





As a low-middle income and populous country with 95 million people, Vietnam faces a high risk of a severe COVID-19 outbreak, which has overflowed even the most developed health care systems.1,2 Despite limited resources, Vietnam has kept the outbreak under control since the first cases were confirmed more than 2 months ago.
Recognizing the outbreak
COVID-19 officially hit Vietnam on 23 January, and the ongoing outbreak in Vietnam can be temporarily divided into three phases (Figure 1, top panel). The first phase lasted until 5 March, characterized by case importation from Asian countries. As COVID-19 exploded globally, Vietnam entered Phase 2 with cases also imported from western countries. On 23 March, the first case without an epidemiological link was reported, suggesting the presence of community spread (Phase 3).
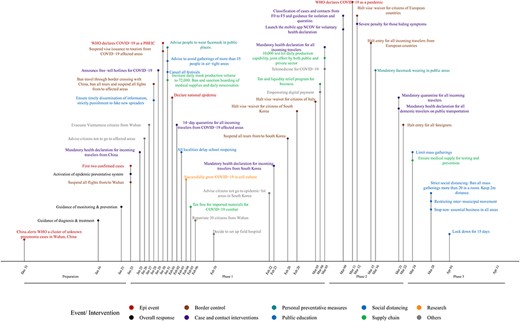
Timeline of outbreak responses in Vietnam
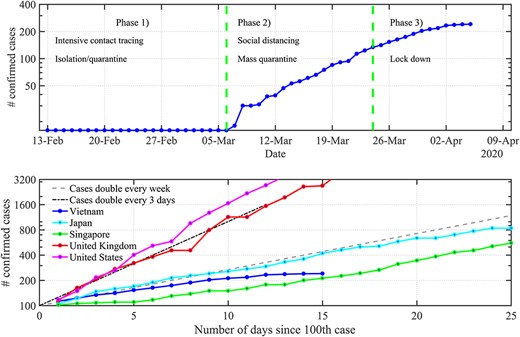
The cumulative number of confirmed cases (top, three phases of the outbreak; bottom, Vietnam in comparison with other countries since 100 cases were reported)
Responses
Vietnam’s responses are generally in line with current practices of other countries, but they were implemented very early, with great emphasis on case identification, source control and public awareness. As early as 16 January 2020, the Vietnamese government took pre-emptive actions by issuing guidelines of COVID-19 diagnosis, treatment and prevention.3 Of note, monitoring and response plans were outlined for potential scenarios. For each phase of the outbreak, specific interventions were issued and adapted accordingly. Overall, control measures were increased in intensity over time, shifting from voluntary to mandatory and from epicentre-targeted to widely targeted (see Figure 1 for details).
To minimize case importation, Vietnam deployed border control measures such as temperature screening, visa waiver/entry halting, 14-day quarantine enforcement and mandatory health declaration. Health declaration, then, was extended to residents with the launch of mobile app NCOV. Extended contact tracing was conducted—once a case (F0) was identified, contacts were traced up to five generations (F1–F5) and put under different levels of prevention.4
The government has kept the public constantly updated with the outbreak progression and responses via accessible official channels, in which personal protective measures and social distancing were especially highlighted. Together with ensuring the supply of daily necessities, the production of medical essentials and personal protective equipment (PPE) was hastened since the first phase of the outbreak, with 10 000 test kits and 72 000 facemasks produced daily.4 Therefore, social distancing, mass masking and other control measures have been embraced and complied by Vietnamese citizens.
Interim outcomes and lessons learned
As of 7 April, Vietnam recorded 241 confirmed cases and no fatality.4 The country has kept the outbreak at a slow growth rate even after reporting 100 cases, with doubling time of more than 7 days, on par with Japan or Singapore (Figure 2, bottom panel).
These positive outcomes result from prompt, proactive actions of the government and collective efforts of the public. Unlike affluent Asian countries with GDP per capita of 20-fold higher, Vietnam could not afford a community-wide testing program. Instead, Vietnam has focused on cost-effective measures. At the centre of its active case finding are extensive contact tracing and health declaration for all. In combination with case isolation, mass quarantine and mass masking, these measures control infections at source, even asymptomatic cases. It is the early recognition of the outbreak, swiftly adaptive actions, production line of medical essentials and PPEs and the public’s cooperation that make these strategies feasible.
Nevertheless, as the pandemic is evolving rapidly, combating the disease becomes more challenging for Vietnam and the globe.
Source of funding
None.
Conflict of Interest statement
We declare no conflict of interest.
Author contributions
LD and TH conceived the idea of study. LD, PD, PDMN, DHNN and TH collected data. LD and TH wrote the manuscript. All authors reviewed and edited the manuscript.

{kind=link}
{kind=link}