





Abstract
The Policy Evaluation Network proposes a consolidated approach to measure comparable health indicators across European health surveillance systems to evaluate effectiveness of policy action.
In a stepwise approach, questionnaire items used by the systems for measuring diet and physical activity data to describe health indicators were identified based on their validity, reliability, and suitability to monitor achievement of health recommendations. They were collated to unified questionnaire modules and discussed bilaterally with representatives of these systems to explore barriers and facilitators for implementation. Also, establishment of a methodological competence platform was proposed, in which the surveillance and monitoring systems agree on the priorities and common quality standards for the harmonization process and to coordinate the integration of questionnaire modules into existing systems.
In total, seven questionnaire modules were developed, of which two diet and two physical activity modules were proposed for implementation. Each module allows measurement of data reflecting only partial aspects of national and WHO recommendations related to diet and physical activity. Main barriers were the requirements of systems to monitor temporal trends and to minimize costs. Main facilitator for implementation was the systems’ use of questionnaire items that were comparable to the unified modules. Representatives agreed to participate in a methodological competence platform.
We successfully took first steps in the realization of the roadmap towards a harmonization of European surveillance by introducing unified questionnaire modules allowing the collection of comparable health indicators and by initiating the establishment of a competence platform to guide this process.
Introduction
Healthy lifestyles are integral to achieving the Sustainable Development Goals (SDGs).1 To evaluate the effectiveness of policies promoting healthy lifestyles, the European member states depend on the regular supply of data on the population’s health and related behaviours. The collection of data describing health behaviour indicators should ideally be carried out in a harmonized manner.2,3 The ultimate aim is to improve data harmonization in a concerted approach, ensuring the comparability of indicators between the regional, national, and international surveillance systems while maintaining the integrity of the participating surveillance systems.4 If possible, the harmonization process is guided by an overarching methodological competence platform, similar to the structure proposed by EuroDish5; it involves representatives of surveillance and monitoring systems and research institutions and intends to connect state-of-the-art research with cross-country health monitoring. The basis for such an approach was developed by the Determinants of Diet and Physical Activity (DEDIPAC) Consortium,6 including a participatory process with representatives of international and regional European surveillance systems. Systems were identified through an inventory3 and deemed suitable if they either provided state-of-the-art instruments to measure physical activity and dietary behaviours or had already created a pan-European infrastructure. The Joint Programming Initiative ‘A Healthy Diet for a Healthy Life’ funded Policy Evaluation Network (PEN)7 proceeds with this roadmap to establish the stepwise alignment of European surveillance systems, covering different age groups: The WHO European Childhood Obesity Surveillance Initiative (COSI; children 6–9 years),8 WHO Health Behaviour in School-Aged Children (HBSC; adolescents 11, 13, and 15 years),9 WHO STEPwise approach to Surveillance (STEPS; adult population),10 Nordic Monitoring of Diet, Physical Activity and Overweight (NORMO; young and adult population aged 7–12 years and 18–65 years),11 and the European Health Interview Survey (EHIS; adolescent and adult population from 15 years onwards).12 This publication describes the first steps of the harmonization roadmap6:
The development of short and uniform questionnaire modules for use in future waves of surveillance systems;
The barriers and facilitators to their implementation;
The establishment of a methodological competence platform to coordinate and sustain the methodological advancement and harmonization across the systems.
Methods
Development of harmonized questionnaire modules
Harmonized questionnaire modules were developed in a four-step process; step one, two and three were previously described.13,14 In the first step, PEN researchers identified key indicators for dietary behaviour, physical activity and sedentary behaviours from: (i) published systematic literature research (e.g. from the DEDIPAC project),15–17 (ii) public health frameworks with a focus on health promotion and obesity prevention, such as the Global Action Plan on Physical Activity or the International Network for Food and Obesity/non-communicable diseases Research, Monitoring and Action Support,17–20 and (iii) the European Core Health Indicators.21 During a Delphi-like expert consultation, key indicators were then prioritized in three stages, considering their relevance for assessing achievement of policy goals, like the SDGs,1 and their current or potential adoption by European surveillance systems to evaluate effectiveness of policy action.13 The consulted panel included 25 PEN researchers and 15 external experts on monitoring health behaviour indicators at the European level: WHO, OECD, European Commission, World Cancer Research Fund and representatives of the European surveillance and monitoring systems identified in the DEDIPAC inventory.3
In the second step, prioritized indicators were assigned to different levels of the socio-ecological model: Policy, community, organizational, interpersonal, and individual level.22
In the third step, these indicators were mapped onto variables provided by 17 monitoring and surveillance systems.14 Included were systems providing data suitable to describe the indicators, and information on previous survey dates, geographical coverage, and data availability. Based on these criteria, the surveillance systems from the DEDIPAC inventory3 were identified and complemented by, e.g. Eurobarometer, WHO Global Nutrition Policy Review, WHO NCD Country Capacity Survey, and the EU Physical Activity Monitoring Framework. Survey databases, handbooks, and questionnaires used in the most recent survey waves were systematically searched for variables that can describe the indicators on the priority list. Not all prioritized indicators could be matched with variables, explaining existing gaps in upstream level data.14
In the fourth step, the focus of this paper, we grouped policy level indicators in domains13 and selected the top six domains for which indicators of high priority were available at the socio-ecological levels. These six domains were developed further and focused on diet and physical activity rather than sedentary behaviour indicators, which were previously ranked lowest. Questionnaire items used to measure the respective indicators were identified, considering their validity, reliability, and their suitability to measure adherence to the WHO recommendations as selection criteria (Supplementary table S1). Robustness of items in a cross-country context was ensured by the selection of items from the systems’ established instrument catalogues. Aligning the identified questionnaire items to the domain-specific indicators originated sets of unified questionnaire modules: Selected Instruments for Multilevel PoLicy and impact Evaluation (SIMPLE) modules.23 In total, seven SIMPLE modules were developed: Food Provision, Food Promotion, and Food Prices as well as Physical Activity Recommendations, Cycling and Walking, and Physical Activity at (Primary or Secondary) School. To improve monitoring of socio-economic disparities,9 an additional equity module was developed for collecting inequality indicators for dietary behaviour.
Consultation process
Key representatives of five multi-national surveillance systems (COSI, HBSC, NORMO, EHIS, and STEPS) were consulted in bilateral video conferences in 2021 to discuss the feasibility to include one or more of the SIMPLE modules in future data collection waves and to identify possible implementation barriers and facilitators. They were also asked if they were interested in becoming an active member of a methodological competence platform. To keep the first harmonization step focused, only the SIMPLE modules Food Prices and Food Promotion as well as Physical Activity Recommendations and Cycling and Walking were suggested for implementation at this point. The choice fell on those modules with most complete indicators at the socio-ecological levels, leaving the least data gaps. To prepare for the consultation, each representative received the underlying DEDIPAC framework,6 the SIMPLE modules, and pre-defined questions to prepare for discussion.
Each consultation concluded with the presentation of the aims and structure of the envisaged methodological competence platform and an invitation to join or to nominate an expert. Consultations were recorded, transcribed and the summaries of main agreements were sent back to the representatives to invite feedback and to obtain final approval.
Results
Description of SIMPLE modules
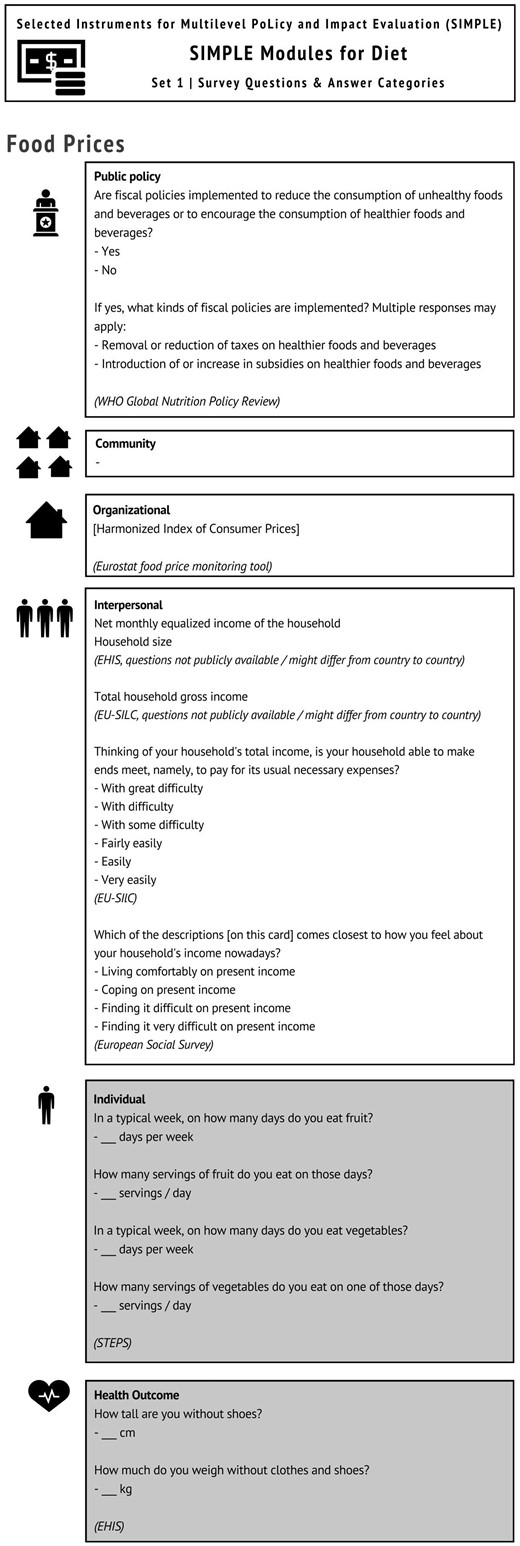
The individual level questionnaire items of the Food Prices and Food Provision SIMPLE modules measure fruit and vegetable intake according to the STEPS questionnaire.24 They allow measuring consumption frequency and serving size of fruits and of vegetables separately, which is relevant for monitoring the WHO recommendations (400 g of fruit and vegetable/day or five portions/day).25 Some indicators were used in several modules; for instance, fruit and vegetable consumption was highly ranked and therefore prioritized as an indicator of healthy dietary behaviour in both the Food Prices and Food Provision modules.
The individual level questionnaire items of the Food Promotion module measure consumption frequency of sugar-sweetened beverages (SSBs) and ultra-processed snack foods from HBSC and COSI, respectively8,9 (table 1). The Food Prices module is presented as an example (figure 1).
Content of SIMPLE module: Food Prices (Example)
Detailed information on SIMPLE modules for dietary behaviour
| Level | Indicator | Survey question [and answer categories] | EU monitoring system/database | A Data gathered from…B ValidationC Proportion of individuals meeting WHO recommendation(s) |
|---|---|---|---|---|
| Food prices | ||||
| Public policy | Taxes or levies on unhealthy foods and beverages (e.g. sugar-sweetened beverages, foods high in nutrients of concern) are in place and increase the retail prices of these foods to discourage unhealthy food choices where possible. |
| WHO Global Nutrition Policy Review |
|
| Community | – | – | – | – |
| Organizational | Relative/absolute cost of healthy and unhealthy foodsa | [Harmonized Index of Consumer Prices] | Eurostat food price monitoring tool |
|
| Interpersonal | Relative household income (household income/household size) |
| EHIS (questions not publicly available/might differ from country to country) |
|
| EU-SILC (questions not publicly available/might differ from country to country) |
| ||
| Financial strain |
| EU-SILC |
| |
| European Social Survey |
| ||
| Individuals | Fruit intake, number of portions per day | STEPS | ||
| Vegetable intake, number of portions per day | STEPS | |||
| Health outcome | BMI | How tall are you without shoes? -___ cm How much do you weigh without clothes and shoes? -___ kg | EHIS | |
| Food promotion (children and adolescents) | ||||
| Public policy | Governmental policies are implemented to restrict commercial marketing (including sponsorship, promotion and advertisement) of unhealthy foods and beverages to children, including adolescents, in settings where children gather (e.g. pre-schools, schools, sports clubs and facilities and cultural events).a | Are school health and nutrition policies, programs or related standards being implemented? [Yes/No] | WHO Global Nutrition Policy Review |
|
| Community | Exposure to food adverts for unhealthy food and beverages through all media and marketing channels.a |
| WHO Global Nutrition Policy Review |
|
| Organizational | School Food Environment |
| COSI |
|
| Interpersonal | – | – | – | – |
| Individuals | Sugar-sweetened beverages, glasses per day |
| HBSC | |
| Consumption frequency/day of ultra-processed snack food* | COSI |
| ||
| Health outcome | BMI | How tall are you without shoes? -___ cm How much do you weigh without clothes and shoes? -___ kg | EHIS | |
| Food promotion (adults) | ||||
| Public policy | Governmental policies are implemented to support social marketing and fund campaigns to promote healthy and sustainable eating. |
| WHO Global Nutrition Policy Review |
|
| Community | – | – | – | – |
| Organizational | – | – | – | – |
| Interpersonal | – | – | – | – |
| Individuals | Sugar-sweetened beverages, glasses per day |
| HBSC | |
| Consumption frequency/day of ultra-processed snack fooda | COSI |
| ||
| Health outcome | BMI |
| EHIS | |
| Level | Indicator | Survey question [and answer categories] | EU monitoring system/database | A Data gathered from…B ValidationC Proportion of individuals meeting WHO recommendation(s) |
|---|---|---|---|---|
| Food prices | ||||
| Public policy | Taxes or levies on unhealthy foods and beverages (e.g. sugar-sweetened beverages, foods high in nutrients of concern) are in place and increase the retail prices of these foods to discourage unhealthy food choices where possible. |
| WHO Global Nutrition Policy Review |
|
| Community | – | – | – | – |
| Organizational | Relative/absolute cost of healthy and unhealthy foodsa | [Harmonized Index of Consumer Prices] | Eurostat food price monitoring tool |
|
| Interpersonal | Relative household income (household income/household size) |
| EHIS (questions not publicly available/might differ from country to country) |
|
| EU-SILC (questions not publicly available/might differ from country to country) |
| ||
| Financial strain |
| EU-SILC |
| |
| European Social Survey |
| ||
| Individuals | Fruit intake, number of portions per day | STEPS | ||
| Vegetable intake, number of portions per day | STEPS | |||
| Health outcome | BMI | How tall are you without shoes? -___ cm How much do you weigh without clothes and shoes? -___ kg | EHIS | |
| Food promotion (children and adolescents) | ||||
| Public policy | Governmental policies are implemented to restrict commercial marketing (including sponsorship, promotion and advertisement) of unhealthy foods and beverages to children, including adolescents, in settings where children gather (e.g. pre-schools, schools, sports clubs and facilities and cultural events).a | Are school health and nutrition policies, programs or related standards being implemented? [Yes/No] | WHO Global Nutrition Policy Review |
|
| Community | Exposure to food adverts for unhealthy food and beverages through all media and marketing channels.a |
| WHO Global Nutrition Policy Review |
|
| Organizational | School Food Environment |
| COSI |
|
| Interpersonal | – | – | – | – |
| Individuals | Sugar-sweetened beverages, glasses per day |
| HBSC | |
| Consumption frequency/day of ultra-processed snack food* | COSI |
| ||
| Health outcome | BMI | How tall are you without shoes? -___ cm How much do you weigh without clothes and shoes? -___ kg | EHIS | |
| Food promotion (adults) | ||||
| Public policy | Governmental policies are implemented to support social marketing and fund campaigns to promote healthy and sustainable eating. |
| WHO Global Nutrition Policy Review |
|
| Community | – | – | – | – |
| Organizational | – | – | – | – |
| Interpersonal | – | – | – | – |
| Individuals | Sugar-sweetened beverages, glasses per day |
| HBSC | |
| Consumption frequency/day of ultra-processed snack fooda | COSI |
| ||
| Health outcome | BMI |
| EHIS | |
Only partial fit of indicator and survey question.
Serving size: 1 apple, 1 banana, 1 orange, ½ cup cooked or chopped fruit (80 g), ½ cup fruit juice. Examples: fruit and berries include fresh, frozen, canned, glassed/potted etc.; e.g. an apple, an orange, a banana, a bunch of grapes, a plate of strawberries or fruit and berries that are part of porridge, fruit stew, or fruit salad etc.24
Serving size: 1 cup of raw green leafy vegetables (spinach, salad), ½ cup other vegetables, cooked or chopped raw (tomatoes, carrots, pumpkins, corn, Chinese cabbage, fresh beans, onion, etc.), ½ cup vegetable juice. Examples: vegetables, pulses and/or root fruits include fresh, frozen, canned, glass/potted etc.; e.g. carrots, tomatoes, cucumber, broccoli, peppers, salad, beans, chick peas, lentils, beetroot, celery and parsnip.24
Validated questions different compared with those of STEPS, including time frame and using answer categories.
Examples: energy drinks, red bull, ice tea,…11
Examples: potato crisps, salted popcorn, salted nuts, savoury biscuits and/or pretzels).11
Detailed information on SIMPLE modules for dietary behaviour
| Level | Indicator | Survey question [and answer categories] | EU monitoring system/database | A Data gathered from…B ValidationC Proportion of individuals meeting WHO recommendation(s) |
|---|---|---|---|---|
| Food prices | ||||
| Public policy | Taxes or levies on unhealthy foods and beverages (e.g. sugar-sweetened beverages, foods high in nutrients of concern) are in place and increase the retail prices of these foods to discourage unhealthy food choices where possible. |
| WHO Global Nutrition Policy Review |
|
| Community | – | – | – | – |
| Organizational | Relative/absolute cost of healthy and unhealthy foodsa | [Harmonized Index of Consumer Prices] | Eurostat food price monitoring tool |
|
| Interpersonal | Relative household income (household income/household size) |
| EHIS (questions not publicly available/might differ from country to country) |
|
| EU-SILC (questions not publicly available/might differ from country to country) |
| ||
| Financial strain |
| EU-SILC |
| |
| European Social Survey |
| ||
| Individuals | Fruit intake, number of portions per day | STEPS | ||
| Vegetable intake, number of portions per day | STEPS | |||
| Health outcome | BMI | How tall are you without shoes? -___ cm How much do you weigh without clothes and shoes? -___ kg | EHIS | |
| Food promotion (children and adolescents) | ||||
| Public policy | Governmental policies are implemented to restrict commercial marketing (including sponsorship, promotion and advertisement) of unhealthy foods and beverages to children, including adolescents, in settings where children gather (e.g. pre-schools, schools, sports clubs and facilities and cultural events).a | Are school health and nutrition policies, programs or related standards being implemented? [Yes/No] | WHO Global Nutrition Policy Review |
|
| Community | Exposure to food adverts for unhealthy food and beverages through all media and marketing channels.a |
| WHO Global Nutrition Policy Review |
|
| Organizational | School Food Environment |
| COSI |
|
| Interpersonal | – | – | – | – |
| Individuals | Sugar-sweetened beverages, glasses per day |
| HBSC | |
| Consumption frequency/day of ultra-processed snack food* | COSI |
| ||
| Health outcome | BMI | How tall are you without shoes? -___ cm How much do you weigh without clothes and shoes? -___ kg | EHIS | |
| Food promotion (adults) | ||||
| Public policy | Governmental policies are implemented to support social marketing and fund campaigns to promote healthy and sustainable eating. |
| WHO Global Nutrition Policy Review |
|
| Community | – | – | – | – |
| Organizational | – | – | – | – |
| Interpersonal | – | – | – | – |
| Individuals | Sugar-sweetened beverages, glasses per day |
| HBSC | |
| Consumption frequency/day of ultra-processed snack fooda | COSI |
| ||
| Health outcome | BMI |
| EHIS | |
| Level | Indicator | Survey question [and answer categories] | EU monitoring system/database | A Data gathered from…B ValidationC Proportion of individuals meeting WHO recommendation(s) |
|---|---|---|---|---|
| Food prices | ||||
| Public policy | Taxes or levies on unhealthy foods and beverages (e.g. sugar-sweetened beverages, foods high in nutrients of concern) are in place and increase the retail prices of these foods to discourage unhealthy food choices where possible. |
| WHO Global Nutrition Policy Review |
|
| Community | – | – | – | – |
| Organizational | Relative/absolute cost of healthy and unhealthy foodsa | [Harmonized Index of Consumer Prices] | Eurostat food price monitoring tool |
|
| Interpersonal | Relative household income (household income/household size) |
| EHIS (questions not publicly available/might differ from country to country) |
|
| EU-SILC (questions not publicly available/might differ from country to country) |
| ||
| Financial strain |
| EU-SILC |
| |
| European Social Survey |
| ||
| Individuals | Fruit intake, number of portions per day | STEPS | ||
| Vegetable intake, number of portions per day | STEPS | |||
| Health outcome | BMI | How tall are you without shoes? -___ cm How much do you weigh without clothes and shoes? -___ kg | EHIS | |
| Food promotion (children and adolescents) | ||||
| Public policy | Governmental policies are implemented to restrict commercial marketing (including sponsorship, promotion and advertisement) of unhealthy foods and beverages to children, including adolescents, in settings where children gather (e.g. pre-schools, schools, sports clubs and facilities and cultural events).a | Are school health and nutrition policies, programs or related standards being implemented? [Yes/No] | WHO Global Nutrition Policy Review |
|
| Community | Exposure to food adverts for unhealthy food and beverages through all media and marketing channels.a |
| WHO Global Nutrition Policy Review |
|
| Organizational | School Food Environment |
| COSI |
|
| Interpersonal | – | – | – | – |
| Individuals | Sugar-sweetened beverages, glasses per day |
| HBSC | |
| Consumption frequency/day of ultra-processed snack food* | COSI |
| ||
| Health outcome | BMI | How tall are you without shoes? -___ cm How much do you weigh without clothes and shoes? -___ kg | EHIS | |
| Food promotion (adults) | ||||
| Public policy | Governmental policies are implemented to support social marketing and fund campaigns to promote healthy and sustainable eating. |
| WHO Global Nutrition Policy Review |
|
| Community | – | – | – | – |
| Organizational | – | – | – | – |
| Interpersonal | – | – | – | – |
| Individuals | Sugar-sweetened beverages, glasses per day |
| HBSC | |
| Consumption frequency/day of ultra-processed snack fooda | COSI |
| ||
| Health outcome | BMI |
| EHIS | |
Only partial fit of indicator and survey question.
Serving size: 1 apple, 1 banana, 1 orange, ½ cup cooked or chopped fruit (80 g), ½ cup fruit juice. Examples: fruit and berries include fresh, frozen, canned, glassed/potted etc.; e.g. an apple, an orange, a banana, a bunch of grapes, a plate of strawberries or fruit and berries that are part of porridge, fruit stew, or fruit salad etc.24
Serving size: 1 cup of raw green leafy vegetables (spinach, salad), ½ cup other vegetables, cooked or chopped raw (tomatoes, carrots, pumpkins, corn, Chinese cabbage, fresh beans, onion, etc.), ½ cup vegetable juice. Examples: vegetables, pulses and/or root fruits include fresh, frozen, canned, glass/potted etc.; e.g. carrots, tomatoes, cucumber, broccoli, peppers, salad, beans, chick peas, lentils, beetroot, celery and parsnip.24
Validated questions different compared with those of STEPS, including time frame and using answer categories.
Examples: energy drinks, red bull, ice tea,…11
Examples: potato crisps, salted popcorn, salted nuts, savoury biscuits and/or pretzels).11
The individual level questionnaire items for the Physical Activity Recommendations and Cycling and Walking SIMPLE modules were taken from EHIS12 and measured data that allow for reflecting only partial aspects of the current WHO recommendations, published in 202032 (table 2).
Detailed information on SIMPLE modules for physical activity
| Level | Indicator | Survey question [and answer categories] | EU monitoring system/database | A Data gathered from…B ValidationC Proportion of individuals meeting WHO recommendation(s) |
|---|---|---|---|---|
| Physical activity recommendations | ||||
| Public policy | National recommendations on physical activity for health |
| WHO NCD Country Capacity Survey |
|
| Community | Proportion of people aware of physical activity programmes organized by the communitya |
| Eurobarometer |
|
| Organizational | Settings included in the delivery of specific health-enhancing physical activity actions | Considering all (…) key physical activity policy documents (…), please indicate which settings are included for the delivery of specific Health-Enhacing Physical Activity actions.
| HEPA PAT |
|
| Interpersonal | Proportion of people who see others being active in their neighbourhooda |
| Eurobarometer |
|
| Individuals | Total time spent with physical activity per week | EHIS |
| |
| EHIS |
| |||
| Cycling and walking | ||||
| Public policy | Government supports the incorporation of walking and cycling infrastructure in urban, rural and transport plansa |
| EU/WHO HEPA Monitoring Framework survey |
|
| Community | Availability and quality of cycling networks/paths/amenities; cycle-friendly infrastructure | [User generated content, e.g. bicycle map, hiking map, wheelchair user map] | Open Street Maps |
|
| Organizational | – | – | – | – |
| Interpersonal | – | – | – | – |
| Individuals | Time spent walking in order to get to and from places in a typical week |
| EHIS |
|
| EHIS |
| ||
| Time spent cycling in order to get to and from places in a typical week |
| EHIS |
| |
| EHIS |
| ||
| Level | Indicator | Survey question [and answer categories] | EU monitoring system/database | A Data gathered from…B ValidationC Proportion of individuals meeting WHO recommendation(s) |
|---|---|---|---|---|
| Physical activity recommendations | ||||
| Public policy | National recommendations on physical activity for health |
| WHO NCD Country Capacity Survey |
|
| Community | Proportion of people aware of physical activity programmes organized by the communitya |
| Eurobarometer |
|
| Organizational | Settings included in the delivery of specific health-enhancing physical activity actions | Considering all (…) key physical activity policy documents (…), please indicate which settings are included for the delivery of specific Health-Enhacing Physical Activity actions.
| HEPA PAT |
|
| Interpersonal | Proportion of people who see others being active in their neighbourhooda |
| Eurobarometer |
|
| Individuals | Total time spent with physical activity per week | EHIS |
| |
| EHIS |
| |||
| Cycling and walking | ||||
| Public policy | Government supports the incorporation of walking and cycling infrastructure in urban, rural and transport plansa |
| EU/WHO HEPA Monitoring Framework survey |
|
| Community | Availability and quality of cycling networks/paths/amenities; cycle-friendly infrastructure | [User generated content, e.g. bicycle map, hiking map, wheelchair user map] | Open Street Maps |
|
| Organizational | – | – | – | – |
| Interpersonal | – | – | – | – |
| Individuals | Time spent walking in order to get to and from places in a typical week |
| EHIS |
|
| EHIS |
| ||
| Time spent cycling in order to get to and from places in a typical week |
| EHIS |
| |
| EHIS |
| ||
Only partial fit of indicator and survey question.
Examples (sports): ball games, athletics, competitive bicycling, running, swimming, etc.35
Examples (fitness): endurance training, strength exercise, flexibility training, etc.35
Examples (recreational activity): nordic walking, brisk walking, ball games, jogging, bicycling, swimming, aerobics, rowing, badminton, etc.35
The time frame of ‘at least 10 minutes’ is no longer recommended in WHO’s Global Physical Activity Guidelines, i.e. a modification of this survey question might be necessary in future.
Applicable to moderate-to-vigorous aerobic recreational activity (minutes per day).
Applicable to walking time (minutes per day).
Applicable to cycling time (minutes per day).
Detailed information on SIMPLE modules for physical activity
| Level | Indicator | Survey question [and answer categories] | EU monitoring system/database | A Data gathered from…B ValidationC Proportion of individuals meeting WHO recommendation(s) |
|---|---|---|---|---|
| Physical activity recommendations | ||||
| Public policy | National recommendations on physical activity for health |
| WHO NCD Country Capacity Survey |
|
| Community | Proportion of people aware of physical activity programmes organized by the communitya |
| Eurobarometer |
|
| Organizational | Settings included in the delivery of specific health-enhancing physical activity actions | Considering all (…) key physical activity policy documents (…), please indicate which settings are included for the delivery of specific Health-Enhacing Physical Activity actions.
| HEPA PAT |
|
| Interpersonal | Proportion of people who see others being active in their neighbourhooda |
| Eurobarometer |
|
| Individuals | Total time spent with physical activity per week | EHIS |
| |
| EHIS |
| |||
| Cycling and walking | ||||
| Public policy | Government supports the incorporation of walking and cycling infrastructure in urban, rural and transport plansa |
| EU/WHO HEPA Monitoring Framework survey |
|
| Community | Availability and quality of cycling networks/paths/amenities; cycle-friendly infrastructure | [User generated content, e.g. bicycle map, hiking map, wheelchair user map] | Open Street Maps |
|
| Organizational | – | – | – | – |
| Interpersonal | – | – | – | – |
| Individuals | Time spent walking in order to get to and from places in a typical week |
| EHIS |
|
| EHIS |
| ||
| Time spent cycling in order to get to and from places in a typical week |
| EHIS |
| |
| EHIS |
| ||
| Level | Indicator | Survey question [and answer categories] | EU monitoring system/database | A Data gathered from…B ValidationC Proportion of individuals meeting WHO recommendation(s) |
|---|---|---|---|---|
| Physical activity recommendations | ||||
| Public policy | National recommendations on physical activity for health |
| WHO NCD Country Capacity Survey |
|
| Community | Proportion of people aware of physical activity programmes organized by the communitya |
| Eurobarometer |
|
| Organizational | Settings included in the delivery of specific health-enhancing physical activity actions | Considering all (…) key physical activity policy documents (…), please indicate which settings are included for the delivery of specific Health-Enhacing Physical Activity actions.
| HEPA PAT |
|
| Interpersonal | Proportion of people who see others being active in their neighbourhooda |
| Eurobarometer |
|
| Individuals | Total time spent with physical activity per week | EHIS |
| |
| EHIS |
| |||
| Cycling and walking | ||||
| Public policy | Government supports the incorporation of walking and cycling infrastructure in urban, rural and transport plansa |
| EU/WHO HEPA Monitoring Framework survey |
|
| Community | Availability and quality of cycling networks/paths/amenities; cycle-friendly infrastructure | [User generated content, e.g. bicycle map, hiking map, wheelchair user map] | Open Street Maps |
|
| Organizational | – | – | – | – |
| Interpersonal | – | – | – | – |
| Individuals | Time spent walking in order to get to and from places in a typical week |
| EHIS |
|
| EHIS |
| ||
| Time spent cycling in order to get to and from places in a typical week |
| EHIS |
| |
| EHIS |
| ||
Only partial fit of indicator and survey question.
Examples (sports): ball games, athletics, competitive bicycling, running, swimming, etc.35
Examples (fitness): endurance training, strength exercise, flexibility training, etc.35
Examples (recreational activity): nordic walking, brisk walking, ball games, jogging, bicycling, swimming, aerobics, rowing, badminton, etc.35
The time frame of ‘at least 10 minutes’ is no longer recommended in WHO’s Global Physical Activity Guidelines, i.e. a modification of this survey question might be necessary in future.
Applicable to moderate-to-vigorous aerobic recreational activity (minutes per day).
Applicable to walking time (minutes per day).
Applicable to cycling time (minutes per day).
For some modules like the Food Promotion module, different versions were provided addressing different settings for policy implementation, such as work place (adults) and school (children, adolescents). The individual level questionnaire item for the Physical Activity at School module was separated into two versions, one for primary school children (reported by parents) and one for secondary school children (self-reported). Generally, individual level questionnaire items are self-reported during Computer Assisted Telephone Interviews (e.g. EHIS, NORMO), self-reported using online questionnaires (eSTEPS app), self-completed in the classroom (e.g. HBSC), or proxy-reported by parents/caregivers (e.g. COSI, NORMO). Variables to describe organizational, community, and policy level indicators are available from national routine monitoring data sets. The SIMPLE modules were developed to facilitate pragmatic implementation of short questionnaire items and not all were validated against a standard measure, e.g. accelerometers. However, a study on the psychometric properties of the EHIS-PAQ, which is comparable to the questionnaire items we selected for the SIMPLE modules, revealed strong to moderate reliability and poor to moderate validity depending on the sub-domains measured33 (Supplementary table S1). The diet questionnaire items were compared against, e.g. a 7-day food diary and a 74-item FFQ. They revealed a strong reliability for fruit, vegetable and SSB intake as well as moderate (for fruits), fair (for vegetables) and strong (for SSB) validity. The domains and sub-domains of the dietary behaviour and physical activity SIMPLE modules differ in nature, as indicators for both behaviours are operationalized differently across European countries and surveillance systems.14 SIMPLE modules are provided on the PEN website.23Supplementary tables S2 and S3 provide the remaining modules. A summary of the consultative process including the systems representatives’ opinion is provided in Supplementary table S4.
Implementation of SIMPLE modules in existing systems and establishment of a methodological competence platform
Fundamental considerations
The SIMPLE modules were developed to provide a first core data set of comparable diet and physical activity indicators as well as body height and weight (for calculating the Body Mass Index, BMI). Ideally, individual level questionnaire items of the SIMPLE modules will be used in next survey waves of the surveillance systems. To start the implementation, it is possible to either introduce the individual level questionnaire items only in voluntary modules, in sub-samples, or to pilot the instruments in national surveys during or between the next survey waves without discarding existing instruments.6
Each SIMPLE module further facilitates identification of routine monitoring data sets providing data on organizational, community, and policy level indicators relevant for one of the six policy domains and the diet module on equity. Hence, researchers, key stakeholders, and policy-makers can use these monitoring data sources to combine national or international data for upstream indicators with newly measured individual level data. Validity and reliability of the selected questionnaire items were discussed critically with all systems as well as their suitability to monitor achievement of WHO recommendations. The concern that measured data can only reflect certain aspects of the WHO recommendations was raised for both, physical activity and diet modules.
Implementation process and methodological competence platform establishment
Implementation of the individual level question of the SIMPLE modules should be supplemented by methodological studies, to further improve and modernize established surveillance questionnaires, because several of them are not ‘fit for purpose’. Questionnaire items that have been introduced decades ago36 may require adaptation to the current recommendations, e.g. for physical activity,32 or to capture changes in circumstances. As an example, variables like ‘Capacity to afford a meal with meat, chicken, fish (or vegetarian equivalent) every second day’ to measure food insecurity (EU-SILC) may no longer be suitable in times of planetary health diets.37
Further studies investigating validity and reliability of questionnaire items in different age groups and—equally important—their suitability to monitor WHO recommendations are needed. As several prioritized indicators could not be matched to variables from existing data sources, the data gaps may be closed with questionnaire items from research studies. To address these methodological challenges, to guide and sustain the harmonization process, and to jointly support and coordinate the necessary methodological developments a methodological competence platform will be established. Besides research institutions the involvement of national and international surveillance systems is desirable. Membership in the methodological competence platform was approved by most representatives (COSI, HBSC, NORMO, STEPS) or will be decided later (EHIS). Platform members meet at regular intervals to agree on the priorities for the harmonization process and common quality standards, to coordinate the necessary action, to propose harmonized surveillance modules for integration into existing systems and to push methodological advancements.6
Piloting the SIMPLE modules
In most systems, formalized processes for changes or extensions of the questionnaires in use are established including steering committees with working groups or sub-committees: The responsible group/committee typically recommends the voluntary piloting of the individual level questionnaire items (such as SIMPLE modules) during the next national survey to the system’s steering group. If the evaluation of the pilot results shows adequate suitability, and improvement to the system’s data sets, their implementation will be suggested for the core (mandatory) questionnaire.
Dietary behaviour
Most surveillance initiatives stated an interest in piloting diet questionnaire items of the Food Prices and Food Promotion modules. This was because they already used the suggested questionnaire item (STEPS, COSI, HBSC) or a comparable instrument, such as a food frequency questionnaire (e.g. NORMO, COSI). Food frequency data can be used to calculate the daily fruit and vegetable intake (g/day) if it includes consumed quantities like in STEPS.10 As NORMO assesses food consumption frequency using the same instruments in children and adults, adherence to the WHO recommendation can be evaluated in both age groups without adding a similar question.
Physical activity
The individual level questionnaire items of the physical activity SIMPLE modules only use parts of validated instruments since the full instruments were considered to be too lengthy and put a high burden on respondents, i.e. the Global Physical Activity Questionnaire. As the SIMPLE modules were less suitable for assessing all aspects of the WHO recommendation, only one system (NORMO) expressed an interest to include the Cycling and Walking SIMPLE module in future waves, but rather as a proxy for measuring sustainable and climate friendly transportation alternatives than for monitoring physical activity of the population.
Body mass index
The BMI was considered as the most appropriate health outcome for the SIMPLE modules. It is either self-reported (HBSC, EHIS, NORMO), or anthropometrically measured in two systems (COSI, STEPS). BMI is assessed in a comparable way by many systems and may thus be considered as an already harmonized indicator across systems and age groups.
Perceived facilitators and barriers of implementation of SIMPLE modules
Facilitators
In general, the systems’ representatives agreed that harmonizing data collection across countries and age groups is desirable and most representatives expressed interest in implementing one or more SIMPLE modules. Of particular interest were the individual level questionnaire items measuring indicators describing sustainability aspects, such as cycling and walking, or fruit and vegetable intake. The systems’ representatives proclaim that implementation could be facilitated if all surveillance systems compromise on one or more unified questionnaire modules. In addition, ongoing harmonization processes within WHO were mentioned as a facilitator: COSI recently started a process to harmonize questionnaire items of the family questionnaire with HBSC.
Barriers
The main concern against the implementation of the SIMPLE modules was the lack of comparability with current data and the objective to monitor temporal trends (all systems). Concerns were also raised regarding the questionnaire length; it is unsuitable to repeat very similar questions and only a limited number of new questions and variables can be added between waves (all systems). Hence, newly introduced instruments need to be broken down to the variable level, with a preference for instruments entailing a small number of variables (EHIS).38 Overall, nationally driven interests related to population health surveillance, such as the need to measure sustainability indicators in future waves must be balanced against limited national resources (NORMO).
Discussion
The DEDIPAC Knowledge Hub developed a roadmap towards a harmonized European surveillance system3,6 and PEN successfully took first steps in its realization.13,14 The SIMPLE modules were proposed for implementation in ongoing surveillance systems during a consultative process. The bilateral consultations revealed a general consensus that the harmonization of data collection is desirable and incorporation of the SIMPLE modules was, in principle, met with approval by most surveillance systems.
Leveraging the facilitators for implementation
Implementation of the modules should be facilitated by the questionnaire items of SIMPLE modules being derived from established surveillance systems. The gained experiences from the pilot studies may guide further adaptations to be tested again in sub-samples until an improved version is provided on a European level. Further, the tendency of systems to keep the list of indicators as stable as possible for trend analyses bears the risk of hampering innovation. However, for different reasons updates of indicators or new measurements may become necessary for the systems. Such reasons include changes to European health surveys, or new relevant public health topics, like climate friendly transportation alternatives39 or sustainable diets.37 However, most surveillance systems make strategic decisions to modernize their assessment methods or questionnaires.40 This is part of the trade-off between the continuation of indicator measures and keeping them up-to-date.
Addressing the barriers for implementation
A critical functionality of surveillance is to measure indicators at a certain moment or over a period of time to monitor changes in prevalence of health status, in habitats, populations, and environments,41 facilitated by repeated standardized surveys.39 The systems’ concern that monitoring trends will be hampered when the new unified questionnaire modules are implemented may be alleviated, as inclusion of questionnaire items without discarding the established systems’ questions will secure the system’s internal integrity and retain their ability to assess temporal trends.6
As the surveillance systems are tightly regulated and will only allow a certain percentage of items to be changed between survey waves, the inclusion of new questionnaire items requires a thorough appraisal.39 As an example, for EHIS surveys, the European Commission allows for a maximum of 10% change between the required variables, and a maximum increase of 5% in the number of variables between EHIS waves 3 and 4, offering a certain degree of flexibility.38 However, any changes in the observed indicator or variable of interest may be explained solely or partly by the change in instruments between survey waves rather than by real changes in health behaviour or health status. This concern may be ruled out as PEN proposed to initially measure indicators using established and uniform questionnaires in parallel, allowing to monitor actual changes. To make sure that these changes are the result of (not) implemented policies, data analysis may apply difference-in-difference design to account for secular trends.42 However, changing the instruments requires a clear purpose for the planned use of the gathered information,43 also to keep the costs at a minimum. In this regard, we have to acknowledge that including the SIMPLE modules will add costs of collection, storage, and analysis of data, unless questionnaires are shortened in other parts. Thus, existing embedded indicators measured insufficiently by poor instruments are the best candidates for replacement. For example, some instruments currently in use to measure physical activity behaviour in everyday life situations (such as mobility and movement patterns, or sedentary and exercise behaviour) have shown low validity.44 The much-needed improvement may be seen in wearable sensors that are increasingly popular in research but not yet implemented in surveillance. Alternatively, valid and robust single-item questions are much shorter compared with established instruments; however, additional methodological studies are required to identify the most reliable and valid question45 that also should serve the purpose to monitor the WHO recommendations.32
The context and political climate in a country may determine what indicators are prioritized and how they are measured. We are just learning this during the COVID-19 pandemic and the projected acute food insecurity due to the war in Ukraine, that new health threats, demographic change, and inequalities in health and healthcare provision in and between EU member states challenge the national health care systems. Thus, to overcome the most urgent public health problems, systemic and integrative approaches are needed, and require responsive and consistent surveillance systems working across national borders.46 This will generate comparable European health data to guide prioritization of health promotion measures, and to raise public and political awareness of the extent of public health problems.43
Health status and health behaviours are largely affected by socio-economic disparities and need to be monitored better across countries and age groups. The diet equity module required further enhancement before implementation since its questionnaire items could only be identified for interpersonal and individual level, leaving data gaps for downstream indicators. Also, developing a physical activity module on equity would be highly relevant; however, current surveillance systems do not measure indicators that would allow mapping out such a module.
In summary, PEN successfully took first steps in the realization of the roadmap towards harmonized European surveillance. Future steps in the harmonization process should not only cover methodological advancement of the SIMPLE modules, or implementation of objective measurements, but also expand usage of the SIMPLE modules by additional national and international surveillance systems. Increasing the comparability of data across surveys, age groups, and countries is essential to evaluate effectiveness of policy action and to inform decision making and appropriate public health action. Improving impact evaluation of health policy interventions in turn will pave the way for healthier food and physical activity environments across Europe.
Supplementary data
Supplementary data are available at EURPUB online.
Acknowledgements
The authors would like to thank all participating experts and representatives of the surveillance and monitoring systems for generously giving their time and contributing their expertise.
Funding
The PEN project (www.jpi-pen.eu) is funded by the Joint Programming Initiative ‘A Healthy Diet for a Healthy Life’ (JPI HDHL), a research and innovation initiative of EU member states and associated countries. The funding agencies supporting this work are (in alphabetical order of participating countries): Germany: Federal Ministry of Education and Research (BMBF); Ireland: Health Research Board (HRB); Norway: The Research Council of Norway (RCN); Poland: The National Centre for Research and Development (NCBR).
Ethics approval and consent to participate
Not applicable.
Conflicts of interest: The authors declare that they have no conflicts of interest.
The Policy Evaluation Network connects the growing scientific interest in investigating interconnections between data—harmonized across several countries—and policies on different levels (e.g. supranational, national, communal) to improve individual health behaviour and inform policies to prevent obesity.
SIMPLE modules collate instruments to harmonize collected data and assess comparable health-related data across European surveillance systems which will facilitate the evaluation of temporal and regional changes in physical activity, dietary behaviour, and associated health outcomes (individual level).
SIMPLE modules aim to measure the impact of national policy action on: (i) individual health and (ii) proximal and distal determinants.
The establishment of a methodological competence platform is a starting point to guide and sustain the harmonization process and the methodological advancement of European health surveillance.
References
Author notes
Wolfgang Ahrens and Celine Murrin contributed equally to this manuscript.

{kind=link}
Comments