





Case report
A 57-year-old, previously healthy, Spanish man presented in February 2021 with a one-week history of right upper quadrant (RUQ) abdominal pain and fever. On examination, main findings were a blood pressure of 90/50 mmHg, a heart rate of 105 bpm, a temperature of 37.6°C, jaundice and abdominal pain (RUQ). He referred no significant past medical history and had never traveled outside Europe. On secondary direct questioning during hospitalization, he admitted to previous unprotected contact (including oral-anal sex) with a Brazilian female sex worker.
Blood tests revealed an elevated white blood cell count (16 400 cells/ul with 14 700 neutrophils/ul), elevated C-Reactive protein (206 mg/l, normal range 0–5), procalcitonin levels of 18.23 ng/ml (normal range < 0.25 ng/ml), elevated AST, ALT, GGT, alkaline phosphatase and LDH levels (205, 227, 157, 263 and 838 U/l, respectively) with a total Bilirubin of 4.35 mg/dl (HIV, hepatitis B and C and syphilis serology were all negative).
A CT scan revealed a large abscess of the hepatic dome (13 × 14.4 × 10 cm) (see Figure 1). Due to hemodynamic instability, urgent percutaneous pigtail catheter insertion was performed and purulent fluid was drained. Empyrical treatment with ceftriaxone and metronidazole was initiated.
Culture of the abscess was sterile (16S pan-bacterial universal PCR also negative) but Entamoeba histolytica PCR of the fluid was positive (in house real-time PCR targeting Entamoeba SSU rRNA gene). Serum E. histolytica IgG was positive (NovaLisa® Entamoeba histolytica IgG, Nova Tec Immundiagnostica GmbH, Dietzenbach, Germany). Stool examination was negative for parasites (rapid antigen test for Entamoeba spp. negative). A colonoscopy revealed scattered colonic ulceration (non-specific inflammatory findings on histological examination, negative PCR for E. histolytica).
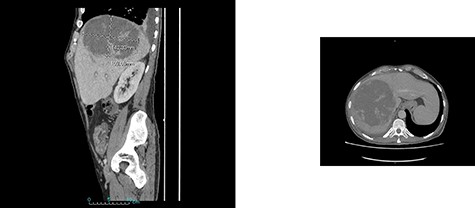
CT scan showing hepatic dome amebic liver abscess (10 × 14 cm).
Outcome was favorable with full-dose intravenous metronidazole treatment which was followed by oral paromomycin to eliminate intraluminal amebic cysts. Evaluation and screening of the presumed contact was attempted but was not possible.
Discussion
Imported infections have decreased during the current pandemic but ‘tropical infections’ may be still be diagnosed in non-endemic areas despite travel restrictions.1 Sexual transmission of intestinal pathogens (such as E. histolytica) or commensals through the oral-anal route has been well documented previously and although most reports describe cases in men who have sex with men, transmission through heterosexual contact as described in this report is also possible.2,3 A recent study on the impact of travel restrictions and lockdown on notifiable infectious diseases in a European country showed sexually transmitted infections continued to occur despite lockdown measures.1 Healthcare professionals in non-endemic settings should be aware of possible alternate modes of transmission and the potential complications of amebic infections.
Author contributions
All authors contributed to the clinical management of the patient and interpretation of the data. F.B. and F.F.N. wrote the paper.
Funding
Support was provided by the Instituto de Salud Carlos III project ‘RD16/0027/0020’ Red de Enfermedades Tropicales, Subprograma RETICS del Plan Estatal de I +D +I.
Conflict of interest: There are no conflicts of interest to declare.

{kind=link}