





This paper provides an update to the original cohort profile paper published a decade ago. The Millennium Cohort Study is the largest, longest-running, prospective study of current and former United States (US) military personnel and is sponsored by the US Departments of Defense (DoD) and Veterans Affairs (VA).
While the original study aim, evaluating the health impact of serving in the military, has remained consistent, the spectrum of research topics has expanded to include areas such as social determinants of health.
260 228 military personnel enrolled across 5 panels between 2001 and 2021 (baseline age range: 25-35 years); participants are surveyed every 3-5 years. The original 21-year follow-up period was extended through 2068 to examine health across the lifespan.
Longitudinal survey data are linked to data from DoD, VA, and external sources (e.g. medical records, deployment histories, vital statistics, and geospatial data).
For inquiries about collaboration, contact the Principal Investigator at usn.point-loma.navhlthrschcensan.mbx.nhrcmillennium-cohort-pi@health.mil
The original cohort
The Millennium Cohort Study (henceforth referred to as the Study) is a prospective occupational cohort study designed to examine the effects of military service, including deployments and other occupational exposures, on the long-term health and wellbeing of US service members and veterans.1,2 Sponsored by the US Departments of Defense (DoD) and Veterans Affairs (VA), the Study was launched in 2001, prior to the terrorist attacks on September 11, 2001. The Study was initiated in response to Section 743 in the Strom Thurmond National Defense Authorization Act (NDAA) for Fiscal Year 1999 (Public Law 105–261), which directed the Secretary of Defense ‘to establish a center devoted to a longitudinal study to evaluate data on the health conditions of members of the Armed Forces upon their return from deployment on military operations for purposes of ensuring the rapid identification of any trends in diseases, illnesses, or injuries among such members as a result of such operations’.3 Study findings are used to inform and guide policy, clinical practice guidelines and health promotion efforts. The original cohort profile publication1 described the initial study design, methods and the characteristics of the first three panels (n = 151 597) of service members who were enrolled into the Study from 2001 to 2008. The original study timeline was planned to end in 2022. Since original publication, the Study has grown to 260 228 participants with the additions of Panels 4 and 5 and extended its follow-up period through 2068 (Figure 1).
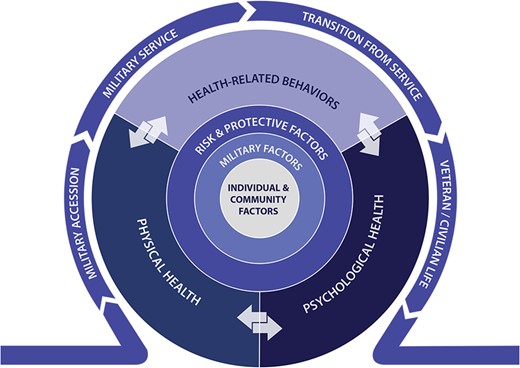
Conceptual model describing the Millennium Cohort Study research areas among service members and veterans through the life course. Reproduced from the following article that is published under the terms of the Creative Commons Attribution-Noncommercial-No Derivatives (CC BY NC ND) License. Belding JN, Castañeda SF, Jacobson IG et al. The Millennium Cohort Study: The first 20 years of research dedicated to understanding the long-term health of US Service Members and Veterans. Ann Epidemiol 2022;67:61–72. doi: 10.1016/j.annepidem.2021.12.002. Epub 2021 Dec 11. PMID: 34906635
What is the reason for the new data collection?
The study extension led to additional panels being enrolled, continued follow-up survey data collection and data linkages to enable broader examination of outcomes across the service member’s life course. In this time period, additional ancillary cohort studies of military spouses (Millennium Cohort Family Study) and military-affiliated children (Study of Adolescent Resilience) were also launched. These studies allow researchers to examine additional social determinants of health and long-term health outcomes and explore effects military service on military families. For example, since the original cohort profile publication,1 new survey data have been collected on sexual orientation, gender identity, homelessness, relationship quality, unit cohesion, adverse childhood experiences, discrimination, bullying, hazing, health care access and utilization and traumatic brain injury (see Table 1).
Survey measures available over time
| Domain | Measure/scale | Survey cycle availability | |||||
|---|---|---|---|---|---|---|---|
| 2001–03 | 2004–06 | 2007–08 | 2011–13 | 2014–16 | 2019–21 | ||
| Sociodemographic factors | Financial problems | X | X | X | X | X | X |
| Marital status | X | X | X | X | X | X | |
| Occupation (e.g. military and civilian)a | X | X | X | X | X | ||
| Educational attainment | X | X | X | X | X | ||
| Employment and household income | X | X | X | ||||
| Homelessness | X | X | |||||
| Household composition and relationship quality | X | X | |||||
| Sexual orientation | X | X | |||||
| Gender identity | X | ||||||
| Military service factors | Combat experiences | X | X | X | X | X | X |
| Environmental exposuresa | X | X | X | X | X | ||
| Deployments (e.g. locations and dates)a | X | X | X | X | |||
| Military satisfaction | X | X | X | X | |||
| Military separationa | X | X | X | X | |||
| Morale and unit cohesion | X | X | |||||
| Stressful life events | Stressful life events | X | X | X | X | X | X |
| Sexual harassment and assault | X | X | X | X | X | X | |
| Adverse childhood experiences | X | X | |||||
| Discrimination, bullying, harassment and hazing | X | ||||||
| Psychosocial factors | Posttraumatic stress disordera | X | X | X | X | X | X |
| Depressiona | X | X | X | X | X | X | |
| Panic/anxietya | X | X | X | X | X | X | |
| Disordered eating | X | X | X | X | X | X | |
| Social support | X | X | X | X | X | X | |
| Anger | X | X | |||||
| Posttraumatic growth, self-mastery | X | X | |||||
| Health-related behaviours | Tobacco and alcohol use | X | X | X | X | X | X |
| Sleep (e.g. duration, medications, disorders) | X | X | X | X | X | X | |
| Fast food, dietary supplements, caffeine intake | X | X | X | X | X | ||
| Physical activity and sedentary behaviour | X | X | X | X | |||
| Physical health, illness, and injury | Body mass index (BMI) | X | X | X | X | X | X |
| Physical health symptoms (e.g. pain, somatic symptoms) | X | X | X | X | X | X | |
| Reproductive healtha | X | X | X | X | X | X | |
| Quality of life/functional health | X | X | X | X | X | X | |
| Hospital daysa and lost workdays | X | X | X | X | X | ||
| Traumatic brain injurya | X | X | X | X | |||
| Motor vehicle injury | X | X | X | ||||
| Respiratory healtha | X | ||||||
| Medical conditions and health care utilization | Medical diagnosesa | X | X | X | X | X | X |
| Medications (e.g. pain)a | X | X | X | X | X | X | |
| Disability | X | X | X | X | X | X | |
| Complementary and alternative medicine | X | X | X | X | X | ||
| Vaccination (i.e. anthrax and smallpox)a | X | X | X | X | |||
| Access (e.g. health insurance) and health and mental health care utilizationa | X | X | |||||
| Domain | Measure/scale | Survey cycle availability | |||||
|---|---|---|---|---|---|---|---|
| 2001–03 | 2004–06 | 2007–08 | 2011–13 | 2014–16 | 2019–21 | ||
| Sociodemographic factors | Financial problems | X | X | X | X | X | X |
| Marital status | X | X | X | X | X | X | |
| Occupation (e.g. military and civilian)a | X | X | X | X | X | ||
| Educational attainment | X | X | X | X | X | ||
| Employment and household income | X | X | X | ||||
| Homelessness | X | X | |||||
| Household composition and relationship quality | X | X | |||||
| Sexual orientation | X | X | |||||
| Gender identity | X | ||||||
| Military service factors | Combat experiences | X | X | X | X | X | X |
| Environmental exposuresa | X | X | X | X | X | ||
| Deployments (e.g. locations and dates)a | X | X | X | X | |||
| Military satisfaction | X | X | X | X | |||
| Military separationa | X | X | X | X | |||
| Morale and unit cohesion | X | X | |||||
| Stressful life events | Stressful life events | X | X | X | X | X | X |
| Sexual harassment and assault | X | X | X | X | X | X | |
| Adverse childhood experiences | X | X | |||||
| Discrimination, bullying, harassment and hazing | X | ||||||
| Psychosocial factors | Posttraumatic stress disordera | X | X | X | X | X | X |
| Depressiona | X | X | X | X | X | X | |
| Panic/anxietya | X | X | X | X | X | X | |
| Disordered eating | X | X | X | X | X | X | |
| Social support | X | X | X | X | X | X | |
| Anger | X | X | |||||
| Posttraumatic growth, self-mastery | X | X | |||||
| Health-related behaviours | Tobacco and alcohol use | X | X | X | X | X | X |
| Sleep (e.g. duration, medications, disorders) | X | X | X | X | X | X | |
| Fast food, dietary supplements, caffeine intake | X | X | X | X | X | ||
| Physical activity and sedentary behaviour | X | X | X | X | |||
| Physical health, illness, and injury | Body mass index (BMI) | X | X | X | X | X | X |
| Physical health symptoms (e.g. pain, somatic symptoms) | X | X | X | X | X | X | |
| Reproductive healtha | X | X | X | X | X | X | |
| Quality of life/functional health | X | X | X | X | X | X | |
| Hospital daysa and lost workdays | X | X | X | X | X | ||
| Traumatic brain injurya | X | X | X | X | |||
| Motor vehicle injury | X | X | X | ||||
| Respiratory healtha | X | ||||||
| Medical conditions and health care utilization | Medical diagnosesa | X | X | X | X | X | X |
| Medications (e.g. pain)a | X | X | X | X | X | X | |
| Disability | X | X | X | X | X | X | |
| Complementary and alternative medicine | X | X | X | X | X | ||
| Vaccination (i.e. anthrax and smallpox)a | X | X | X | X | |||
| Access (e.g. health insurance) and health and mental health care utilizationa | X | X | |||||
Objective measures, in addition to self-reported measures, have been available for this variable throughout the Study period (see Table 3).
Survey measures available over time
| Domain | Measure/scale | Survey cycle availability | |||||
|---|---|---|---|---|---|---|---|
| 2001–03 | 2004–06 | 2007–08 | 2011–13 | 2014–16 | 2019–21 | ||
| Sociodemographic factors | Financial problems | X | X | X | X | X | X |
| Marital status | X | X | X | X | X | X | |
| Occupation (e.g. military and civilian)a | X | X | X | X | X | ||
| Educational attainment | X | X | X | X | X | ||
| Employment and household income | X | X | X | ||||
| Homelessness | X | X | |||||
| Household composition and relationship quality | X | X | |||||
| Sexual orientation | X | X | |||||
| Gender identity | X | ||||||
| Military service factors | Combat experiences | X | X | X | X | X | X |
| Environmental exposuresa | X | X | X | X | X | ||
| Deployments (e.g. locations and dates)a | X | X | X | X | |||
| Military satisfaction | X | X | X | X | |||
| Military separationa | X | X | X | X | |||
| Morale and unit cohesion | X | X | |||||
| Stressful life events | Stressful life events | X | X | X | X | X | X |
| Sexual harassment and assault | X | X | X | X | X | X | |
| Adverse childhood experiences | X | X | |||||
| Discrimination, bullying, harassment and hazing | X | ||||||
| Psychosocial factors | Posttraumatic stress disordera | X | X | X | X | X | X |
| Depressiona | X | X | X | X | X | X | |
| Panic/anxietya | X | X | X | X | X | X | |
| Disordered eating | X | X | X | X | X | X | |
| Social support | X | X | X | X | X | X | |
| Anger | X | X | |||||
| Posttraumatic growth, self-mastery | X | X | |||||
| Health-related behaviours | Tobacco and alcohol use | X | X | X | X | X | X |
| Sleep (e.g. duration, medications, disorders) | X | X | X | X | X | X | |
| Fast food, dietary supplements, caffeine intake | X | X | X | X | X | ||
| Physical activity and sedentary behaviour | X | X | X | X | |||
| Physical health, illness, and injury | Body mass index (BMI) | X | X | X | X | X | X |
| Physical health symptoms (e.g. pain, somatic symptoms) | X | X | X | X | X | X | |
| Reproductive healtha | X | X | X | X | X | X | |
| Quality of life/functional health | X | X | X | X | X | X | |
| Hospital daysa and lost workdays | X | X | X | X | X | ||
| Traumatic brain injurya | X | X | X | X | |||
| Motor vehicle injury | X | X | X | ||||
| Respiratory healtha | X | ||||||
| Medical conditions and health care utilization | Medical diagnosesa | X | X | X | X | X | X |
| Medications (e.g. pain)a | X | X | X | X | X | X | |
| Disability | X | X | X | X | X | X | |
| Complementary and alternative medicine | X | X | X | X | X | ||
| Vaccination (i.e. anthrax and smallpox)a | X | X | X | X | |||
| Access (e.g. health insurance) and health and mental health care utilizationa | X | X | |||||
| Domain | Measure/scale | Survey cycle availability | |||||
|---|---|---|---|---|---|---|---|
| 2001–03 | 2004–06 | 2007–08 | 2011–13 | 2014–16 | 2019–21 | ||
| Sociodemographic factors | Financial problems | X | X | X | X | X | X |
| Marital status | X | X | X | X | X | X | |
| Occupation (e.g. military and civilian)a | X | X | X | X | X | ||
| Educational attainment | X | X | X | X | X | ||
| Employment and household income | X | X | X | ||||
| Homelessness | X | X | |||||
| Household composition and relationship quality | X | X | |||||
| Sexual orientation | X | X | |||||
| Gender identity | X | ||||||
| Military service factors | Combat experiences | X | X | X | X | X | X |
| Environmental exposuresa | X | X | X | X | X | ||
| Deployments (e.g. locations and dates)a | X | X | X | X | |||
| Military satisfaction | X | X | X | X | |||
| Military separationa | X | X | X | X | |||
| Morale and unit cohesion | X | X | |||||
| Stressful life events | Stressful life events | X | X | X | X | X | X |
| Sexual harassment and assault | X | X | X | X | X | X | |
| Adverse childhood experiences | X | X | |||||
| Discrimination, bullying, harassment and hazing | X | ||||||
| Psychosocial factors | Posttraumatic stress disordera | X | X | X | X | X | X |
| Depressiona | X | X | X | X | X | X | |
| Panic/anxietya | X | X | X | X | X | X | |
| Disordered eating | X | X | X | X | X | X | |
| Social support | X | X | X | X | X | X | |
| Anger | X | X | |||||
| Posttraumatic growth, self-mastery | X | X | |||||
| Health-related behaviours | Tobacco and alcohol use | X | X | X | X | X | X |
| Sleep (e.g. duration, medications, disorders) | X | X | X | X | X | X | |
| Fast food, dietary supplements, caffeine intake | X | X | X | X | X | ||
| Physical activity and sedentary behaviour | X | X | X | X | |||
| Physical health, illness, and injury | Body mass index (BMI) | X | X | X | X | X | X |
| Physical health symptoms (e.g. pain, somatic symptoms) | X | X | X | X | X | X | |
| Reproductive healtha | X | X | X | X | X | X | |
| Quality of life/functional health | X | X | X | X | X | X | |
| Hospital daysa and lost workdays | X | X | X | X | X | ||
| Traumatic brain injurya | X | X | X | X | |||
| Motor vehicle injury | X | X | X | ||||
| Respiratory healtha | X | ||||||
| Medical conditions and health care utilization | Medical diagnosesa | X | X | X | X | X | X |
| Medications (e.g. pain)a | X | X | X | X | X | X | |
| Disability | X | X | X | X | X | X | |
| Complementary and alternative medicine | X | X | X | X | X | ||
| Vaccination (i.e. anthrax and smallpox)a | X | X | X | X | |||
| Access (e.g. health insurance) and health and mental health care utilizationa | X | X | |||||
Objective measures, in addition to self-reported measures, have been available for this variable throughout the Study period (see Table 3).
What will be the new areas of research?
The Study’s major research priorities remain consistent with its legislative mandate and broadly include overarching programme areas that address psychological and physical health and health-related behaviours (Figure 1).2,4 The breadth of research topics has expanded over the past decade in response to the increasing sociodemographic diversity of the military reflected in the Cohort population, shifting stakeholder priorities and the continued expansion of sources for data integration. Some of these expanded topics include military-to-civilian transitions (e.g. economic difficulties), post-service life experiences (e.g. homelessness) and equity and inclusion. Reflecting the joint sponsorship of the DoD and VA, the research on veterans’ health has grown. New ancillary studies of spouses and children of service members have enabled examination of the health and relationship adjustment of military families. Furthermore, the Study has established additional linkages with DoD, VA, and other federal databases such as health care utilization, mortality and geospatial databases.
Who is in the cohort?
Recruitment of potential participants involves sampling of US service members (i.e. active duty, Reserve and National Guard personnel) from rosters maintained by the US Defense Manpower Data Center (DMDC), the central DoD source for personnel, manpower, training and financial databases. The first panel of participants (Panel 1) consisted of service members from a probability-based sample of the entire military population as of October 2000 and enrolled in 2001–03. A sample of service members was invited to Panel 1, regardless of length of service, with an oversampling of women, Reserves/National Guard and those with prior deployment experience. Additional random samples of personnel with 1 to 5 years of military service were invited to join subsequent enrolment panels in 2004–06 (Panel 2), 2007–08 (Panel 3), 2011–13 (Panel 4) and 2020–21 (Panel 5). Specific groups (e.g. women, Marines for Panels 2–3; women, married personnel for Panels 4–5) were intentionally oversampled to enable sufficient sample size for sub-group comparisons (Figure 2). Invitations to enrol in the study and to complete follow-up surveys were initially sent through email, where invitees are prompted to consent and fill out surveys online, with additional paper reminders (e.g. postcards, newsletters and paper surveys). Panel 5 is the first panel recruited using a web-only survey with minimal print reminders.
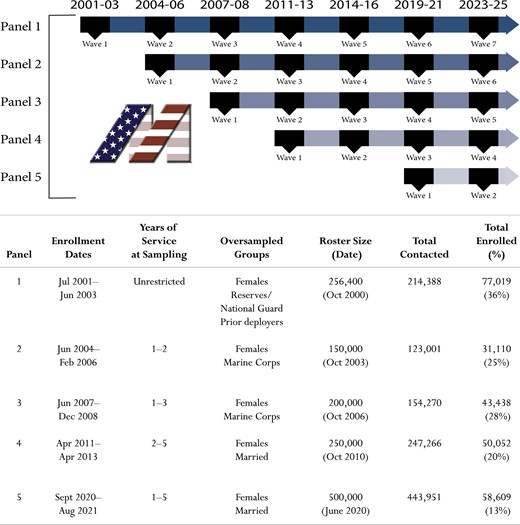
Timeline for enrolment and follow-up data collection by panel. Adapted from the following article that is published under the terms of the CC BY NC ND License. Belding JN, Castañeda SF, Jacobson IG et al. The Millennium Cohort Study: The first 20 years of research dedicated to understanding the long-term health of US Service Members and Veterans. Ann Epidemiol 2022;67:61–72. doi: 10.1016/j.annepidem.2021.12.002. Epub 2021 Dec 11. PMID: 34906635
With the enrolment of two additional panels since publication of the original cohort profile paper in 2012, the Study population has increased in size from 151 597 to 260 228. Enrolled participants represent all service branches (i.e. Army, Marine Corps, Navy, Air Force, Space Force and Coastguard), service components (i.e. active duty, Reserves and National Guard), pay grades (i.e. enlisted and officers) and a diversity of racial and ethnic groups (Table 2). Currently, over half of the Study population is currently no longer in military service.
Sociodemographic and military characteristics by enrolment panel
| Characteristics at study enrolmentd | Overall | Panel 1 | Panel 2 | Panel 3 | Panel 4 | Panel 5 |
|---|---|---|---|---|---|---|
| N = 260 228 | N = 77 019 | N = 31 110 | N = 43 438 | N = 50 052 | N = 58 609 | |
| (%) | (%) | (%) | (%) | (%) | (%) | |
| Enrolment period | 2001–21 | 2001–03 | 2004–06 | 2007–08 | 2011–13 | 2020–21 |
| Age [M, standard deviation (SD)] | 29 (8) | 35 (9) | 25 (5) | 25 (4) | 27 (5) | 26 (5) |
| Sex | ||||||
| Male | 69 | 73 | 62 | 64 | 73 | 69 |
| Female | 31 | 27 | 38 | 36 | 27 | 31 |
| Race and ethnicity | ||||||
| American Indian or Alaska Native | 1 | 1 | 1 | 2 | 2 | 1 |
| Asian or Pacific Islander | 6 | 3 | 5 | 6 | 5 | 9 |
| Black, Non-Hispanic | 12 | 14 | 12 | 11 | 10 | 13 |
| Hispanic or Latino | 10 | 6 | 10 | 8 | 9 | 19 |
| Multiethnic or othera | 2 | 2 | 1 | 1 | 1 | 3 |
| White, Non-Hispanic | 69 | 74 | 71 | 72 | 73 | 55 |
| Paygrade | ||||||
| Enlisted | 82 | 77 | 88 | 89 | 84 | 80 |
| Officer | 18 | 23 | 12 | 11 | 16 | 20 |
| Service component | ||||||
| Active duty | 70 | 57 | 60 | 79 | 73 | 85 |
| Reserve or National Guard | 30 | 43 | 40 | 21 | 27 | 15 |
| Service branch | ||||||
| Air Forceb | 31 | 29 | 27 | 30 | 29 | 39 |
| Army | 43 | 47 | 48 | 36 | 45 | 35 |
| Coastguard | 2 | 1 | 1 | 3 | 3 | 3 |
| Marine Corps | 9 | 5 | 8 | 16 | 10 | 11 |
| Navy | 15 | 17 | 16 | 16 | 14 | 11 |
| Age in 2023c (M, SD) | 42 (12) | 56 (9) | 43 (5) | 40 (4) | 39 (5) | 29 (5) |
| Separated from the Militaryc | 60 | 93 | 73 | 66 | 59 | 4 |
| Deployment 2001–22c | 60 | 54 | 71 | 78 | 78 | 36 |
| Deceasedc | 2 | 4 | 2 | 1 | 1 | 0 |
| Characteristics at study enrolmentd | Overall | Panel 1 | Panel 2 | Panel 3 | Panel 4 | Panel 5 |
|---|---|---|---|---|---|---|
| N = 260 228 | N = 77 019 | N = 31 110 | N = 43 438 | N = 50 052 | N = 58 609 | |
| (%) | (%) | (%) | (%) | (%) | (%) | |
| Enrolment period | 2001–21 | 2001–03 | 2004–06 | 2007–08 | 2011–13 | 2020–21 |
| Age [M, standard deviation (SD)] | 29 (8) | 35 (9) | 25 (5) | 25 (4) | 27 (5) | 26 (5) |
| Sex | ||||||
| Male | 69 | 73 | 62 | 64 | 73 | 69 |
| Female | 31 | 27 | 38 | 36 | 27 | 31 |
| Race and ethnicity | ||||||
| American Indian or Alaska Native | 1 | 1 | 1 | 2 | 2 | 1 |
| Asian or Pacific Islander | 6 | 3 | 5 | 6 | 5 | 9 |
| Black, Non-Hispanic | 12 | 14 | 12 | 11 | 10 | 13 |
| Hispanic or Latino | 10 | 6 | 10 | 8 | 9 | 19 |
| Multiethnic or othera | 2 | 2 | 1 | 1 | 1 | 3 |
| White, Non-Hispanic | 69 | 74 | 71 | 72 | 73 | 55 |
| Paygrade | ||||||
| Enlisted | 82 | 77 | 88 | 89 | 84 | 80 |
| Officer | 18 | 23 | 12 | 11 | 16 | 20 |
| Service component | ||||||
| Active duty | 70 | 57 | 60 | 79 | 73 | 85 |
| Reserve or National Guard | 30 | 43 | 40 | 21 | 27 | 15 |
| Service branch | ||||||
| Air Forceb | 31 | 29 | 27 | 30 | 29 | 39 |
| Army | 43 | 47 | 48 | 36 | 45 | 35 |
| Coastguard | 2 | 1 | 1 | 3 | 3 | 3 |
| Marine Corps | 9 | 5 | 8 | 16 | 10 | 11 |
| Navy | 15 | 17 | 16 | 16 | 14 | 11 |
| Age in 2023c (M, SD) | 42 (12) | 56 (9) | 43 (5) | 40 (4) | 39 (5) | 29 (5) |
| Separated from the Militaryc | 60 | 93 | 73 | 66 | 59 | 4 |
| Deployment 2001–22c | 60 | 54 | 71 | 78 | 78 | 36 |
| Deceasedc | 2 | 4 | 2 | 1 | 1 | 0 |
‘Other’ includes those who reported multiple races and ‘none’ or ‘other’ for ethnicity.
Air Force currently includes Space Force participants.
Recent age is as of April 2023 and vital status is as of April 2022. At least one deployment in support of post-9/11 operations, predominately to locations in and around the Middle East region between September 2001 and November 2022. Separation from the military is as of December 2021.
Percentages may not add to 100 percent due to rounding.
Sociodemographic and military characteristics by enrolment panel
| Characteristics at study enrolmentd | Overall | Panel 1 | Panel 2 | Panel 3 | Panel 4 | Panel 5 |
|---|---|---|---|---|---|---|
| N = 260 228 | N = 77 019 | N = 31 110 | N = 43 438 | N = 50 052 | N = 58 609 | |
| (%) | (%) | (%) | (%) | (%) | (%) | |
| Enrolment period | 2001–21 | 2001–03 | 2004–06 | 2007–08 | 2011–13 | 2020–21 |
| Age [M, standard deviation (SD)] | 29 (8) | 35 (9) | 25 (5) | 25 (4) | 27 (5) | 26 (5) |
| Sex | ||||||
| Male | 69 | 73 | 62 | 64 | 73 | 69 |
| Female | 31 | 27 | 38 | 36 | 27 | 31 |
| Race and ethnicity | ||||||
| American Indian or Alaska Native | 1 | 1 | 1 | 2 | 2 | 1 |
| Asian or Pacific Islander | 6 | 3 | 5 | 6 | 5 | 9 |
| Black, Non-Hispanic | 12 | 14 | 12 | 11 | 10 | 13 |
| Hispanic or Latino | 10 | 6 | 10 | 8 | 9 | 19 |
| Multiethnic or othera | 2 | 2 | 1 | 1 | 1 | 3 |
| White, Non-Hispanic | 69 | 74 | 71 | 72 | 73 | 55 |
| Paygrade | ||||||
| Enlisted | 82 | 77 | 88 | 89 | 84 | 80 |
| Officer | 18 | 23 | 12 | 11 | 16 | 20 |
| Service component | ||||||
| Active duty | 70 | 57 | 60 | 79 | 73 | 85 |
| Reserve or National Guard | 30 | 43 | 40 | 21 | 27 | 15 |
| Service branch | ||||||
| Air Forceb | 31 | 29 | 27 | 30 | 29 | 39 |
| Army | 43 | 47 | 48 | 36 | 45 | 35 |
| Coastguard | 2 | 1 | 1 | 3 | 3 | 3 |
| Marine Corps | 9 | 5 | 8 | 16 | 10 | 11 |
| Navy | 15 | 17 | 16 | 16 | 14 | 11 |
| Age in 2023c (M, SD) | 42 (12) | 56 (9) | 43 (5) | 40 (4) | 39 (5) | 29 (5) |
| Separated from the Militaryc | 60 | 93 | 73 | 66 | 59 | 4 |
| Deployment 2001–22c | 60 | 54 | 71 | 78 | 78 | 36 |
| Deceasedc | 2 | 4 | 2 | 1 | 1 | 0 |
| Characteristics at study enrolmentd | Overall | Panel 1 | Panel 2 | Panel 3 | Panel 4 | Panel 5 |
|---|---|---|---|---|---|---|
| N = 260 228 | N = 77 019 | N = 31 110 | N = 43 438 | N = 50 052 | N = 58 609 | |
| (%) | (%) | (%) | (%) | (%) | (%) | |
| Enrolment period | 2001–21 | 2001–03 | 2004–06 | 2007–08 | 2011–13 | 2020–21 |
| Age [M, standard deviation (SD)] | 29 (8) | 35 (9) | 25 (5) | 25 (4) | 27 (5) | 26 (5) |
| Sex | ||||||
| Male | 69 | 73 | 62 | 64 | 73 | 69 |
| Female | 31 | 27 | 38 | 36 | 27 | 31 |
| Race and ethnicity | ||||||
| American Indian or Alaska Native | 1 | 1 | 1 | 2 | 2 | 1 |
| Asian or Pacific Islander | 6 | 3 | 5 | 6 | 5 | 9 |
| Black, Non-Hispanic | 12 | 14 | 12 | 11 | 10 | 13 |
| Hispanic or Latino | 10 | 6 | 10 | 8 | 9 | 19 |
| Multiethnic or othera | 2 | 2 | 1 | 1 | 1 | 3 |
| White, Non-Hispanic | 69 | 74 | 71 | 72 | 73 | 55 |
| Paygrade | ||||||
| Enlisted | 82 | 77 | 88 | 89 | 84 | 80 |
| Officer | 18 | 23 | 12 | 11 | 16 | 20 |
| Service component | ||||||
| Active duty | 70 | 57 | 60 | 79 | 73 | 85 |
| Reserve or National Guard | 30 | 43 | 40 | 21 | 27 | 15 |
| Service branch | ||||||
| Air Forceb | 31 | 29 | 27 | 30 | 29 | 39 |
| Army | 43 | 47 | 48 | 36 | 45 | 35 |
| Coastguard | 2 | 1 | 1 | 3 | 3 | 3 |
| Marine Corps | 9 | 5 | 8 | 16 | 10 | 11 |
| Navy | 15 | 17 | 16 | 16 | 14 | 11 |
| Age in 2023c (M, SD) | 42 (12) | 56 (9) | 43 (5) | 40 (4) | 39 (5) | 29 (5) |
| Separated from the Militaryc | 60 | 93 | 73 | 66 | 59 | 4 |
| Deployment 2001–22c | 60 | 54 | 71 | 78 | 78 | 36 |
| Deceasedc | 2 | 4 | 2 | 1 | 1 | 0 |
‘Other’ includes those who reported multiple races and ‘none’ or ‘other’ for ethnicity.
Air Force currently includes Space Force participants.
Recent age is as of April 2023 and vital status is as of April 2022. At least one deployment in support of post-9/11 operations, predominately to locations in and around the Middle East region between September 2001 and November 2022. Separation from the military is as of December 2021.
Percentages may not add to 100 percent due to rounding.
What has been measured?
Survey measures
After providing informed consent and completing a baseline survey, participants are invited to complete follow-up surveys every 3 to 5 years through 2068. Five baseline and five follow-up surveys have been conducted to date (Figure 2). Study measures assessed over time are derived from validated measures or publicly available epidemiological survey sources. Although constructs assessed have largely remained consistent over time, certain measures have changed in response to developments in research priorities, military policy, stakeholder input or scientific advances. A summary of the survey measures is described below and listed in Table 1.
Sociodemographic factors
Financial problems, marital status, occupation (military and civilian) and educational attainment have been consistently assessed over time. The survey has expanded to assess employment (e.g. unemployed, part-time, full-time), household income, homelessness, household composition, relationship quality, sexual orientation and gender identity.
Military service characteristics
Service-related factors that have been consistently assessed over time include combat experiences, environmental exposures, deployments (e.g. locations and dates), military satisfaction and reasons for separating from the military. Assessment of unit cohesion was recently added.
Stressful life events
Varying stressful events stemming from the Social Readjustment Rating Scale have been assessed over time.5 More recently, detailed assessments of sexual harassment and assault and additional life stressors, such as adverse childhood experiences,6 discrimination, bullying, harassment and hazing experienced have been included.
Psychosocial factors
Posttraumatic stress disorder (PTSD) has been measured using the PTSD Checklist (PCL), originally with the PCL Civilian Version (PCL-C) and more recently with the PCL for DSM-5 (PCL-5).7 In addition, major depressive disorder has been measured using the Patient Health Questionnaire (PHQ)-9 or PHQ-8,8 with other anxiety syndrome, panic syndrome and disordered eating measured using additional corresponding modules in the PHQ.9 Social support has been consistently measured using an item from the PHQ and a six-item version of the Multidimensional Scale of Perceived Social Support (MSPSS) was added more recently. 10 More recent psychosocial factors include anger measured by the Dimensions of Anger Reactions-5 (DAR-5),11 positive outlook measured by a modified ‘current standing’ short form of the current-state beliefs Posttraumatic Growth Inventory, short-form (C-PTGI-SF)12 and self-mastery measured by the Perlin Mastery Scale.13
Health-related behaviours
Tobacco use has been included since the Study’s beginning (e.g. lifetime cigarette use, quit attempts, use of other tobacco products) with vaping and e-cigarette use recently added. Alcohol use (e.g. heavy weekly drinking, binge drinking, problem drinking and potential alcohol dependence) has been assessed throughout the duration of the study.14 In addition, varying sleep measures have been included over time, including sleep duration15 and insomnia symptoms measured by the PHQ anxiety screen and the PCL-C,9,16 clinical insomnia measured by the Insomnia Severity Index (ISI),17 and sleep medication use from the Pittsburg Sleep Quality Index (PSQI).18 In addition, fast-food consumption,19 dietary supplement use, caffeine intake, physical activity and sedentary time20 have been included.
Physical health, illness and injury
Body mass index calculated from self-reported height and weight, physical health symptoms (e.g. pain, somatic symptoms),21,22 reproductive health and quality of life/functional health assessed by the Short Form 36-item Health Survey for Veterans (SF-36V) or Veterans RAND 12 Item Health Survey23 have been assessed over time. In addition, traumatic brain injury, motor vehicle injury, hospital days and lost workdays due to illness or injury have been assessed over time.
Medical conditions and health care utilization
Self-reported medical diagnoses (e.g. asthma, diabetes, heart disease, cancer, sleep apnoea, chronic bronchitis, emphysema, PTSD, infertility), complementary and alternative medicine use, medication use, disability and vaccinations (e.g. anthrax and smallpox) have been assessed over time. More recently, access to health care (e.g. health insurance coverage), and health and mental health care utilization have been assessed.
Data linkages
Historically, the Study has linked survey data with military electronic medical records and administrative datasets to address specific research questions and hypotheses. Sociodemographic factors (e.g. sex, age, marital status, race and ethnicity) and military factors (e.g. pay grade, service branch, time in service, military occupation, service component and separation) are obtained from the DMDC. Detailed deployment characteristics (e.g. number, length, location, exposure to potentially hazardous substances) are also linked. Health records from the Military Health System Data Repository (MDR) and VA health records (e.g. inpatient and outpatient health care utilization, pharmacy records, vaccinations), vital status/death records from several sources, and DoD survey data (e.g. Recruit Assessment Program surveys and surveys from select Study participant spouses enrolled in the Millennium Cohort Family Study) have been linked to survey data and are available for analyses. A detailed listing of integrated external data sources is included in Table 3.
Established data linkages
| Type of data | Data source |
|---|---|
| Sociodemographic data (e.g. age, race, ethnicity, education) |
|
| Military service characteristics [e.g. deployment, service branch, occupation, service status (active, regular, reserve, separated), rank and service history, including deployment] |
|
| Military health care (utilization, inpatient and outpatient, pharmacy, immunizations) |
|
| Deployment data (e.g. duration of deployment, injury) |
|
| Occupational and environmental exposures |
|
| Serum specimens (e.g. collected for military HIV antibody testing). |
|
| DoD Survey (e.g. spouse data) |
|
| Social and built-environment data (e.g. demographic, socioeconomic, other community attributes of where participants reside or work) |
|
| Vital status and cause of death |
|
| Veteran health care (e.g. utilization, inpatient and outpatient, pharmacy, disability records, benefits) |
|
| Type of data | Data source |
|---|---|
| Sociodemographic data (e.g. age, race, ethnicity, education) |
|
| Military service characteristics [e.g. deployment, service branch, occupation, service status (active, regular, reserve, separated), rank and service history, including deployment] |
|
| Military health care (utilization, inpatient and outpatient, pharmacy, immunizations) |
|
| Deployment data (e.g. duration of deployment, injury) |
|
| Occupational and environmental exposures |
|
| Serum specimens (e.g. collected for military HIV antibody testing). |
|
| DoD Survey (e.g. spouse data) |
|
| Social and built-environment data (e.g. demographic, socioeconomic, other community attributes of where participants reside or work) |
|
| Vital status and cause of death |
|
| Veteran health care (e.g. utilization, inpatient and outpatient, pharmacy, disability records, benefits) |
|
Established data linkages
| Type of data | Data source |
|---|---|
| Sociodemographic data (e.g. age, race, ethnicity, education) |
|
| Military service characteristics [e.g. deployment, service branch, occupation, service status (active, regular, reserve, separated), rank and service history, including deployment] |
|
| Military health care (utilization, inpatient and outpatient, pharmacy, immunizations) |
|
| Deployment data (e.g. duration of deployment, injury) |
|
| Occupational and environmental exposures |
|
| Serum specimens (e.g. collected for military HIV antibody testing). |
|
| DoD Survey (e.g. spouse data) |
|
| Social and built-environment data (e.g. demographic, socioeconomic, other community attributes of where participants reside or work) |
|
| Vital status and cause of death |
|
| Veteran health care (e.g. utilization, inpatient and outpatient, pharmacy, disability records, benefits) |
|
| Type of data | Data source |
|---|---|
| Sociodemographic data (e.g. age, race, ethnicity, education) |
|
| Military service characteristics [e.g. deployment, service branch, occupation, service status (active, regular, reserve, separated), rank and service history, including deployment] |
|
| Military health care (utilization, inpatient and outpatient, pharmacy, immunizations) |
|
| Deployment data (e.g. duration of deployment, injury) |
|
| Occupational and environmental exposures |
|
| Serum specimens (e.g. collected for military HIV antibody testing). |
|
| DoD Survey (e.g. spouse data) |
|
| Social and built-environment data (e.g. demographic, socioeconomic, other community attributes of where participants reside or work) |
|
| Vital status and cause of death |
|
| Veteran health care (e.g. utilization, inpatient and outpatient, pharmacy, disability records, benefits) |
|
What has it found? Key findings and publications
Since the Study’s inception, over 150 peer-reviewed publications have reported findings from longitudinal and cross-sectional studies of physical health outcomes (e.g. chronic disease and injury), psychological health outcomes (e.g. PTSD, depression and anger), health-related behaviours (e.g. sleep, alcohol and tobacco use), and other priority concerns including sexual trauma and intimate partner violence. Whereas it is beyond the scope of this report to summarize scientific findings in detail, a comprehensive review of the findings from the first 20 years of the Study was recently published.24
A main impetus of the Study’s research is to contribute to policies and programmes that improve service member and veteran health and wellbeing. For example, in 2020, the National Academies of Science, Engineering and Medicine published a report on exposures to airborne hazards and respiratory outcomes among service members who deployed to the Persian Gulf region and Afghanistan. The report summarized findings across multiple studies, including this Study, and developed recommendations for future research and policies related to respiratory health.25 In addition, the Study’s findings on respiratory hazards during deployment informed policy updates regarding VA disability claims for ‘asthma, rhinitis, and sinusitis based on presumed particulate matter exposures during military service in Southwest Asia and certain other areas if these conditions manifested within 10 years of a qualifying period of military service’.26 Another example of how the Study contributed to policy was in response to section 748 of the 2020 NDAA (Public Law 116–92)27 which required reports on gynaecological and perinatal health of service women enrolled in the Millennium Cohort Study. In addition to these health concerns, the Study continues to track how results in other programmatic areas have been disseminated to stakeholders and inform programmes and policies.
What are the main strengths and weaknesses?
Due in part to the sample size and prospective design, the Study is well-positioned to describe occupational and social determinants of health, including economic, career and family-related factors that may positively or negatively affect health and wellbeing over time. The Study is unique in having a diverse cohort from all service branches and components and in collecting data on service members even after they separate from the military. Another notable strength is the ability to integrate survey data with other data sources.
Despite these strengths, the Study has some limitations that warrant mention. As with general survey research, the Study may be subject to non-response bias, which may influence interpretation and generalizability of results. Approximately 20% of those invited to participate in the Study have enrolled. Panel 1 was a probability-based sample of the entire military population at enrolment, and Panels 2 through 5 were random samples of personnel with 1 to 5 years of military service (Figure 2). Previous research indicated that Panel 1 was representative of the overall military at baseline, indicating that findings are generalizable to the military at large,28 whereas subsequent Panels 2 and 3 had greater enrolment among those with deployment experience and more recent outpatient health care visits, and less enrolment among those with more inpatient hospitalizations and mental disorders.29 Efforts to examine generalizability of Panels 4 and 5 are forthcoming. Response rates to the Study’s follow-up surveys over time have historically been approximately 60% (range 43–71%), which is comparable to other occupational cohort studies such as the California Teachers Study that had a 20-year follow-up response rate of ∼40%.30 A recent examination of multiple exposure-outcome associations employed methods to correct for missing data in the Study and suggested minimal differences between effect estimates derived from complete case analyses and analyses weighted for non-response.31 In addition, the Study employs participant engagement and retention efforts32 to address concern about initial Study enrolment and response to follow-up surveys.
Can I get hold of the data? Where can I find out more?
Guidelines for collaborative research can be found on the Study’s website [www.millenniumcohort.org]. New collaborators will be asked to submit a one-page research overview to assess initial feasibility and capability to address the research topic. Research proposals developed in consultation with the research team are reviewed by a scientific oversight committee to ensure alignment with the objectives of the Study. Upon approval of a research proposal, institutional review board protocols and data-sharing agreements must be established. Investigators interested in obtaining further information on initiating collaborative research with the Millennium Cohort Study are invited to refer to the website and contact the principal investigator at [usn.point-loma.navhlthrschcensan.mbx.nhrc-millennium-cohort-pi@health.mil].
Millenium Cohort Study team additional members
Additional members of the Millennium Cohort Study team: Anna Baccetti, Anna Bukowinski, Toni Rose Geronimo-Hara, Clinton Hall, Judith Harbertson, David Moreno Ignacio, Aprilyn Piega, Neika Sharifian, Steven Speigle, Daniel Trone, Javier Villalobos, Katie Zhu, Erin Hoffman, Lynne Liu and Elaine Hu.
Ethics approval
The study protocol is approved by the Naval Health Research Center Institutional Review Board and VA Puget Sound IRB, in compliance with all applicable Federal regulations governing the protection of human subjects. Research data are derived from an approved Naval Health Research Center Institutional Review Board protocol number NHRC.2000.0007.
Data availability
The datasets generated and/or analysed during the current study are not publicly available due to security protocols and privacy regulations, but limited de-identified datasets may be made available on reasonable request by the contacting the study principal investigator. See ‘Can I get hold of the data?’ above.
Author contributions
Concept and design: S.F.C., J.N.B., I.G.J., C.A.K., R.P.R., E.J.B., M.A.R. Acquisition, analysis or interpretation of data: S.F.C., J.N.B., C.A.K., I.G.J., C.A.L., J.L.W., B.D.S., R.P.R., E.J.B., A.C.R., M.A.R. Drafting of the manuscript: S.F.C., J.N.B., C.A.K., C.A.L., R.P.R. Critical revision of the manuscript for important intellectual content: S.F.C., J.N.B., C.A.K., I.G.J., C.A.L., A.C.R., J.L.W., B.D.S., F.R.C., E.J.B., R.P.R., M.A.R. Statistical analysis: C.A.K., A.C.R., S.B. Obtained funding: R.P.R., E.J.B. Administrative, technical or material support: J.L.W., B.D.S., R.P.R. Supervision: I.G.J., R.P.R.
Funding
The Millennium Cohort Study is funded through the Military Operational Medicine Research Program (MOMRP), Defense Health Program and Department of Veterans Affairs. R.P.R., S.F.C., J.N.R., F.R.C., M.A.R. and E.J.B. are military service members or employees of the US government. This work was prepared as part of our official duties. Title 17, USC §105 provides that copyright protection under this title is not available for any work of the US government. Title 17, USC §101 defines a US government work as that prepared by a military service member or employee of the US government as part of that person’s official duties. Report 22–87 was supported by the MOMRP, Defense Health Program and the Department of Veterans Affairs under work unit No. 60002. The views expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Department of the Navy, Department of Defense, Department of Veterans Affairs or the US government.
Acknowledgements
The authors appreciate contributions from the Deployment Health Research Department, Millennium Cohort Family Study, Study of Adolescent Resilience, Birth and Infant Health Research Team and Leidos Inc. We greatly appreciate the contributions of the Millennium Cohort Study participants. Finally, we are greatly indebted to the team of founding investigators (Dr Gregory Gray, Dr Margaret A K Ryan, Dr Edward Boyko, Dr Rick Riddle, Dr Timothy Wells, Dr Paul Amoroso, Dr Tomoko Hooper, and Dr Gary Gackstetter) whose foresight laid the framework for the Study’s continued success.
Conflict of interest
None declared.
References
Library of Congress. Strom Thurmond National Defense Authorization Act for Fiscal Year 1999. Public Law 105–261, H.R. 3616, 105th Congress (1997–1998). Retrieved August 1, 2022 from: https://www.congress.gov/bill/105th-congress/house-bill/3616/text.
Library of Congress. National Defense Authorization Act for Fiscal Year 2020. Sec. 748. Reports on Millennium Cohort Study relating to women members of the Armed Forces. In: 116th Congress, ed. Public Law 116–922019. Retrieved August 1, 2022 from https://www.congress.gov/116/plaws/publ92/PLAW-116publ92.pdf


{kind=link}
{kind=link}