





Sir,
Resistance of Gram-negative pathogens to current antibiotics has revived interest in earlier and often disused molecules for which resistance is still low. Yet, detailed pharmacokinetic/pharmacodynamic data are scarce for these drugs. A typical example is temocillin (6-α-methoxy-ticarcillin), active against most Gram-negative bacteria, which shows stability against a variety of β-lactamases, including most ESBLs, AmpC and some carbapenemases. Temocillin represents a strategic sparing alternative to carbapenems.1 There is no EUCAST breakpoint set for temocillin, but in recent surveys, MIC90 values of 8–16 mg/L were reported for ESBL and AmpC producers.2,3 The main driver of efficacy of β-lactams is the fraction of time between successive administrations during which their free concentration remains above the MIC for the offending organism. For penicillins, it is generally accepted that this fraction must reach 40% of the dosing interval. However, more demanding targets (such as maintaining unbound concentrations >4 times the MIC for the offending organism) have been advocated for severe infections in critically ill patients4 and for preventing the emergence of resistance.5 This may require the use of large doses as well as implementing continuous infusion as done routinely for temocillin in our ICU.6 Yet, many infections are located deep in tissues, highlighting the importance of antibiotic tissue penetration in the final outcome of the treatment. In this context, we report here the case of a critically ill patient in whom we could measure temocillin concentration in the pancreatic tissue. Written informed consent was obtained from the patient’s relatives for collecting samples.
A female in her early fifties was transferred to our ICU from another institution because of severe necrotizing pancreatitis secondary to duodenal perforation after endoscopic retrograde cholangiopancreatography. She received meropenem for >2 weeks for suspicion of a pancreatic infection. In the third week after admission, her condition deteriorated with development of septic shock. A duodenal fistula was documented and blood cultures grew for Klebsiella pneumoniae with MICs (Etest) of 12 mg/L for meropenem (categorized as resistant) and 16 mg/L for temocillin. Temocillin was given for 10 days by continuous infusion at a daily dose of 6 g owing to the low susceptibility of the pathogen, even though the patient was under continuous haemofiltration (owing to acute renal failure; glomerular filtration rate = 20 mL/min). Temocillin total and unbound concentrations were quantified in plasma samples collected every 24 h from day 5 to day 9, using a validated LC–tandem MS method.7 Bacteraemia had resolved after 10 days of treatment, but surgical debridement was required to remove infected pancreatic tissue, giving us the opportunity to collect a necrotic sample at day 8 and to measure its temocillin content. In brief, the sample was washed in saline, dried at 40°C for 24 h (temocillin stability was >90% in these conditions), homogenized in saline, reconstituted in ethyl acetate containing internal standard (ticarcillin) and phosphate buffer pH 9.2, and centrifuged at 4°C for 5 min at 11 000 g. The organic phase was collected, evaporated and reconstituted in 20 μL of mobile phase for assay as described for plasma samples,7 with a calibration curve using a fragment of porcine pancreas spiked with temocillin and treated by the same procedure.
Mean unbound and total temocillin concentrations in plasma remained stable over time during the sampling period (69.8 ± 5.2 and 112.5 ± 2.9 mg/L, respectively; see Figure 1). These high levels are probably explained by the patient’s renal insufficiency. Notably, the unbound concentrations, which were high probably owing to the low plasma protein level (44.6 ± 1.6 g/L; see discussion in Alexandre and Fantin3 and Laterre et al.6), were continuously >4 times the MIC for the offending organism. Temocillin content in the tissue homogenate was 186 μg/g, which could be approximated to 186 mg/L.8 Such a high concentration was unexpected, because β-lactams show a low distribution volume (denoting a lack of tissue accumulation), and because necrotic tissue is poorly vascularized. It could be related to the long-lasting exposure of the tissue to stable, elevated serum levels afforded by the continuous infusion, the high unbound plasma concentrations in this patient and the low perfusion of the organ, which could reduce the clearance of the drug if bound to tissue constituents. As we used whole-tissue homogenate, this value represents the mean concentration of drug present extracellularly or intracellularly. In most publications, the temocillin concentrations in tissues and body fluids represent 8%–65% of the total serum concentrations (see Alexandre and Fantin3 for review), but these may not represent values at equilibrium since temocillin was given by discontinuous infusion. Moreover, these studies were not performed in critically ill patients. Finally, total tissue levels could be high owing to low serum protein concentration, resulting in a temocillin equilibrium shift in favour of the tissue. This is of particular importance for drugs with non-linear protein binding9 such as temocillin. Thus, although limited to a single case, these data suggest that temocillin may reach therapeutic levels in some tissues and encourage further studies in this area.
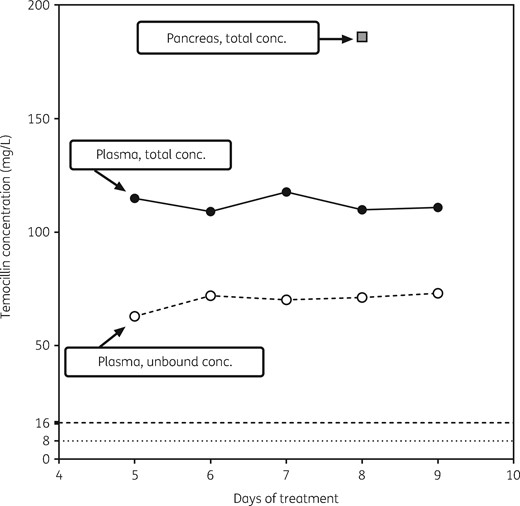
Concentration of total (filled circles) and unbound (open circles) temocillin in plasma samples and of total temocillin in pancreatic homogenate (grey squares) collected from a critically ill patient receiving 6 g per day by continuous infusion. Plasma samples were collected from day 5 to day 9 of treatment, and the pancreatic biopsy was collected at day 8. The horizontal broken lines correspond to typical MIC90 values reported in recent surveys for Enterobacteriaceae producing ESBLs (8 and 16 mg/L).
Acknowledgements
We are grateful to the on-site nurses for their participation and to M. Vergauwen (Chirurgie Expérimentale et Transplantation; Université catholique de Louvain) for providing us with a sample of porcine pancreas.
Funding
This study was carried out as part of our routine work.
Transparency declarations
P. N. P. is an employee of the Université catholique de Louvain. A. C. was and P. W. and P.-F. L. are employees of the Cliniques universitaires Saint-Luc. P. M. T. was unpaid. F. V. B. is Research Director of the Fonds de la Recherche Scientifique (F.R.S.-FNRS). P. M. T. is an unpaid advisor to Eumedica, the registration holder of temocillin.

{kind=link}