. To graduate from the BMQ, all recruits must be able to perform essential tasks such as cardiopulmonary resuscitation, ceremonial exercises, and sentry duties, and it is mandatory to meet the minimum standard of the Fitness for Operational Requirements of Canadian Armed Forces Employment (FORCE) job–based simulation test (JBST). The purpose of the FORCE JBST is to predict the ability of future CAF members to perform physically challenging tasks that are deemed essential for CAF personnel. It has been previously reported that a low initial fitness level is a predictor of musculoskeletal injuries (MSKIs) at CFLRS,2 and therefore, it is essential for recruits to be well prepared. Every CAF recruit follows the same physical training (PT) program that prepares them to pass the FORCE JBST and the rigors of military occupational training, regardless of their trade, age, gender, and initial fitness level.
During the BMQ, the perceived training load (TL) within the same recruit platoon can be slightly different due, among other things, to the different initial fitness level, sex, and body composition of the recruits. The physical and mental requirement can be very high at the beginning of the qualification, and the tasks are often performed with an external load, such as a weapon and/or a rucksack (up to 24.5 kg) to carry. It is well documented that the addition of external loads increases the metabolic demand3 as well as the possibility of increasing the risk of injury.4 Between the years of 2016 and 2017, course interruption from the injury rate was reported at 4.3% at CFLRS during the BMQ.2 The majority of these course-interruption injuries were from overuse (56%) and mostly targeted the lower limbs (78%).2 A better understanding of TL would allow military instructors to plan a better load progression of certain tasks, such as rucksack marches, and therefore establish an appropriate acute to chronic workload ratio to avoid big spike of TL, to maintain a minimum of TL, to indicate the need for recovery, and therefore to reduce the injury risk. As a comparison, in elite sports, TL and performance monitoring are well recognized to successfully program TL in order to minimize injury and increase performance.5 Despite this well-documented effectiveness with sports athletes, monitoring TL in a military environment with recruits, who are considered as tactical athletes, seems more difficult and few investigators, to this date, have studied it during basic military training.6–8
The quantification of the TL during the BMQ is of fundamental importance to establish an adequate periodization of the TL. Thus, the objective of this observational study was to evaluate, for the first time, how the TL fluctuates on a weekly basis during a 10-week BMQ. A secondary objective was to identify how the training plan periodization impacts the operation fitness performance, the sleep duration, and risk of developing injuries during a 10-week BMQ. We hypothesized that TL would fluctuate significantly on a weekly basis.
MATERIALS AND METHODS
Ethics
This observational study was approved by the Defense Research and Development Canada Human Research Ethics Committee (DRDC-HREC#2021-017), by the Director General of Health Services (DGHS), and by the Director General of Military (DGM). On their first day at CFLRS, the recruits attended the study information session led by the research team members. Their participation was voluntary, and their participation had no influence on the outcome of completion of their course. The recruits had time to ask questions and fully understand their implications before signing the informed consent form.
Participants
Forty participants (32 males and 8 females) out of fifty-four from A-11 platoon at CFLRS provided their informed consent to participate in this research and completed a demographic information questionnaire. The mean age and height were 24.6 ± 5.2 years and 176.4 ± 10.4 cm, respectively (24.6 ± 5.2 years and 164.8 ± 8.4 cm for females; 23.2 ± 5.1 years and 179.3 ± 8.8 cm for males). During the project, eight participants were withdrawn from the study for different reasons such as MSKI (N = 4), voluntary release from the military (N = 3), and quitting the study (N = 1), which represents a 20% loss. The participants received the standard curriculum of the 10-week BMQ, which was composed of military skills (drill, obstacle course, and field exercises), PT, and theoretical classes. The platoon was sleeping on the eighth dormitory floor in a building of 11 floors, which represented close to 275 steps to climb from the ground floor. The smoking status was 12 (30%) ex-smokers, 10 (25%) current smokers, 16 (40%) never smoked, and 2 (5%) missing data.
Pilot Descriptive Study Design
The study was completed during the autumn season in the province of Québec (Canada) and between the temperature range 0 and 23 degree Celsius, and the wind fluctuated between 11 and 57 km h−1, according to the local weather station.9
Physical activity and sleep duration were measured using accelerometers (GENEActiv Originals, UK). Physical activity and sleep duration were collected daily during weeks one to nine. Participants wore the accelerometer on the dominant or non-dominant wrist to minimize burden and maximize wear compliance. Raw acceleration sampling was set at 40 Hz and extracted every 60 s. The gravity-subtracted sum of vector magnitudes for each minute were analyzed from the raw acceleration data to estimate metabolic equivalents (METs) using the lowest thresholds10 previously validated for GENEActiv accelerometers11 and calculated using the following equation:
The quantity/duration of physical activity (PA) and sleep was the weekly average between Monday and Sunday. Sleep data were programmed from 2300 to 0500. Data were extracted from the devices every two weeks by the research team.
The Musculoskeletal injuries monitoring fact form was completed following every visit to the medical clinic. The participants filled out a MSKI questionnaire and provided a copy of their medical limitations to the investigators.
The FORCE-JBST was administered as indicated in the standard protocol of the FORCE Operations Manual.12 The FORCE-JBST consists of four following components: 20 meter rushes (20mR); the sandbag lift (SBL), the intermittent loaded shuttle (ILS), and the sandbag drag (SBD), which together represent a proxy agility, lower and upper body power and strength, anaerobic and aerobic capacity, and overall stamina/endurance.2 The distance covered for 20 mR is 80 m in 51 s or less, the weight for the SBL is 20 kg and needed to be lifted 30 times in 3 min 30 se or less, the distance covered for the ILS is 400 m divided 5 times of 40-m walking with a sandbag of 20 kg and 40-m running without load in 5 min 21 sec or less, and finally, for the SBD, you need to carry a 20-kg sandbag and pull a minimum of four on the floor over 20 m without stopping (the total of weight being dragged depends on the type of floor). Maximal aerobic capacity (VO2peak) was estimated from the FORCE-JBST, which combines performance on the test and waist circumference.13 Operational physical fitness is scored on a total of 400 points (z/400 score), which is defined by the completion time of each of the four components (100 points/components) of the FORCE-JBST according to sex and age categories. This total score is compared to the overall CAF population. FORCE-JBST was administered during the second and the last weeks of the BMQ.
Height was obtained using a stadiometer to the nearest 0.5 cm. Measurements were collected during the first week of the BMQ.
Statistical Analysis
The raw acceleration data from the accelerometer were processed and analyzed using an open-source package (GGIR Version 2.5-0) in R, expressed in milligravitational units per second2 (mg s−2), and were completed in a numeric spreadsheet (Excel, Office 2018, Microsoft, USA). The missing data attributed to the mean values of the group studied. Attributing the mean value for missing data was done when breakage or not wearing the device on a particular day occurred. Participants with more than 15% of missing data were excluded (six participants) from the research only for the TL and sleep duration analysis, and an average of 1.8 days per participants was substituted. The mean ± standard deviation of TL, sleep, FORCE-JBST, and MSKI were calculated using SPSS 27 version (IBM, USA).
Paired sample t-tests were used to evaluate the changes in FORCE-JBST from the first and last weeks of BMQ. Repeated measures analysis of variance (ANOVA) were used to compare the sleep duration variation between recruits with and without MSKI throughout the BMQ, and unpaired sample t-tests were used to evaluate the mean difference between groups. Pearson’s correlation was used to evaluate the relationship with the TL and MSKI. Finally, a hierarchical cluster analysis was conducted to classify the population studied. The level of significance was established with alpha at P ≤ 0.05. All statistical analyses were performed using SPSS 27 version (IBM, USA).
RESULTS
TL
The average overall TL during 9 weeks of the BMQ was 2767.4 ± 148.7 METs min per day. The weekly TL varied significantly from week to week (F(1,23) = 6.071; P = 0.022) (Fig. 1A). Most noteworthily, the highest TL was 2970.3 ± 283.5 METs min at week 8 and was significantly different from all other training weeks. In fact, weeks 1 and 4 (2896.4 ± 244.4 METs min and 2922.2 ± 230.7 METs min respectively) were similar and significantly different from other training weeks. Weeks 5, 6, and 9 (2789.4 ± 205.4 METs min, 2789.3 ±302.4 METs min, and 2792.9 ± 367.1 METs min, respectively) were similar and significantly different from other training weeks. The lowest TL was observed during weeks 2, 3, and 7 (2652.0 ± 265.8 METs min, 2566.6 ± 266.9 METs min, and 2567.2 ± 223.8 METs min, respectively) and were significantly different from other training weeks. The average total time of moderate to vigorous physical activity (MVPA) per week during the BMQ is 1640.9 ± 342.8 min with an average of 189.7 ± 48.1 min of moderate PA and 44.7 ± 15.2 min of vigorous PA per day (Fig. 1B).
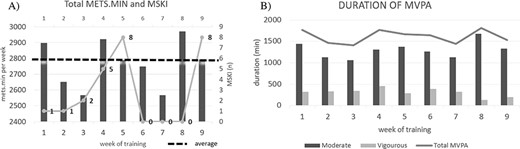
Summary of TL over 9-week BMQ. (A) Average total METs min per day and number of MSKI per week during 9 weeks. The total METs min is represented by the bar graph, the average is represented by the dark dotted line and the number of MSKI is represented by the grey light line. (B) Average duration of MVPA per week during 9 weeks. Moderate and vigorous PA is represented by the dark and light bar graphs, respectively, and the average total of MVPA is represented by the line.
MSKI Occurrence
Sixteen participants needed to consult the medical clinic for MSKI for a total of 25 consultations as seen in Fig. 1A (light grey line). Fifty-two percent of consultations occurred during weeks four and five. Pearson’s analysis did not show a significant correlation between TL and MSKI per week (r = 0.30 and P = 0.440), but the relationship was in the anticipated direction. Altogether, the participants accumulated 95 days under medical limitations with an average of 3.8 consecutive days per consultation. The majority of the MSKI area was at the lower limb (79%), mainly caused by activities with repeated motion (62.5%), whereas only 20.8% of those injuries were traumatic. From the hierarchical cluster analysis, the characteristic that describes this sample of recruits with low and high risk of MSKI are shown in Fig. 2.
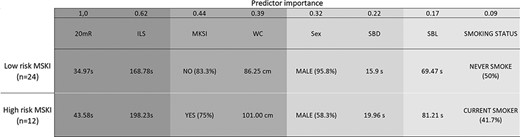
Population classification with predictor importance from 1.0 to 0.009. 20 meter rushes. MSKI = recruits with musculoskeletal injury during BMQ.
FORCE-JBST Performance
The FORCE-JBST results from the second and last week of BMQ are provided in Table I. The results present the performance on the FORCE-JBST for all recruits, female recruits and male recruits. The recruits when compared to week 2 significantly reduced their waist circumference (P = 0.0001) at week 10 by 4.8 cm on average. When focusing on both the entire sample, and males only, most of the FORCE-JBST components were significantly improved (P ≤ 0.05). However, as observed on the score z/400, the overall operational fitness performance did not significantly improve from pre to post. For female recruits, only the waist circumference showed a significant improvement (P = 0.028), and surprisingly, even if not significant, the z/400 score decreased.
FORCE-JBST Results. Overall Results Include Females and Males
| Overall | Female | Male | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean ± standard deviation (SD) | Mean ± SD | Mean ± SD | |||||||||||
| N | Pre | Post | P | N | Pre | Post | P | N | Pre | Post | P | ||
| FORCE-JBST | Waist circumference (cm) | 29 | 89.6 ± 10.7 | 84.8 ± 7.6 | 0.000 | 6 | 89.2 ± 5.1 | 83.0 ± 4.9 | 0.028 | 23 | 89.7 ± 11.8 | 85.3 ± 8.2 | 0.004 |
| 20-m rushes (s) | 28 | 36.7 ± 4.8 | 37.6 ± 5.7 | 0.154 | 5 | 43.4 ± 6.6 | 42.9 ± 8.5 | 0.732 | 23 | 35.2 ± 36.5 | 36.5 ± 4.4 | 0.085 | |
| Sandbag lift (s) | 28 | 70.4 ± 16.0 | 65.9 ± 16.9 | 0.006 | 5 | 88.9 ± 19.4 | 88.5 ± 25.6 | 0.956 | 23 | 66.4 ± 12.3 | 61.0 ± 9.4 | 0.001 | |
| Intermittent loaded shuttles (s) | 27 | 172.8 ± 21.0 | 159.9 ± 22.1 | 0.002 | 4 | 197.0 ± 25.0 | 185.3 ± 22.3 | 0.173 | 23 | 168.6 ± 17.7 | 155.5 ± 19.3 | 0.006 | |
| Sandbag drag (s) | 27 | 16.9 ± 5.6 | 15.2 ± 4.9 | 0.026 | 4 | 24.7 ± 7.4 | 20.3 ± 3.8 | 0.309 | 23 | 15.6 ± 4.1 | 14.3 ± 4.5 | 0.048 | |
| Estimated VO2peak (ml kg−1 min−1) | 24 | 47.1 ± 6.3 | 50.2 ± 5.8 | 0.001 | 4 | 38.9 ± 6.3 | 43.2 ± 5.3 | 0.118 | 20 | 48.7 ± 4.9 | 51.6 ± 4.9 | 0.003 | |
| Score z/400 | 26 | 247.5 ± 77.4 | 259.3 ± 97.1 | 0.335 | 4 | 232.3 ± 143.1 | 218.8 ± 192.2 | 0.693 | 22 | 250.2 ± 64.4 | 266.7 ± 74.7 | 0.225 | |
| Overall | Female | Male | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean ± standard deviation (SD) | Mean ± SD | Mean ± SD | |||||||||||
| N | Pre | Post | P | N | Pre | Post | P | N | Pre | Post | P | ||
| FORCE-JBST | Waist circumference (cm) | 29 | 89.6 ± 10.7 | 84.8 ± 7.6 | 0.000 | 6 | 89.2 ± 5.1 | 83.0 ± 4.9 | 0.028 | 23 | 89.7 ± 11.8 | 85.3 ± 8.2 | 0.004 |
| 20-m rushes (s) | 28 | 36.7 ± 4.8 | 37.6 ± 5.7 | 0.154 | 5 | 43.4 ± 6.6 | 42.9 ± 8.5 | 0.732 | 23 | 35.2 ± 36.5 | 36.5 ± 4.4 | 0.085 | |
| Sandbag lift (s) | 28 | 70.4 ± 16.0 | 65.9 ± 16.9 | 0.006 | 5 | 88.9 ± 19.4 | 88.5 ± 25.6 | 0.956 | 23 | 66.4 ± 12.3 | 61.0 ± 9.4 | 0.001 | |
| Intermittent loaded shuttles (s) | 27 | 172.8 ± 21.0 | 159.9 ± 22.1 | 0.002 | 4 | 197.0 ± 25.0 | 185.3 ± 22.3 | 0.173 | 23 | 168.6 ± 17.7 | 155.5 ± 19.3 | 0.006 | |
| Sandbag drag (s) | 27 | 16.9 ± 5.6 | 15.2 ± 4.9 | 0.026 | 4 | 24.7 ± 7.4 | 20.3 ± 3.8 | 0.309 | 23 | 15.6 ± 4.1 | 14.3 ± 4.5 | 0.048 | |
| Estimated VO2peak (ml kg−1 min−1) | 24 | 47.1 ± 6.3 | 50.2 ± 5.8 | 0.001 | 4 | 38.9 ± 6.3 | 43.2 ± 5.3 | 0.118 | 20 | 48.7 ± 4.9 | 51.6 ± 4.9 | 0.003 | |
| Score z/400 | 26 | 247.5 ± 77.4 | 259.3 ± 97.1 | 0.335 | 4 | 232.3 ± 143.1 | 218.8 ± 192.2 | 0.693 | 22 | 250.2 ± 64.4 | 266.7 ± 74.7 | 0.225 | |
FORCE-JBST Results. Overall Results Include Females and Males
| Overall | Female | Male | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean ± standard deviation (SD) | Mean ± SD | Mean ± SD | |||||||||||
| N | Pre | Post | P | N | Pre | Post | P | N | Pre | Post | P | ||
| FORCE-JBST | Waist circumference (cm) | 29 | 89.6 ± 10.7 | 84.8 ± 7.6 | 0.000 | 6 | 89.2 ± 5.1 | 83.0 ± 4.9 | 0.028 | 23 | 89.7 ± 11.8 | 85.3 ± 8.2 | 0.004 |
| 20-m rushes (s) | 28 | 36.7 ± 4.8 | 37.6 ± 5.7 | 0.154 | 5 | 43.4 ± 6.6 | 42.9 ± 8.5 | 0.732 | 23 | 35.2 ± 36.5 | 36.5 ± 4.4 | 0.085 | |
| Sandbag lift (s) | 28 | 70.4 ± 16.0 | 65.9 ± 16.9 | 0.006 | 5 | 88.9 ± 19.4 | 88.5 ± 25.6 | 0.956 | 23 | 66.4 ± 12.3 | 61.0 ± 9.4 | 0.001 | |
| Intermittent loaded shuttles (s) | 27 | 172.8 ± 21.0 | 159.9 ± 22.1 | 0.002 | 4 | 197.0 ± 25.0 | 185.3 ± 22.3 | 0.173 | 23 | 168.6 ± 17.7 | 155.5 ± 19.3 | 0.006 | |
| Sandbag drag (s) | 27 | 16.9 ± 5.6 | 15.2 ± 4.9 | 0.026 | 4 | 24.7 ± 7.4 | 20.3 ± 3.8 | 0.309 | 23 | 15.6 ± 4.1 | 14.3 ± 4.5 | 0.048 | |
| Estimated VO2peak (ml kg−1 min−1) | 24 | 47.1 ± 6.3 | 50.2 ± 5.8 | 0.001 | 4 | 38.9 ± 6.3 | 43.2 ± 5.3 | 0.118 | 20 | 48.7 ± 4.9 | 51.6 ± 4.9 | 0.003 | |
| Score z/400 | 26 | 247.5 ± 77.4 | 259.3 ± 97.1 | 0.335 | 4 | 232.3 ± 143.1 | 218.8 ± 192.2 | 0.693 | 22 | 250.2 ± 64.4 | 266.7 ± 74.7 | 0.225 | |
| Overall | Female | Male | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean ± standard deviation (SD) | Mean ± SD | Mean ± SD | |||||||||||
| N | Pre | Post | P | N | Pre | Post | P | N | Pre | Post | P | ||
| FORCE-JBST | Waist circumference (cm) | 29 | 89.6 ± 10.7 | 84.8 ± 7.6 | 0.000 | 6 | 89.2 ± 5.1 | 83.0 ± 4.9 | 0.028 | 23 | 89.7 ± 11.8 | 85.3 ± 8.2 | 0.004 |
| 20-m rushes (s) | 28 | 36.7 ± 4.8 | 37.6 ± 5.7 | 0.154 | 5 | 43.4 ± 6.6 | 42.9 ± 8.5 | 0.732 | 23 | 35.2 ± 36.5 | 36.5 ± 4.4 | 0.085 | |
| Sandbag lift (s) | 28 | 70.4 ± 16.0 | 65.9 ± 16.9 | 0.006 | 5 | 88.9 ± 19.4 | 88.5 ± 25.6 | 0.956 | 23 | 66.4 ± 12.3 | 61.0 ± 9.4 | 0.001 | |
| Intermittent loaded shuttles (s) | 27 | 172.8 ± 21.0 | 159.9 ± 22.1 | 0.002 | 4 | 197.0 ± 25.0 | 185.3 ± 22.3 | 0.173 | 23 | 168.6 ± 17.7 | 155.5 ± 19.3 | 0.006 | |
| Sandbag drag (s) | 27 | 16.9 ± 5.6 | 15.2 ± 4.9 | 0.026 | 4 | 24.7 ± 7.4 | 20.3 ± 3.8 | 0.309 | 23 | 15.6 ± 4.1 | 14.3 ± 4.5 | 0.048 | |
| Estimated VO2peak (ml kg−1 min−1) | 24 | 47.1 ± 6.3 | 50.2 ± 5.8 | 0.001 | 4 | 38.9 ± 6.3 | 43.2 ± 5.3 | 0.118 | 20 | 48.7 ± 4.9 | 51.6 ± 4.9 | 0.003 | |
| Score z/400 | 26 | 247.5 ± 77.4 | 259.3 ± 97.1 | 0.335 | 4 | 232.3 ± 143.1 | 218.8 ± 192.2 | 0.693 | 22 | 250.2 ± 64.4 | 266.7 ± 74.7 | 0.225 | |
Sleep Duration
The average sleep duration was 5.4 ± 0.4 h per night, while during field exercises, during week 8 and two days in week 9, it decreased to an average of 4.2 h ± 0.4 per night (Fig. 3). A significant difference in sleep duration was observed between recruits with and without MSKI throughout the BMQ (F(1, 22) = 6.608; P = 0.017). The group with MSKI slept 54 min ± 11 min (95% confidence interval (CI): −80 min to −36 min) on average less than the group without MSKI (P = 0.000).
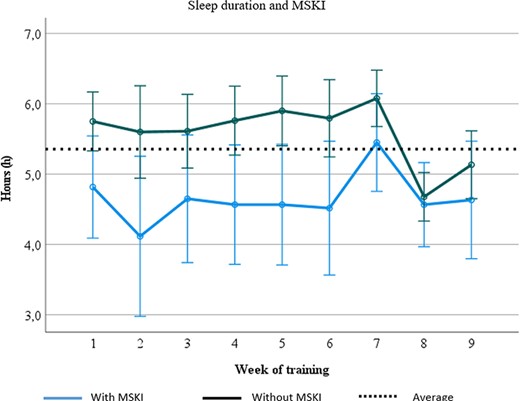
Comparison of sleep duration (h) for recruits with and without MSKI. The average sleep duration for recruits with MSKI is represented by the dark line, the average sleep duration for recruits without MSKI is represented by the light line, and the overall average sleep duration throughout the 9-week BMQ is represented by the dotted line.
DISCUSSION
To our knowledge, this is the first observational study that investigates the TL, sleep duration, MSKI occurrence, and operational fitness performance without disturbing the normal curriculum during the 10-week BMQ. From the TL analysis, one can observe that the physical demands are of high magnitude with high demands from the onset at week 1 and that TL varies significantly from week to week. These variations can be explained by the different objectives of instructions per week. For example, the end of indoctrination is at the beginning of week 4 and recruits are required to meet the military standard, and field exercises are held in week 8 and recruits are required among other things to apply field techniques in a tactical environment. Indeed, the average total time of MVPA per week during the BMQ is as high as 1640.9 ± 342.8 min. On a daily basis, the average PA was observed at 189.7 ± 48.1 and 44.7 ± 15.2 min of moderate and vigorous, respectively. These physical demands seem to be higher than the ones reported from basic military training in Fort Benning (Georgia, USA) with a daily average of 107 ± 42 min at moderate intensity, 26 ± 22 min in vigorous intensity and 10 ± 21 min in very vigorous intensity.8 Data acquisition was similar in both studies, but some differences may explain the higher TL during BMQ at CFLRS compared to basic military training at Fort Benning: accelerometer location (wrist vs waist), raw acceleration data (40 Hz vs 30 Hz), and information entered into the software (none vs age, height, weight, ethnicity, and hand dominance). When compared to the Canadian Society for Exercise Physiology recommendations for PA that are to accumulate 150 minutes of MVPA per week,14 the total MVPA per week during BMQ was observed to be 10.9 times higher. The gap can be even higher as only 15% of Canadians aged from 20 to 79 years old meet this recommendation, while 69% of Canadians engage in sedentary behavior during the day.15 As recruits are a reflection of the Canadian general population, the drastic increase in TL between civilian life and the first weeks of qualification put stress on the musculoskeletal system, particularly the lower limbs, and has been associated with an increased risk of developing MSKI.16,17 The relationship between TL and MSKI is well documented in sport18 and it was reported that the risk of injury can be up to 3 to 4 weeks after an increase of TL.19 Similar results were observed in this study, which follows the drastic increase from civilian life at weeks 1, 4 and 8. In addition, we observed that 80% of injuries are to the lower body (65% overuse and 25% traumatic) as reported by others.2 When we compare our data from the BMQ to the British Army recruit’s infantry training, it was observed that 81% of injuries were also to the lower body with 65% of those injuries being attributed to overuse.20 The same comparison is observed when compared to the New Zealand Army Recruits, where an investigation showed 75% of lower body injuries, of which 67% were at the knee and below.21
TL monitoring allows us to identify some modifiable principles in training management in order to prevent injuries and optimize performance. In fact, it is recommended to avoid sudden changes in the TL on a weekly and daily basis to ensure that the load does not exceed the capacity of the individual as well as to maintain a minimum of PA on a daily basis in order to develop the ability to tolerate the demands in sports as well as in a military context.22,23 Adequate physical preparation for such conditions promotes the ability to tolerate a rapid increase in workload at a high volume and thus reduce the risk of injury.24
Physical training preparation for the BMQ is necessary since it was previously reported that recruits with a lower FORCE-JBST score (20mR (46s), SBL (97.5s), ILS (218.0s) and SBD (fail)) are more likely to develop an MSKI at CFLRS.2 In this study, we observed that recruits at greater risk of MSKI have faster results on FORCE-JBST than those previously reported by Chassé et al. (2020) but slower results when compared to the recruits without MSKI. Also, we observed that the BMQ has a positive impact on operational fitness performance for all recruits and men only on most of the FORCE-JBST components after BMQ except for the 20mR and therefore the score z/400. Overall, the lack of improvement (score z/400) on operational fitness performance is mainly due to a deterioration of the 20mR (agility and speed component), which may be explained by the timing (week 10) of the second FORCE-JBST evaluation completed following the field exercises thus in a more fatigued state. However, with regard to female recruits’ operational fitness performance compared to the male recruits, the lack of improvement may be caused by inadequate high-intensity endurance training or strength training, and/or a lack of progression in the training plan.25 Therefore, it seems important to understand that the physical demand for BMQ may not provide adequate training stimulation to induce changes in operational fitness performance in women, that the FORCE-JBST should be considered when developing injury prevention strategies,26 and that the minimum standard of FORCE-JBST may not meet the physical requirements of the BMQ.27
Sleep deprivation has a negative impact on physical and mental performance.28,29 Current guidelines for bedtime and rise time at the CFLRS are from 2200 to 0600 to provide the opportunity for 8 h of sleep per night. Nevertheless, our data demonstrated that recruits sleep on average only 5.4 hours during the BMQ and an average 4.4 h during field exercises, which is lower than current guidelines. Reduction of sleep quantity during field exercises may be due to nocturnal activities as well as the outdoor sleep environment. These average sleep durations during field exercises seem to be higher than the one reported from the British officer cadets with an average of 2.1 (1.3 h) h of sleep per night.30 However, a recent study from the 12-week basic military training in Australia reported that recruits sleep an average of 6.3 h per night and that it was possible to maintain the same sleep quantity during field exercises.31 Allowing adequate sleep time has positive impacts on performance by maintaining alertness, perceptual and cognitive abilities.32 Indeed, these psychological factors have impacts on physical performance33 and it was previously reported that less than 8 h of sleep per night can be associated with increased risk of suffering a MSKI.34 Lisman et al.35 also reported a significant association between sleep quantity and the risk of suffering a MSKI. We observed that recruits with MSKI throughout the BMQ had slept less (P < 0.05), but currently it is impossible to say whether the pain disrupted sleep or that it was sleep disturbances that increased pain/MSKI. Thus, the use of scientific principles for TL and sleep monitoring management can help assess fatigue and indicate the need for recovery to promote performance while minimizing the risk of injury.36
LIMITATIONS
This observational study is a first step at quantifying and qualifying the TL of the BMQ in Canada. The results from this study represent a single platoon (N = 40) who slept on the eighth floor during the autumn season, with only six females completing the 10-week BMQ and limited variety of military trades. The variables studied (TL, MSKI, sleep, and operational fitness performance) may vary differently depending of several factors including the dormitory floor (e.g., 6th or 11th), the different seasons (winter vs summer) and the different personality or attitude of military instructors. Another limitation of this study was that the accelerometer was worn on the wrist, which may overestimate movements when recruits walk quickly from one place to another with accentuated arm movements. On the other hand, TL may be underestimated when carrying loads, muscle exercises, or prolonged standing. Finally, we demonstrated the feasibility of monitoring TL and it would be beneficial to replicate this study with a larger population as well as with officer cadets.
CONCLUSION
In conclusion, TL is of high magnitude and demonstrates a high variability from week to week during the BMQ and seems to be linked to MSKI occurrences during BMQ at CFLRS. Furthermore, low sleep duration seems to be associated with the occurrence of MSKI. According to the FORCE-JBST assessment, we did not observe a significant improvement in operational fitness performance by the end of BMQ. Nonetheless, recommendations, following the results of our study, for military PT to optimally prepare new recruits for the physical demands of the BMQ would include the following: (1) better prepare new recruits before their arrival or evaluate the possibility to modify the FORCE-JBST to increase the level of fitness at the beginning, (2) better periodize the training plan to minimize the week-to-week variation, (3) investigate how disrupted sleep influences MSKI and vice versa and whether improving sleep duration has any subsequent impact on injury rate at CFLRS, and (4) focus on the difference in operational fitness performances between the sexes. Overall, to maximize the recruits’ operational fitness performances and reduce the general occurrence of MSKI, scientifically based TL monitoring and MSKI surveillance must be a priority at all levels.
ACKNOWLEDGMENTS
The authors would like to thank the CFLRS school commander, Lcol Ramessar, the DGHS, and the DGM Personnel for supporting this research project.
The authors would like to express their special thanks to Pierre-Luc Desormeaux, Mona Raouf, Patrick Gagnon, Julie Gagnon, Philippe Laplante, Maxime Brouillard, Maj Julien Galarneau, and Raymond Houle.
FUNDING
This work is writting by the CFMWS employees supporting the Canadian Armed Force.
CONFLICT OF INTEREST STATEMENT
None declared.
INSTITUTIONAL REVIEW BOARD (HUMAN SUBJECTS)
This observational study was approved by the DRDC-HREC (#2021-017), by the DGHS, and by the DGM.
INSTITUTIONAL ANIMAL CARE AND USE COMMITTEE (IACUC)
Not applicable.
INDIVIDUAL AUTHOR CONTRIBUTION STATEMENT
A.L.S. collected and analyzed the data and drafted the original manuscript. A.A.G. and J.A.B. designed this research, reviewed, and edited the manuscript. All authors read and approved the final manuscript.
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are available on request from the corresponding author. All data is freely accessible.
INSTITUTIONAL CLEARANCE
Institutional clearance approved.
REFERENCES
Author notes
The views expressed are solely those of the authors and do not reflect the official policy or position of the Canada Armed Forces, the Department of National Defense, or the Government of Canada.


{kind=link}
{kind=link}
{kind=link}