Abstract
Radiotherapy for prostate cancer causes erectile dysfunction (ED) in about 40% of the patients. Hypofractionated radiotherapy has become the new clinical standard for prostate cancer. Several randomized trials reported non-inferiority of hypofractionated radiotherapy with respect to late toxicity. We investigated the effect on erectile function of moderate hypofractionation (MHF = 20x3/3.1Gy) and ultra-hypofractionation (UHF = 7x6.1Gy) in clinical practice.
We evaluated n = 168 cT1-cT2 prostate cancer patients treated with UHF (n = 113) or MHF (n = 55) without androgen-deprivation therapy who were included in the prospective cohort study “Health-Related Quality of Life in Prostate Cancer Patients treated with Radiotherapy” (PRORAD) in 2019-2023. UHF was restricted to patients with adequate urinary function. The radiation dose was prescribed to the prostate +/- base of seminal vesicles, depending on the risk group. Questionnaires were distributed at baseline, end of treatment, 3-6-12-24-36-48-60 months post-radiotherapy. Erectile function was scored with the abridged five-item version of the International Index of Erectile Function (IIEF-5). We evaluated collected data at baseline, and 6-12-24-36 months after treatment. Defined ED categories were: no (22-25 points), mild (17-21), mild-to-moderate (12-16), moderate (8-11), and severe ED (5-7).
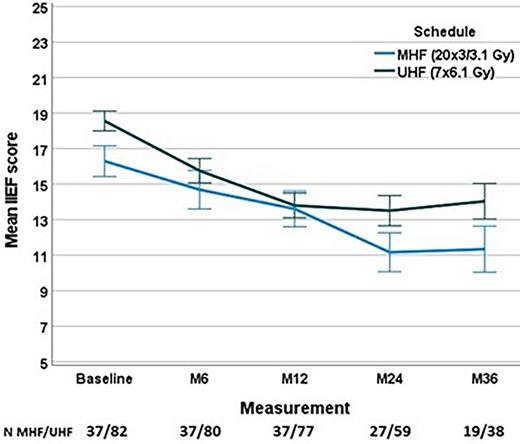
Median follow-up was 24 months. Of those patients who had none-to-mild ED at baseline (score > =17, n = 73, 43%), 7.2%, 18.9% and 13.9% reported severe ED at 12-24-36 months, respectively. At baseline, n = 49 (29%) reported severe ED. Average scores (with 1 standard error) over time are shown in the Figure for the remaining n = 119, per treatment group. The risk of developing severe ED significantly correlated with baseline erectile function (p < 0.001). At last follow-up, severe ED was reported in 5%, 24%, 33% and 68% in the subgroup with no, mild, mild-to-moderate and moderate ED at baseline, respectively. In patients with a baseline IIEF score > =12 (n = 100), 19% had developed severe ED at last follow-up (MHF 24%, UHF 17%, p = 0.5).
MHF and UHF were associated with a similar decrease in erectile function in this patient population, with results comparing favourably with conventionally fractionated radiotherapy reported in the literature. The risk of developing severe ED significantly correlated with baseline erectile function.
None.