






This report describes an approach for the treatment of high-risk native mitral valve stenosis. It incorporates the deployment of a transcatheter valve in the mitral position under full endoscopic vision, combined with endoscopic mitral repair techniques that secure valve positioning and reduce the risk of paravalvular leak. This approach could be used as a rescue procedure in centres with experience in transcatheter and endoscopic valve techniques.
INTRODUCTION
Fully endoscopic mitral valve repair surgery and transcatheter mitral valve replacement are two different treatment strategies for the management of mitral valve disease. We present a case where these two strategies are combined and supplement each other for the treatment of native mitral valve stenosis.
MATERIALS AND METHODS
An 86-year old lady was admitted with recurrent episodes of breathlessness. She had a history of chronic kidney disease and previous aortic valve replacement with bioprosthesis combined with a single coronary artery bypass vein graft.
Transthoracic echocardiography revealed severe mitral stenosis (mean gradient: 16 mmHg, mitral valve area: 0.7 cm2). There was moderate mitral insufficiency, mild biventricular dysfunction and evidence of pulmonary hypertension. The mitral valve annulus and subvalvular apparatus appeared to be severely calcified. Coronary angiography showed patent vein graft. Taking into consideration our unit's experience in reoperative endoscopic mitral valve surgery [1] as well as the patient's clinical condition, age and frailty, a decision was reached for her disease to be treated in a less invasive setting.
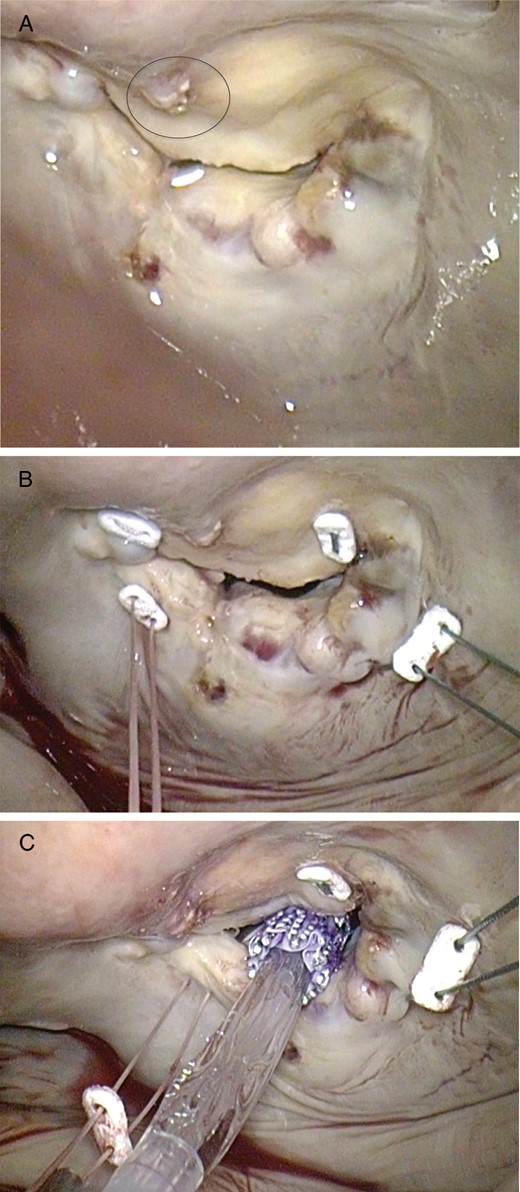
Intraoperative images taken with the endoscope. (A) View of the mitral valve. The severe calcification of the posterior annulus as well as the protruding strut of the aortic bioprosthesis (circle) can be appreciated. (B) Placement of one pledgeted polyfilament annuloplasty U-suture in each commissure. (C) Introduction and placement of the transcatheter aortic valve.
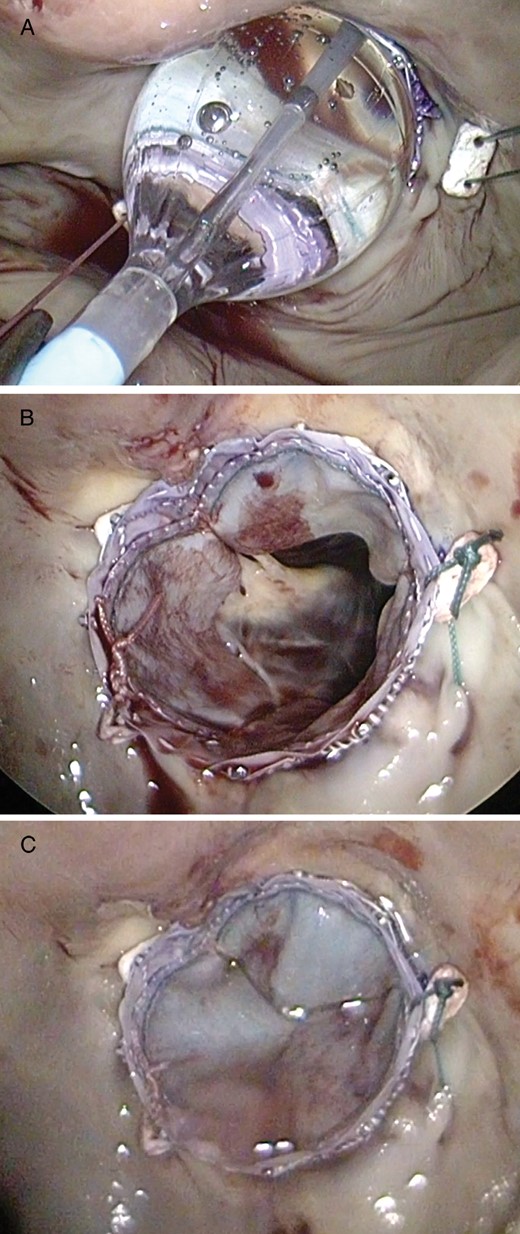
Intraoperative images taken with the endoscope. (A) Balloon inflation and deployment of the transcatheter valve. (B) Valve inspection after deployment. (C) Assessment of the result after water testing.
RESULTS
Postoperative echocardiography confirmed optimal valve placement with no paravalvular leak. The patient was extubated 6 h after surgery. Her initial recovery was uneventful. Two months later, however, and despite the fact she was rehabilitating well, she passed away after a severe lung infection. During these events, transthoracic echocardiography confirmed a well-seated prosthesis with no paravalvular leaks and preserved left ventricular function.
DISCUSSION
Minimally invasive native mitral valve surgery can be performed by different approaches. Endoscopic non-rib spreading procedures are well established for complex mitral valve repairs and replacements [1]. Transcatheter mitral valve implantation has also been described. The valve can be delivered through the apex of the heart [2], through the left atrium under direct vision [3], through sternotomy [4] or using a robotic system [5]. Our report suggests that a combination of fully endoscopic and transcatheter techniques can be employed for the treatment of native mitral valve stenosis, particularly in patients with high technical and surgical risk where an extensive decalcification of the annulus could be more risky than beneficial. Endoscopic procedures offer optimal vision and the option of simultaneous additional repair techniques, without the cost of robotic consoles. They have, therefore, a role as they can optimize valve placement and reduce the risk of paravalvular leak; therefore, they should be considered in this group of patients.
Conflict of interest: none declared.

{kind=link}