




The 57-year-old male patient, previously diagnosed with nasopharyngeal carcinoma, felt pain in the pharynx. 18F-fluorodeoxyglucose (FDG) positron emission tomography/computed tomography (PET/CT) showed that the nasopharyngeal carcinoma invaded the skull base (Fig. 1b–d), with bilateral multiple lymph node metastases in the neck (Fig. 1a), the metabolism of many muscles in the right hip and knee was diffusely and unevenly elevated (Fig. 1a, e–h, 57.6 cm, SUVmax = 18). Multiple hypermetabolic lymph nodes were found in the right groin and right thigh (Fig. 1e and f). CT showed swelling of soft tissues with slightly decreased density, surrounded by muscular lymph nodes. Physical examination found swelling from the right hip to the right knee with no hint of haphalgesia or abnormality in knee movement.
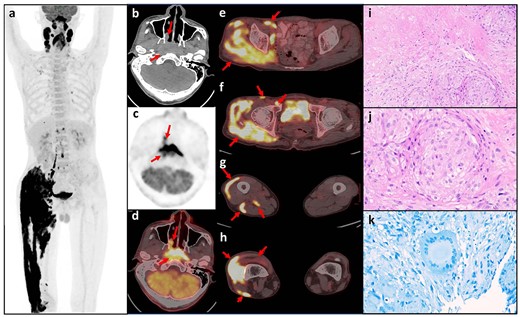
(a) Maximum intensity projection of FDG PET; (b–d) axial PET/CT showing nasopharyngeal carcinoma invading the skull base; (e–h) axial PET/CT showing hypermetabolic lymph nodes in the right groin and unevenly elevated metabolism in the thigh muscles; (i–j) HE staining showed coagulative necrosis surrounded by granulomatous inflammation, mainly composed of epithelioid cells (i, ×200) and a few lymphocytes (j, ×400); (k) acid-fast staining revealed multinucleated giant cells.
The patient’s history of malignancy, no abnormal discomfort in the right crura and extensive hypermetabolism in the right crura revealed by PET/CT examination could be mistaken as malignancy, with lymphoma being the first consideration.
Histopathological results for the biopsy confirmed non-keratinous undifferentiated carcinoma of the nasopharynx and metastatic non-keratinous undifferentiated carcinoma of the neck lymph nodes. Soft tissue biopsy of the right lateral knee showed granulomatous inflammation with coagulative necrosis (Fig. 1i–k). γ-interferon release test was positive (+) and serological C-reactive protein was elevated. Microscopic examination for acid-resistant bacilli (antacid staining) was negative. Seven strict sequences of Mycobacterium tuberculosis complexes were found by subsequent metagenomic next-generation sequencing (mNGS) of preserved muscle specimens, and relative abundance of bacteria was 0.02%. Multi-Disciplinary Team recommended a 1-month anti-tuberculosis treatment followed by chemotherapy and radiotherapy. The patient has now completed local radiotherapy for nasopharyngeal carcinoma. Follow-up visits were conducted 1 month (by phone) and 3 months (in person) after anti-tuberculosis treatment and the patient is now in stable condition.
Muscular tuberculosis (TB) is an extremely rare entity accounting for only 1–3% of all TB cases (1,2). Patients with malignant tumors are a high-risk group for TB, and the clinical symptoms and signs are often atypical when combined with TB (3). Accurate diagnosis is usually difficult to achieve by pathological examination alone, and laboratory tests are of high importance. In our case, due to the unexpected detection of extensive and atypical TB lesions in the lower extremities by PET/CT, we realized that there were possibilities other than lymphoma. The diagnosis of muscular TB was further evidenced by morphological, pathogenic examination and mNGS etiological study. These findings have changed the clinical treatment plan and provided a new experience of extra-pulmonary TB manifestation by PET/CT to reduce misdiagnosis.
Conflict of interest statement
None declared.
Ethics approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the principles of the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Consent to participate
Informed consent was taken from the patient for the publication of this case report and related imaging.

{kind=link}